

By Dr. Ara Deukmedjian
Board Certified Neurosurgeon
Medically reviewed on Jul 14, 2026
Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
Key Points
✓ A C5-C6 bulging disc is a protrusion of the disc between the C5 and C6 vertebrae with the outer wall still intact. ¹
✓ C5-C6 is the most common level for cervical disc problems. ²
✓ It typically pinches the C6 nerve, causing pain from the neck into the shoulder, thumb, and index finger. ³
✓ Age-related degeneration not injury. Is the leading cause in adults over 40. ⁴
✓ MRI confirms the diagnosis, but 87% of pain-free adults also show disc bulges on MRI. ⁵
✓ 75–90% of patients improve within 6–12 weeks without surgery. ⁶ ⁷
✓ ACDF (fusion) permanently removes motion and raises the risk of adjacent-segment disease. ⁸
✓ Full-endoscopic decompression removes the bulge through a 7 mm incision: no fusion, no hardware. ⁹ ¹⁰
✓ Deuk Laser Disc Repair®: 99.6% success, 0.01% complication rate, 2,700+ procedures.
The Quick Answer
In case your MRI results show you have C5-C6 disc bulge and your doctor recommends anterior cervical discectomy and fusion (ACDF), reconsider the advice and get another opinion because C5-C6 disc bulge implies that only your disc is affected but not the whole segment. In the vast majority of such cases, the disc herniation or protrusion can be removed via a 7mm incision in an endoscopic manner under local anesthesia in less than one hour without making any muscle cuts or bony resections or vertebra fusion. ⁹ ¹
What Is a Bulging Disc In The Neck?
The cervical spine has seven vertebral segments labeled as C1 to C7. There is an intervertebral disc located between every two adjacent segments. Which acts as a shock absorber, where the nucleus pulposus (gelatinous center) is surrounded by annulus fibrosus (outer ring). C5-C6 disc is the main load bearer of the mid-cervical spine. Every time you look down to your mobile phone, turn your head or extend your neck. You will feel pain in the neck.
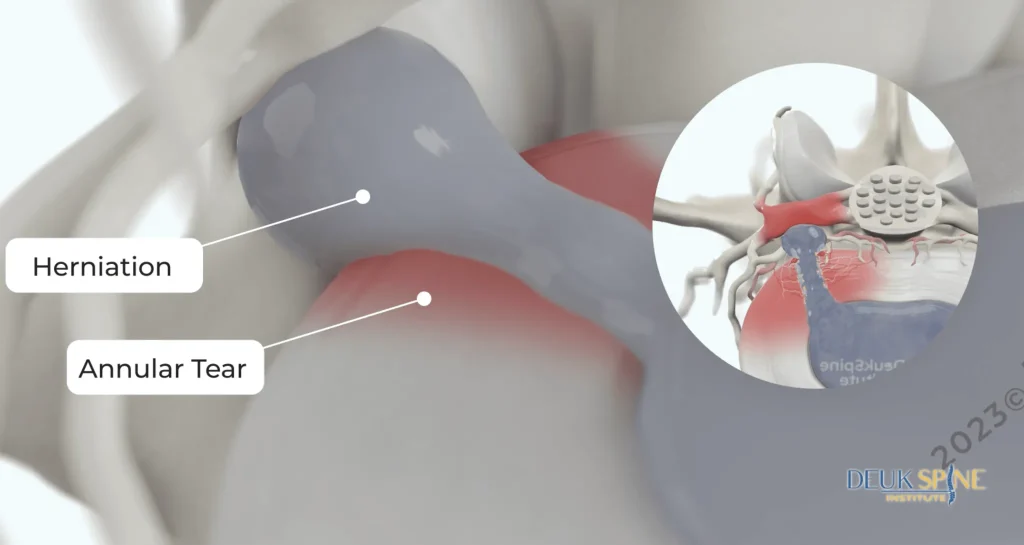
Disc bulge refers to the process whereby there is weakening of the annulus leading to disc swelling beyond the normal boundary while maintaining integrity of the external wall. In the case of herniation of the disc, there is actually tearing of the annulus resulting in protrusion of the nucleus into the spinal canal or foramen. ¹
The involved discs are C5-C6 and the involved nerve root is C6. If the disc bulge affects the neural foramen or central canal, the patient presents with symptoms of “pinched nerve in the neck.”
