


By Dr. Ara Deukmedjian
Board-Certified Neurosurgeon
Medically reviewed on May 28, 2026
Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with a qualified spine specialist about your specific condition and treatment options.
Key Points
✓ “Minimally invasive spine surgery” (MISS) is as much a marketing term as a technical one. It’s an umbrella category, not one procedure, and outcomes vary widely by technique, surgeon, and indication. ¹ ²
✓ On fair comparisons, MISS delivers less blood loss, shorter hospital stays, and lower perioperative complication rates than open surgery, with equivalent or modestly better function at 2–5 years. ³ ⁴ ⁵
✓ At 5 years, MIS-TLIF showed a 2.2% reoperation rate vs. 8.8% for open TLIF, with equivalent pain and disability scores. ⁶ Open surgery also showed more adjacent segment disease at 7 years. ⁷
✓ The label describes the access, not the operation. A minimally invasive fusion is still a fusion. Same hardware, same lost motion, same long-term biology, just a smaller incision.
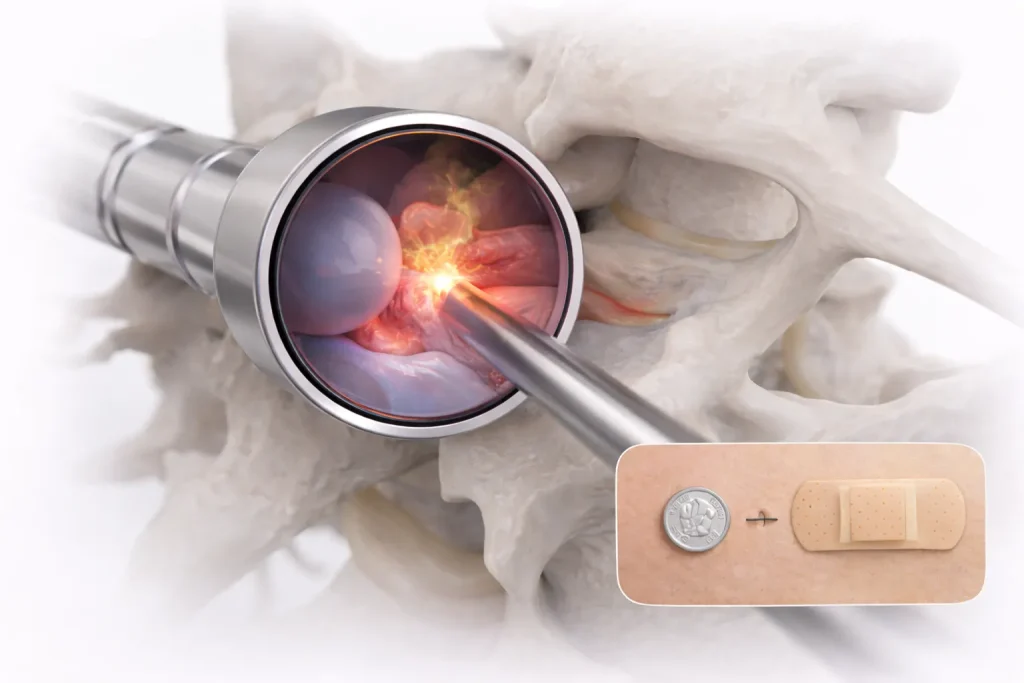
✓ The Deuk Laser Disc Repair® (DLDR) is truly minimally invasive: A 4–7 mm incision, no hardware, no fusion, with a 94.6% published success rate and 99.6% across 2,000+ procedures over 20 years. ⁸ ⁹
✓ The honest answer to “is MISS better?” is: it depends on which procedure, which surgeon, and which patient. The label alone guarantees nothing.

Minimally Invasive Spine Surgery: What The Term Actually Means
“Minimally invasive spine surgery” is one of the most marketed phrases in modern orthopedic medicine. It appears on hospital billboards, in clinic websites, and on the front page of nearly every spine surgery practice that has updated its branding in the last decade. The implication is consistent: smaller incision, faster recovery, better outcomes, less risk.

