Dear Dr. Deukmedjian,
On behalf of the committee, I’d like to thank you for your participation in ISASS19 to be held at the Anaheim Convention Center, April 3-5. Your contributions to this event will play a significant role in continuing to provide our industry with the latest information and ideas.
Your presentation(s) is scheduled as follows:
617: Lumbar Deuk Laser Disc Repair: Long-Term Outcomes
Wednesday April 3, 2019
2:55 PM – 2:56 PM
Please note that this time might be minutes off from your original time due to changes in the program.
Please note your presentation is only one minute. We encourage you not to have more than two or three slides. There will be a timer in the room to keep all speakers on time and we appreciate your assistance in keeping to your one minute presentation time.
This year there will be a new mobile app available to attendees, which will contain the full schedule of events, abstracts, presenter information, exhibitors, interactive floor plan and more. In order to provide a robust tool for attendees, we are asking all speakers to log into the Conference Harvester to complete the tasks (listed below) at your earliest convenience. The deadline to complete is March 18.
Please note, the Speaker Ready Room at the Anaheim Convention Center North is in Room 253C which is located on the 2nd floor. The hours are as follows:
Tuesday, April 2, Noon – 5 p.m.
Wednesday, April 3, 6:30 a.m. – 5:30 p.m.
Thursday, April 4, 6:30 a.m. – 5:30 p.m.
Friday, April 5, 6:30 a.m. – 2:30 p.m.
We ask that you stop by the Speaker Ready Room at least 24 hours before your speaking time to verify they have your presentation. They are also available to help with any issues you may have with the presentation or answer questions.
Please use the link and your personalized Access Key below to log on and complete your tasks at your earliest convenience.
Objective: To evaluate the long-term efficacy and safety of Deuk Laser Disc Repair (DLDR) for the treatment of symptomatic lumbar disc disease.
Background: DLDR is an endoscopic surgical technique for the treatment of symptomatic disc disease. Safety and efficacy of DLDR has been established in prior studies; however, long term outcome data has not been previously published.
Methods: Forty-five (45) patients with a minimum follow-up of 24 months underwent lumbar DLDR between May 2008 and June 2016. Patient-reported % resolution of lower back pain, radicular symptoms and VAS score reductions were the primary outcome measures. Complications, hospital transfers and re-operation rates were evaluated.
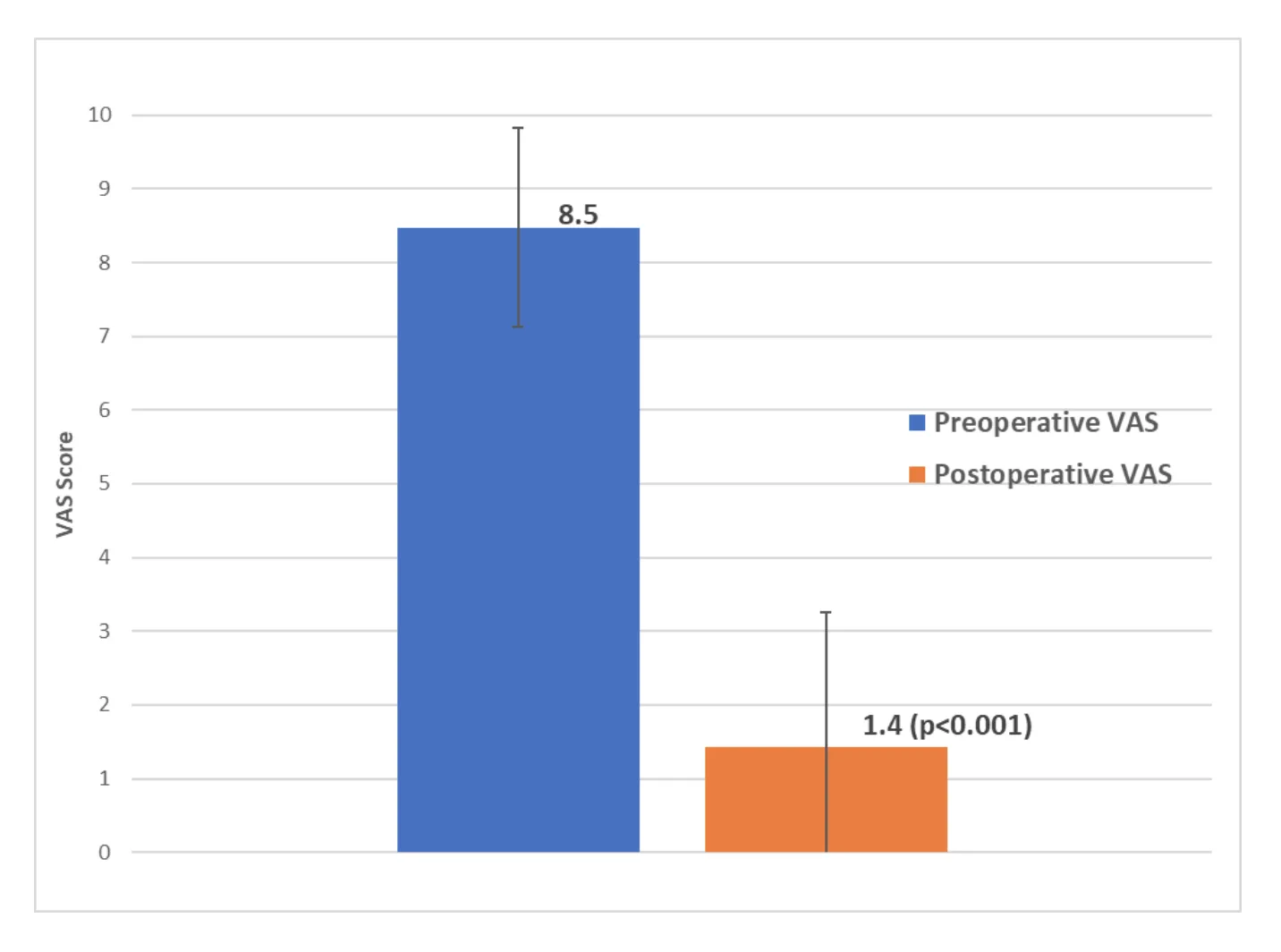