C5-C6, along with C6-C7, accounts for the majority of symptomatic cervical disc disease. ² The reason is mechanical: this level sits at the pivot between the highly mobile upper cervical spine and the stiffer cervicothoracic junction. And it accumulates the most wear over a lifetime.
Symptoms of a Bulging Disc in C5-C6
Symptoms fall into three categories depending on what the disc is pressing on. The disc itself (discogenic pain), the C6 nerve root (radiculopathy), or the spinal cord (myelopathy).
1. Axial neck pain (discogenic pain)
A deep, aching pain confined to the neck. Sometimes spreading into the shoulder blades is the earliest and most common symptom. It reflects irritation of nerve endings within the outer disc wall itself, not compression of a spinal nerve. ¹ Discogenic pain typically worsens with sustained flexion (looking down at a screen) and improves with lying flat.
2. C6 radiculopathy (arm symptoms)
When the bulge compresses the C6 nerve root. Symptoms follow the C6 nerves and are typically one-sided: ³
- Pain: travels from the neck into the shoulder. Down the outer arm and forearm, into the thumb and index finger
- Sensory changes: numbness or tingling in the thumb and radial forearm
- Motor weakness: weak biceps and wrist extensors (difficulty lifting a coffee cup or bringing the wrist backward against resistance)
- Reflex changes: diminished brachioradialis reflex
Symptoms characteristically worsen with neck extension and rotation toward the painful side and improve when the arm is placed overhead. The “shoulder abduction relief sign,” which is highly specific for cervical radiculopathy. ³
3. Stiffness and reduced range of motion
Muscle spasms caused by reflex guarding of the injured area create stiffness which is severe especially early in the morning or after periods of immobility. There may be difficulties with seeing out of the corners of the eyes when driving.
4. Cervical myelopathy
If a large central bulge compresses the spinal cord itself, the presentation changes and becomes urgent. Myelopathy is a surgical red flag and requires immediate evaluation: ¹¹
- Loss of fine motor control in the hands
- Being unbalanced when walking
- Hand clumsiness or dropping objects
- Hyperreflexia, positive Hoffman’s sign, or a positive Babinski
- Bowel or bladder changes
Any of these findings warrant urgent imaging and specialist referral.
Bulging vs. Herniated Disc at C5–C6
The two terms are often used interchangeably, but they describe different structural failures. Here is what actually distinguishes them on imaging and in symptoms.
Both conditions respond to the same non-operative care. And both are candidates for endoscopic decompression when surgery is needed.
What Causes a C5-C6 Disc to Bulge?
The dominant cause in adults over 40 is age-related degeneration, not injury. ⁴ Over years, the disc loses water content, the annulus develops microscopic fissures. And the disc’s height and shape change. Contributing factors include:
- Cumulative mechanical load — forward-head posture, prolonged desk work, and “text neck” concentrate stress at C5-C6. ²
- Genetics — twin studies show heritability accounts for 34–74% of disc degeneration. ¹²
- Smoking — nicotine reduces disc nutrition and accelerates degeneration.
- Trauma — motor vehicle accidents, sports impacts, and whiplash can acutely worsen or unmask an already degenerated disc, but pure traumatic bulges in a healthy disc are uncommon. ⁴
- Occupational exposure — repetitive overhead work and heavy load-bearing on the shoulders.
Diagnosing A C5-C6 Bulging Disc
1. History and physical exam
A spine specialist will map the exact source of your pain. Through testing the C5-through-T1 strength and reflexes, and performing provocative maneuvers. The Spurling test (extension, rotation, and axial compression toward the symptomatic side) and the shoulder abduction relief sign. A textbook exam can often predict the affected level before any imaging is reviewed. ³
2. MRI
MRI is the imaging test of choice. It shows the disc, nerve roots, spinal cord, and ligaments in soft-tissue detail and is the only study that reliably distinguishes a bulge from a herniation and identifies cord compression. ⁵
3. CT and CT myelogram
CT scanning is more useful in terms of bone pathology including osteophytes, facet arthrosis, and the foramina. A CT myelogram is used in cases where MRI cannot be performed or when MRI is equivocal.