The actual definition is much looser. MISS is an umbrella term that includes:
- Tubular retractor decompressions
- Percutaneous pedicle screw fixation
- MIS-TLIF (minimally invasive transforaminal lumbar interbody fusion)
- Lateral interbody fusion (XLIF, LLIF, OLIF)
- Microdiscectomy
- Full-endoscopic discectomy (transforaminal and interlaminar)
- Unilateral biportal endoscopy (UBE)
- Laser disc repair
What these procedures share is a goal accomplish the same surgical objective through smaller corridors and with less muscle disruption than traditional open surgery. What they do not share is a complication profile, a recovery timeline, or a long-term outcome. An MIS-TLIF and a full-endoscopic discectomy are both labeled “minimally invasive,” and both are dramatically different operations with different success rates.
This is the central problem with the question “is minimally invasive spine surgery better?” The label is too broad to answer it.
What “Minimally Invasive” Originally Meant And What It Has Become
The original MISS movement, beginning in the late 1990s, was motivated by a specific clinical problem: traditional open spine surgery required wide midline incisions, extensive paraspinal muscle stripping, and prolonged retraction that produced measurable long-term muscle injury, atrophy, and chronic pain even when the spinal pathology itself was corrected. ¹⁰ The downstream cost of the exposure was, in some patients, larger than the cost of the actual disc or stenosis being treated.
MISS techniques were developed to reduce that collateral damage. The original promise was specific and modest: same operation, less soft-tissue trauma, faster recovery.
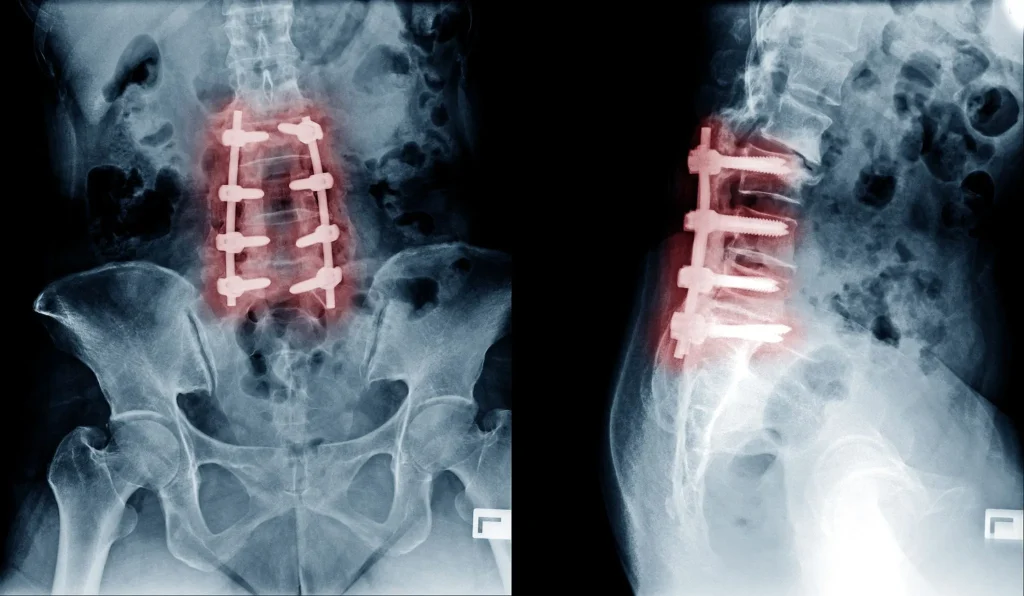
Over time, the term has expanded. “Minimally invasive” is now used to describe almost any spine procedure that uses a smaller incision than what was standard in 1995, regardless of what is actually being done under the skin. A two-level lumbar fusion with percutaneous pedicle screws is described to the patient as “minimally invasive” even though the procedure still removes the disc, places permanent hardware, and permanently eliminates motion at the operated segment. The incision is smaller. The operation, biologically, is the same.
This is where marketing and medicine diverge. A smaller incision is a real benefit, but it does not change what happens to the spine after the incision.
What the Peer-Reviewed Data Actually Shows
When you set the marketing aside and read the comparative literature, the picture is clear.