Results: Mean patient age was 55 (range, 22 – 82). Mean follow-up time was 72 months (range, 24 -120). Post-operative % resolution of lower back pain and radicular symptoms were 92 ±10% and 93 ±10% respectively. Mean preoperative VAS was 8.5 ±1.5. Mean post-operative VAS was significantly reduced to 1.4 ±1.5 (p<0.001). All procedures were performed outpatient with no complications or hospital transfers. Two (4%) patients required a revision Deuk Laser Disc Repair procedure at the index levels due to recurrent herniation at 3 months post-op. One (2%) patient developed adjacent segment disease above the index level requiring an additional Deuk Laser Disc Repair procedure at 2 months post-op.
Conclusion: Lumbar DLDR is a safe and effective treatment for lower back pain and radicular symptoms from disc disease with an average of 93% resolution. Long term follow-up demonstrates no complications from treatment and a low reoperation rate.
Lumbar endoscopic surgery is an emerging surgical technique for the treatment of chronic disc disorders and associated symptoms. Prior studies have shown promising results of endoscopic spine surgery in symptomatic relief of back pain and radicular symptoms.1-17 Reported benefits of this surgical technique include small incision sites, minimal soft tissue dissection, low intraoperative blood loss, shorter hospital stay, immediate relief of presurgical symptoms with rapid recovery to activities of daily living (ADLs), and a low complication rate.1-17 Studies have found the safety and efficacy of endoscopic spine surgery in comparison to open lumbar microdiscectomy is similar. Lumbar endoscopic surgery is superior in achieving shorter operation and rehabilitation times than traditional open lumbar microdiscectomy.1, 5, 9, 12-15, 18 Despite these positive recent findings, a lack of long-term postoperative follow up data represents a key limitation to the acceptance of lumbar endoscopic discectomy as the gold standard for treatment of symptomatic lumbar disc herniation.
Deuk Laser Disc Repair (DLDR) is a laser-assisted, endoscopic surgical treatment for symptomatic spinal disc disease.19, 20 The safety and efficacy of DLDR for symptomatic cervical disc disease has been established in prior studies.19, 20 The surgical objectives remain the same for both cervical and lumbar DLDR: 1) annular debridement, 2) discectomy and 3) foramenoplasty. Annular debridement with a Holmium-YAG laser is an essential step for eliminating axial discogenic pain and is unique to the DLDR procedure. Discectomy of both interposed and extruded nuclear fragments is performed to eliminate radicular symptoms caused by both chemical irritation (radiculitis) and compression (radiculopathy) of the associated nerve root(s). Foramenoplasty treats foraminal narrowing, further contributing to the elimination of radicular symptoms. Lumbar DLDR utilizes a transforaminal approach with a tubular retractor for treatment of symptomatic lumbar disc herniation(s) with or without spinal stenosis [Fig 1]. The endoscopic nature of the procedure provides direct visualization of the symptomatic disc herniation and nerve root allowing for maximal precision and efficacy [Fig 2].