4. EMG / nerve conduction studies
If the level of the disease is not known, or if the radiographic findings do not correlate with the patient’s symptoms, then the electrophysiological examination will be able to pinpoint which nerve root is inflamed and also exclude peripheral entrapment syndromes (carpal and cubital tunnels).
The MRI only tell us so much
This is absolutely key in terms of taking care of the cervical spine. Population-based research has found that 87% of asymptomatic adults have a disc bulge on their cervical MRIs, which increases with age. ⁵ Having an MRI abnormality is not a diagnosis by itself. Symptomatology, physical examination, and imaging need to be consistent and confirm the same level and the same nerve root in order for any treatment plan, particularly surgical intervention, to be considered. Surgical procedures based only on MRI is a warning sign.
Non-Surgical Treatment of a C5-C6 Bulging Disc
For most patients, a symptomatic disc bulge between C5-C6 can be managed conservatively. Non-operative management of radiculopathy without any red flags according to North American Spine Society is recommended for 6 to 12 weeks based on prospective outcomes literature. ⁶ ⁷
Activity modification and posture correction
Relative rest, adjustment of the monitor height, and avoidance of prolonged forward head postures can minimize the load on the C5-C6 disc during acute periods of inflammation.
Physical therapy

Cervical disc disease treatment with physical therapy is focused on deep neck flexors strength training, shoulder blade stability training, and traction. Extensive exercise programs based on spinal extension are usually counterproductive and should be avoided.
Medication
NSAIDs are first-line. A short course of oral steroids (a Medrol dose pack, for example) is appropriate for acute severe radiculopathy. Opioids are not appropriate long-term treatment and do not address the underlying compression.
Cervical epidural steroid injection
In patients who still experience unresolved symptoms despite weeks of conservative management. Image guided cervical epidural or transforaminal steroid injection can provide relief by delivering an anti-inflammatory agent straight into the inflamed nerve root. It can provide meaningful relief. And importantly, helps confirm the pain generator before any surgery is considered. ⁷
When conservative care is not enough
Non-operative care fails when:
- Symptoms persist beyond 6–12 weeks of appropriate treatment
- Arm weakness is present or progressing
- Pain is severe enough to disable normal function
- Any myelopathy red flags emerge
At that point, decompression should be discussed. But the type of decompression matters.
Surgical Treatment: The Case Against Defaulting to Fusion
The conventional treatment for C5-C6 disc herniation with radiculopathy is an anterior cervical discectomy and fusion procedure (ACDF). In an ACDF operation the whole disc is surgically removed and the adjacent vertebrae are permanently fused by using a cage, plate, and screws. ACDF has been the gold standard cervical surgery procedure for many years because of its effectiveness. But it treats a focal disc problem with a whole-segment solution, and it has three durable costs:

- Permanent loss of motion at the treated level.
- Adjacent-segment disease. A landmark study by Hilibrand et al. found symptomatic adjacent-segment degeneration at a rate of approximately 2.9% per year after ACDF, with 25.6% of patients affected within 10 years. ⁸ The mechanical load a fused level cannot absorb is transferred to C4-C5 above and C6-C7 below.
- Recovery. ACDF requires an inpatient stay, weeks of restricted activity, and a several-month bone-healing timeline.
However, CDR is motion-preserving with better adjacent-segment results compared to ACDF, although it requires complete removal of the intervertebral disc, use of metallic implants, and a lifetime commitment to a prosthesis. Not every disc herniation at the C5-C6 level needs such aggressive surgery.
Posterior cervical foraminotomy/discectomy avoids fusion but disrupts the paraspinal muscles and lamina, with a longer recovery and higher rate of persistent axial neck pain.
The critical question is whether your specific C5-C6 disc bulge actually requires any of these trades. In the absence of documented instability, cord compression with myelopathy, or multi-level severe pathology, the answer for most patients is no.
The Endoscopic Alternative: Full-Endoscopic Cervical Decompression

Full-endoscopic cervical decompression is the modern, ultra-minimally-invasive treatment for a C5-C6 disc bulge in appropriately selected patients. ⁹ ¹⁰
How it works
- A 7 mm skin incision is made under fluoroscopic guidance.
- A tubular dilator is passed between the paraspinal muscles. Muscles are spread, not cut.
- An HD endoscope with a working channel is inserted into the disc area using saline irrigation continuously.
- In magnified live viewing, the surgeon uses micro-instruments and a side-firing holmium laser to remove the precise problematic tissue from the disc.