Perioperative Outcomes: MISS Wins Consistently
Across virtually every comparative study, MISS approaches outperform open surgery on the metrics measured during and immediately after the operation:
A 2024 systematic review and meta-analysis of seven studies and 909 patients undergoing surgery for thoracolumbar fractures found that MIS produced lower postoperative ODI and NRS pain scores than open surgery, with significant reductions in blood loss, operative time, infection rate, hospitalization length, and rehabilitation time. ³
A retrospective cohort study of 80 patients comparing unilateral biportal endoscopic (UBE) discectomy to microscopic discectomy reported shorter operative time, shorter hospital stay, less blood loss, and greater early improvement in VAS, ODI, and JOA scores at 3 days, 3 months, and 6 months in the endoscopic group. ¹¹
A multicenter retrospective comparison of MIS-TLIF (with bilateral decompression via unilateral approach) to open TLIF reported a complication rate of 6.2% in the MIS group versus 14.8% in the open group with equivalent clinical outcomes at 2 years. ¹²
On perioperative metrics; what happens during and in the first few weeks after surgery the data favoring MISS is consistent and reproducible.
Long-Term Outcomes: The Picture Is More Complicated
Where MISS proponents oversell, and where critics have a point, is in the long-term comparison. At 1 to 2 years out, most patient-reported outcomes converge between MISS and open approaches for the same procedure. By 5 to 7 years, the differences become subtle and indication-specific.

The 5-year prospective Quality Outcomes Database registry analysis of MI-TLIF versus open TLIF for grade I degenerative spondylolisthesis (297 patients) found no significant difference in 60-month ODI, NRS back pain, NRS leg pain, EQ-5D, or NASS satisfaction. The 60-month reoperation rate trended lower in the MIS group (5.6% vs. 11.6%). ⁵
A separate retrospective cohort with at least 5 years of follow-up reported a significantly lower reoperation rate after MIS-TLIF (2.2%) compared with open TLIF, with equivalent VAS and ODI scores between groups. ⁶
A 7-year follow-up study of 97 patients reported significantly higher rates of radiographic and symptomatic adjacent segment disease in the open TLIF group beginning at 5 years, though the operative ASD rate (i.e., ASD severe enough to require another surgery) was similar between groups. ⁷
The honest synthesis: MISS approaches produce better short-term outcomes and modestly lower long-term reoperation rates in most studies, but the size of the long-term advantage is smaller than the marketing implies and is not universal across procedures.
Where MISS Has Failed to Deliver
It is also worth being honest about where the marketing has outpaced the evidence.
A 2025 systematic review and meta-analysis of MIS tubular decompression versus open laminectomy for lumbar spinal stenosis found no functional benefit of MIS tubular decompression at 6 or 24 months in some included studies, with previous reviews noting inconsistent outcomes across comparative studies. ¹³ For straightforward decompressions, the benefit of the smaller incision is real perioperatively but does not always translate to better long-term function.
Critics of MISS including some published commentary in spine journals have noted that, particularly in the cost of laser discectomy, some studies have reported higher reoperation rates with certain laser-based discectomy techniques than with conventional microdiscectomy. ¹ This is not an indictment of laser-based approaches in general, but it is a reminder that the word “laser” on a marketing page is not the same as a peer-reviewed clinical outcome.
The lesson is consistent. The label “minimally invasive” describes the access. It does not describe what is being done, who is doing it, or how well-matched the procedure is to the underlying pathology.
The Three Things That Actually Determine Outcomes
If “minimally invasive” by itself does not guarantee a better outcome, what does? Three factors dominate the long-term success of any spine surgery, MISS or open:

1. Whether the Right Operation Was Chosen for the Right Patient
A 95% successful operation that is wrong for your anatomy has a 0% chance of helping you. The single largest determinant of spine surgery outcome is whether the procedure being performed actually treats the source of the pain.
A patient with discogenic pain from a contained herniated nucleus pulposus and an annular tear is not made better by a fusion, no matter how small the incision through which the fusion is delivered. A patient with mechanical instability from spondylolisthesis is not made better by an endoscopic discectomy, no matter how elegantly performed.
2. The Specific Procedure, Not the Marketing Category
Within the MISS umbrella, the gap between procedures is larger than the gap between MISS and open. A full-endoscopic discectomy through a 7 mm incision is a different operation from a percutaneous-screw MIS-TLIF, and both are different again from a tubular decompression. They are not interchangeable.
The relevant question is never “is MISS better than open?” It is “is this specific procedure the smallest correct intervention for my specific pathology?”
3. The Surgeon’s Volume and Experience
MISS procedures have steeper learning curves than open procedures. A surgeon who performs 5 endoscopic discectomies a year produces different outcomes than one who performs 200. The published learning-curve data for unilateral biportal endoscopy alone shows operative time tapering to a steady state only after roughly 43 cases. ¹²
This is why patient selection of a surgeon matters as much as selection of a procedure. The “minimally invasive” label on a hospital website tells you nothing about how many of the specific procedures that surgeon has actually done.
Where Deuk Laser Disc Repair® Fits On This Spectrum
The Deuk Laser Disc Repair® (DLDR) sits at the most genuinely minimally invasive end of the MISS spectrum. It is a full-endoscopic, laser-based procedure performed through a 4 to 7 mm incision about the diameter of a pencil eraser. There is no hospital admission, no general anesthesia in most cases, no fusion hardware, and no artificial implant.
DLDR® is not a fusion delivered through a smaller incision. It is not a discectomy with a marketing rebrand. It is a different operation that addresses the actual structural source of discogenic pain: the herniated nucleus material and the annular tear through which it has herniated.
The published outcomes:
- Peer-reviewed cervical DLDR® outcomes: 94.6% average symptom resolution across 66 consecutive patients, with 50% reporting complete (100%) resolution of preoperative symptoms and a 1.5% recurrent herniation rate. No major complications were reported. ⁸
- Institutional track record: 99.6% success rate across more than 2,000 procedures over 20+ years, with zero reported complications. ⁹
- Adjacent segment disease: not seen, because no segment is fused or replaced.
- Hospital stay: none. DLDR® is performed outpatient.
- Return to activity: days, not months.
The reason these numbers sit above the published rates for fusion (even “minimally invasive” fusion) and disc replacement is not because the incision is smaller. It is because the underlying operation is different. No bone is removed. No muscle is detached. No ligament is cut. No segment is fused. The cascade of complications: adjacent segment disease, hardware failure, pseudoarthrosis; that drives the long-term failure rate of fusion does not have a mechanism to occur after DLDR®.
DLDR® is what “minimally invasive” was originally supposed to mean: a smaller intervention that does less to the spine while addressing the actual source of pain.
Open vs. MISS vs. DLDR®
What These Numbers Don’t Tell You
Three caveats every patient should keep in mind when reading any MISS comparison:
1. “Minimally Invasive” Describes the Approach, Not the Operation
A minimally invasive fusion is still a fusion. A minimally invasive disc replacement is still a disc replacement. The smaller incision spares some muscle and shortens recovery, but the long-term biology of the spine. The loss of motion, the placement of permanent hardware, the biomechanical load on adjacent segments is the same as it would have been through a larger incision. If a fusion is being recommended, the long-term consequences of fusing your spine do not depend on whether the screws were placed through the skin.
2. Marketing Claims Outpace Evidence
The strongest peer-reviewed data supports MISS for what it is good at: less blood loss, shorter hospital stay, fewer perioperative complications, lower infection rates, and modestly lower reoperation rates over 5 to 10 years for some procedures. ³ ⁴ ⁵ ⁶ ⁷ The strongest claims sometimes made in marketing. That MISS is dramatically safer, dramatically more effective, or universally superior are not supported by the literature. ¹ ¹³
3. The Right Question Is Not “Is MISS Better?”
The right question is “is the procedure being recommended the smallest correct intervention for my specific anatomy?” A patient with a contained herniated disc and an annular tear is over-treated by an MIS-TLIF, no matter how small the incision. A patient with severe spondylolisthesis and mechanical instability is under-treated by an endoscopic discectomy, no matter how elegant the technique. The match between procedure and pathology matters more than the marketing label on the procedure.