- The lamina, facet joints, and spinal ligaments are preserved. No implants are used.
- The wound is closed with one suture or skin adhesive.
Because no bone is cut and no structural element is removed, the procedure is motion-preserving. There is no fusion, no hardware, and no biomechanical liability at the adjacent levels.
What the evidence shows
- Randomized and prospective studies of full-endoscopic cervical decompression report clinical success rates in the 85–95% range, with outcomes equivalent or superior to ACDF and significantly less blood loss, hospital stay, and recovery time. ⁹ ¹⁰
- Reported major complication rates are on the order of 1–3%, comparable to or lower than open cervical surgery. ¹⁰
- Most patients are discharged the same day, back to desk work within a week.
Deuk Laser Disc Repair® for C5-C6
Deuk Laser Disc Repair® is our proprietary endoscopic-laser decompression, refined by Dr. Deukmedjian over more than 15 years of dedicated endoscopic practice. For a symptomatic C5-C6 disc bulge, DLDR® uses a side-firing holmium laser through a 7 mm working channel to ablate the offending disc tissue and decompress the C6 nerve with local anesthesia, as an outpatient. Across more than 2,700 procedures the DLDR® has a 99.6% success rate. And 0.01% complication rate and the vast majority of patients return to normal activity within 72 hours.
Who Can The DLDR® Help?
Best-suited candidates:
- Symptomatic C5-C6 disc bulge with C6 radiculopathy
- Failure of 6–12 weeks of appropriate conservative care
- MRI-confirmed disc pathology matching clinical symptoms
- No radiographic instability or myelopathy
Less-appropriate candidates:
- Severe cord compression with myelopathy
- Documented cervical instability
- Multi-level severe degenerative disease
- Fracture, tumor, or infection
Patients in the second group may still require a more traditional decompression, artificial disc replacement, or fusion. An honest surgeon will tell you which category you fall into.
How to Choose the Right Surgeon for a C5-C6 Disc Bulge
Endoscopic cervical surgery is strongly surgeon-dependent, with a defined learning curve. Before consenting to any procedure, ask:
- Are you board certified and fellowship trained in neurological surgery, orthopedic spine surgery, or through the American Board of Spine Surgery?
- How many endoscopic cervical decompressions have you personally performed in the last 12 months? Recent volume matters more than lifetime totals.
- What is your published success rate and complication rate? A high-volume endoscopic surgeon can quote their own outcome data.
- Why do you recommend this procedure over the alternatives? The plan should be proportional to the pathology.
- What will you not do? A surgeon who defaults to ACDF for every disc bulge is not the right surgeon for a focal disc problem.
- Have you gotten a second opinion? If a fusion has been recommended, get one. A phone call can prevent an irreversible surgical decision.
Decompress the C6 nerve without fusing your neck.
A C5-C6 disc bulge is a focal disc problem, not a whole-segment problem. Before you consent to ACDF or an artificial disc, send your MRI for a free review by Dr. Deukmedjian and learn whether Deuk Laser Disc Repair® can decompress the C6 nerve through a 7 mm incision — under local anesthesia, in under an hour, with your disc, bone, ligaments, and natural neck motion preserved.
- 99.6%
- Average pain relief
- 0.01%
- Complication rate
- 7mm
- Incision, outpatient
FAQs
What does a C5-C6 bulging disc feel like?
Most patients describe a deep, aching neck pain that radiates into the shoulder, outer arm, and thumb, often with tingling or numbness in the thumb and index finger. Symptoms typically worsen with looking up or turning the head toward the painful side and improve when the arm is placed overhead. ³
Can a C5-C6 bulging disc heal on its own?
The disc itself does not “unbulge,” but the inflammatory process irritating the nerve usually settles. Approximately 75–90% of patients with cervical radiculopathy improve within 6–12 weeks of non-operative care. ⁶ ⁷ Asymptomatic bulges require no treatment.
Is a C5-C6 bulging disc serious?
For most patients, no. It is a treatable condition that responds to conservative care. It becomes serious when it produces progressive weakness, unrelenting pain, or signs of spinal cord compression (myelopathy), any of which warrant urgent evaluation. ¹¹
What’s the difference between a bulging disc and a herniated disc?