The Bottom Line
Minimally invasive spine surgery is real, and the advantages: less blood loss, shorter hospital stays, fewer infections, faster early recovery, and in many studies modestly lower long-term reoperation rates. Are supported by peer-reviewed data across multiple procedure types. On the metrics where MISS was originally designed to outperform open surgery, it does. ³ ⁴ ⁵ ⁶ ⁷ ¹²
But “minimally invasive” is also one of the most marketed phrases in modern spine medicine, and the label has expanded far beyond what the original concept was designed to describe. A two-level fusion done with screws inserted through the skin is considered “minimally invasive” only because it uses a smaller skin incision. The spine itself receives the same operation it always did. The fusion is still permanent. The adjacent segments still bear the redistributed load. The long-term consequences of fusing the spine are not erased by the size of the incision used to do it.
The right way to read the MISS label is as a description of the access, not the operation. The question that matters is not whether the recommended procedure is “minimally invasive.” It is whether the procedure uses endoscopic techniques that utilize a small skin incision and cause minimal damage to the muscle, ligaments and spine. When treating the source of your pain.
For the majority of patients told they need a fusion or disc replacement for back or neck pain caused by a herniated disc. Even when that fusion is offered as “minimally invasive” there is a smaller, structure-preserving option that isn’t offered by other surgeons because no other surgeon can perform it. The Deuk Laser Disc Repair® is what “minimally invasive” was originally supposed to be: an operation that does less, preserves more, and treats the actual pain generator without removing or replacing any of your natural anatomy.
If a fusion, disc replacement, or any other spine surgery has been recommended to you. Minimally invasive or otherwise. Submit your MRI for a free virtual consultation before consenting. An independent review of your imaging, your symptoms, and your alternatives is not a delay in your care. It is your care.

Frequently Asked Questions
Is minimally invasive spine surgery actually safer than open surgery?
For most procedures, in most studies, yes but the size of the safety advantage is smaller than the marketing implies. Peer-reviewed comparisons consistently show MISS produces less blood loss, shorter hospital stays, lower perioperative infection rates, and modestly lower reoperation rates over 5 to 10 years. ³ ⁴ ⁵ ⁶ ⁷ ¹² However, MISS procedures still carry the major risks of spine surgery. Dural tears, nerve root injury, hardware complications, adjacent segment disease (in fusion cases), and reoperation and in some specific techniques the published reoperation rates have been higher than for conventional approaches. ¹ The advantage is real but not universal.
Does a smaller incision mean a better long-term outcome?
Not necessarily. The size of the incision determines short-term recovery but does not determine the long-term biology of the spine. A minimally invasive fusion is still a fusion, with the same long-term risk of adjacent segment disease (5–18% at 4–14 years) as a fusion done through a larger incision. ¹⁴ The procedure that is performed matters more than the size of the corridor used to perform it.
Is laser spine surgery the same as minimally invasive spine surgery?
No. “Laser spine surgery” describes a tool. A laser used at some point during the procedure. “Minimally invasive spine surgery” describes a category of approaches. Some MISS procedures use lasers; many do not. The term “laser spine surgery” has been used aggressively in marketing by some practices, and patients should ask specifically what procedure is being performed, what the laser is being used for, and what the peer-reviewed outcomes for that specific procedure are. The Deuk Laser Disc Repair® uses a precision laser as part of a full-endoscopic disc repair procedure with published peer-reviewed outcomes not all “laser spine surgery” is the same. ⁸
What is the difference between MIS-TLIF and open TLIF?
Both procedures remove the disc, place an interbody cage, and use pedicle screws and rods to permanently fuse the segment. The difference is the corridor: open TLIF uses a midline incision with extensive muscle stripping; MIS-TLIF uses tubular or percutaneous access with less muscle disruption. Peer-reviewed comparisons show MIS-TLIF produces less blood loss, shorter hospital stays, lower complication rates, and lower long-term reoperation rates (2.2% vs. 8.8% at 5 years in one cohort), with equivalent ODI and VAS outcomes at 2 to 5 years. ⁶ The long-term biology of the fusion itself including adjacent segment disease risk is the same.
Is endoscopic discectomy better than microdiscectomy?