A bulging disc extends beyond its normal border with the outer wall intact; a herniated disc involves a tear in the outer wall that allows inner disc material to escape. ¹ Herniations are often more focal and cause more severe radiculopathy, but treatment principles are similar.
Do I need surgery for a C5-C6 bulging disc?
Most patients do not. NASS guidelines recommend an initial 6–12 week course of conservative care in the absence of red flags. ⁶ Surgery becomes appropriate when conservative care fails, weakness is progressing, pain is disabling, or myelopathy is present. Even then, surgery does not have to mean fusion.
Is fusion (ACDF) necessary for a C5-C6 bulging disc?
Almost never, unless there is documented instability, severe multi-level disease, or cord compression that cannot be addressed endoscopically. A focal disc problem calls for a focal decompression, not permanent hardware. Symptomatic adjacent-segment degeneration develops at approximately 2.9% per year after ACDF. ⁸ If fusion has been recommended for an isolated C5-C6 disc bulge, get a second opinion.
How successful is endoscopic surgery for a C5-C6 disc bulge?
Published outcomes for full-endoscopic cervical decompression report meaningful improvement in 85–95% of appropriately selected patients. Statistically equivalent to or better than ACDF, with less blood loss, shorter hospital stays, and faster return to work. ⁹ ¹⁰ Deuk Laser Disc Repair® reports a 99.6% success rate across more than 2,700 procedures.
How long is recovery after endoscopic C5-C6 decompression?
Most patients are discharged the same day, walking within hours, and back to desk work within 3–7 days. Return to full activity typically takes 4–6 weeks. ⁹
Does insurance cover endoscopic cervical decompression?
Most major U.S. insurance plans, Medicare, and workers’ compensation cover medically necessary endoscopic spine procedures, though coverage for specific advanced techniques varies by carrier. Deuk Spine Institute verifies benefits during a free MRI review.
Can I make a C5-C6 disc bulge worse?
Yes. Prolonged forward-head posture, high-impact sports during the acute phase, heavy overhead lifting, and smoking all accelerate disc degeneration or delay recovery. Posture correction and load management are essential.
References
View References
- Fardon DF, Williams AL, Dohring EJ, et al. Lumbar disc nomenclature: version 2.0. Spine J. 2014;14(11):2525–2545.
- Radhakrishnan K, Litchy WJ, O’Fallon WM, Kurland LT. Epidemiology of cervical radiculopathy: a population-based study from Rochester, Minnesota, 1976 through 1990. Brain. 1994;117(Pt 2):325–335.
- Iyer S, Kim HJ. Cervical radiculopathy. Curr Rev Musculoskelet Med. 2016;9(3):272–280.
- Wong JJ, Côté P, Quesnele JJ, Stern PJ, Mior SA. The course and prognostic factors of symptomatic cervical disc herniation with radiculopathy: a systematic review of the literature. Spine J. 2014;14(8):1781–1789.
- Nakashima H, Yukawa Y, Suda K, Yamagata M, Ueta T, Kato F. Abnormal findings on magnetic resonance images of the cervical spines in 1211 asymptomatic subjects. Spine (Phila Pa 1976). 2015;40(6):392–398.
- Bono CM, Ghiselli G, Gilbert TJ, et al. An evidence-based clinical guideline for the diagnosis and treatment of cervical radiculopathy from degenerative disorders. Spine J. 2011;11(1):64–72.
- Persson LC, Carlsson CA, Carlsson JY. Long-lasting cervical radicular pain managed with surgery, physiotherapy, or a cervical collar. A prospective, randomized study. Spine (Phila Pa 1976). 1997;22(7):751–758.
- Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH. Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am. 1999;81(4):519–528.
- Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic cervical posterior foraminotomy for the operation of lateral disc herniations using 5.9-mm endoscopes: a prospective, randomized, controlled study. Spine (Phila Pa 1976). 2008;33(9):940–948.
- Ahn Y. Endoscopic spine discectomy: indications and outcomes. Int Orthop. 2019;43(4):909–916.
- Bakhsheshian J, Mehta VA, Liu JC. Current diagnosis and management of cervical spondylotic myelopathy. Global Spine J. 2017;7(6):572–586.
- Battié MC, Videman T, Kaprio J, et al. The Twin Spine Study: contributions to a changing view of disc degeneration. Spine J. 2009;9(1):47–59.