In most comparative studies, endoscopic discectomy (transforaminal, interlaminar, or biportal) produces similar long-term pain and disability outcomes to microdiscectomy, with shorter operative time, less blood loss, shorter hospitalization, and in some studies lower recurrence and revision rates. ¹⁵ ¹⁶ The trade-off is a steeper learning curve for the surgeon; outcomes in endoscopic discectomy are more surgeon-volume-dependent than outcomes in microdiscectomy.
Can I avoid fusion by choosing a minimally invasive approach?
Sometimes — but the answer depends on the source of your pain, not the marketing of the procedure. If your pain is coming from a herniated disc or annular tear, structure-preserving options like Deuk Laser Disc Repair® can treat the source directly without any fusion. If your pain is coming from true mechanical instability (e.g., spondylolisthesis with motion), some form of stabilization may be genuinely necessary. The only way to know which category you fall into is a careful review of your MRI by a surgeon experienced in all of these approaches, not just the one they personally perform.
How do I tell if “minimally invasive” is being used as marketing in my case?
Ask three questions. First: what specific procedure is being recommended by its actual name, not its marketing description? Second: what is being done to the spine itself is a disc being removed, is hardware being placed, is a segment being fused? Third: what are the published outcomes for that specific procedure, performed by that specific surgeon, at 5 and 10 years? If the answers are vague, the “minimally invasive” label is doing more marketing work than clinical work. A free MRI review is the most reliable way to get an independent answer.
Sources
- Minimally Invasive Spine Surgery Is a Smart Marketing Concept. But Does It Result in Quicker Recovery? The Back Letter. 2009;24(9):97,104,107.
- Kim JS, Härtl R, Mayer HM. Minimally Invasive Spinal Surgery. BioMed Research International. 2016.
- Esposito F, Bove I, Vitulli F, et al. Outcome Measures of Open versus Minimally Invasive Surgery for Thoracolumbar Spinal Traumatic Fractures: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024;13:5558.
- Yang W, Pan X, Xiao X. Meta-Analysis of the Clinical Effect of MIS-TLF Surgery in the Treatment of Minimally Invasive Surgery of the Orthopaedic Spine. 2022.
- Minimally invasive versus open transforaminal lumbar interbody fusion for grade I lumbar spondylolisthesis: 5-year follow-up from the prospective multicenter Quality Outcomes Database registry. Neurosurgical Focus. 2023;54(1):E2.
- Long-term clinical outcomes of minimally invasive transforaminal lumbar interbody fusion (Mis-TLIF) compared with open TLIF (O-TLIF): A retrospective cohort study for at least 5 years. European Spine Journal. 2026.
- Comparison of minimally invasive and open TLIF outcomes with more than seven years of follow-up. North American Spine Society Journal. 2022.
- Deukmedjian AJ, Cutright J, Cianciabella A, Deukmedjian A. Deuk Laser Disc Repair® is a safe and effective treatment for symptomatic cervical disc disease. Surgical Neurology International. 2013;4:68.
- Deuk Spine Institute. Deuk Laser Disc Repair® clinical outcomes data.
- Advances and Challenges in Minimally Invasive Spine Surgery. PMC. 2023.
- He Y, Cao PF, Zhang Y, et al. Clinical outcomes of unilateral biportal endoscopic discectomy vs. microdiscectomy in lumbar disc herniation. Frontiers in Medicine. 2026.
- Comparison of minimally invasive transforaminal lumbar interbody fusion (Mis-TLIF) with bilateral decompression via unilateral approach and open-TLIF with bilateral decompression for degenerative lumbar diseases: a retrospective cohort study. 2024.
- Minimally invasive tubular decompression versus traditional open surgery for lumbar spinal stenosis: a systematic review and meta-analysis. Scientific Reports. 2025.
- Hashimoto K, Aizawa T, Kanno H, et al. Adjacent segment degeneration after fusion spinal surgery: a systematic review. International Orthopaedics. 2019.
- A Systematic Review and Meta-Analysis of Preoperative Characteristics and Postoperative Outcomes in Patients Undergoing Endoscopic Spine Surgery: Part I Endoscopic Microdiscectomy. PMC. 2025.
- Endoscope-Assisted Spine Surgery: A Comprehensive Review of Clinical Applications. PMC. 2025.