Relatively few long term follow up studies exist for spine surgery outcomes. A PubMed database search for endoscopic lumbar spine surgery yielded 1,158 published studies. The same search with “5 year follow up” resulted in only 3 publications and there were none with over 5 year mean follow up. The purpose of this study was to report long-term (greater than 2 years) outcomes of lumbar Deuk Laser Disc Repair for treatment of symptomatic disc disease.
This study was approved by the Institutional Review Board. From May 2008 to June 2016, forty five (45) patients with symptomatic lumbar disc disease underwent Deuk Laser Disc Repair (DLDR) and met inclusion criteria for this study. Selection criteria for lumbar DLDR surgery was: 1) discogenic back pain with or without radicular symptoms for a period of at least 4 weeks, 2) failure to achieve adequate symptom relief after a minimum of 6 weeks of nonsurgical treatment including medication, therapy and interventional procedures, and 3) MRI or CT scan identifying lumbar disc herniation or spondylosis at one or more levels localized to the region of the patient’s pain. Inclusion criteria for the study included all patients that underwent lumbar DLDR and had a minimum of two (2) years of follow up data. Exclusion criteria for the study included patients with 1) history of prior lumbar spine surgery, 2) history of post-operative trauma, and 3) major deformity, fracture, tumor or infection. All surgeries were performed by a single neurosurgeon in an ambulatory surgery center. Outcome measures included VAS scores for back and leg pain and patient-reported percent relief of back pain and radicular pain/symptoms. Complications, revision rates, adjacent segment disease, and other standard perioperative variables were also recorded for all patients.
Operative technique
All patients were positioned prone on a Jackson spinal table with fluoroscopy draped in a sterile fashion into the operative field for localization and navigation. IV propofol sedation was used with MAC. Next, a 7 mm skin incision is made in the patient’s flank region on the side of their leg symptoms. Using x-ray guidance, an 18-gauge beveled spinal needle is advanced through the incision and soft tissues down to the facet joint adjacent to the symptomatic disc herniation. While advancing the needle through the soft tissues, local anesthetic is injected to minimize patient discomfort. The facet joint is then anesthetized and AP/lateral fluoroscopy is used to navigate through the foramen below the exiting nerve root to the posterior annulus at the medial pedicular line. The 18-gauge spinal needle is then advanced through the annular tear to the center of the symptomatic disc(s). The patient is advised to report the development of any new leg pain or radicular symptoms. Next, an evocative discogram is performed at the operative levels with a low pressure injection of 1-3cc of Isovue 200 with 10% indigo carmine blue dye. The patient’s response is recorded. A blunt tip guide wire is passed down the spinal needle to the center of the disc under fluoroscopic guidance. The spinal needle is removed over the guidewire and a 6mm diameter tapered tip dilator is used to enlarge the myofascial passage to the spine. A fenestrated tubular retractor is passed over the dilator and advanced into the disc at the site of annular tear and herniation. The dilator and guide wire are removed. Next, the endoscope is passed through the tubular retractor with the tip of the scope passing through the neuroforamen and into the injured disc. Continuous suction and cold bacitracin/polymyxin NaCl irrigation are used in the operative field during the procedure. The endoscope has a 3.1mm working channel through which the straight firing Holmium-YAG laser fiber and mechanical pituitary rongeurs are passed to perform the three surgical objectives of the Deuk Laser Disc Repair: discectomy, annular debridement, and foramenoplasty.
Annular debridement is unique to the DLDR and was first described by Deukmedjian et al. in the original publication in 2012.[ref] Annular debridement is the process of removing inflammatory tissue and interposed nuclear material from the gap between the torn annular edges. Annular debridement is accomplished using both laser energy to vaporize pathological inflammatory tissue and the laser’s pulse wave to mechanically dislodge fragments of abnormal tissue for removal with a pituitary rongeur. Herniated disc fragments are placed in formaldehyde and sent for independent histopathological review. Foramenoplasty for decompression of the exiting nerve root(s) is performed with removal of any foraminal disc fragments, osteophytes, and/or abnormal ligament. Adjacent exiting and traversing nerve roots are visualized endoscopically to verify decompression (if indicated) and structural preservation.
Upon completion of the annular debridement and discectomy, the endoscope is removed and 20mg of depomedrol is injected into the epidural space via the transforaminal route at each level treated to reduce postoperative nerve root inflammation/radiculitis. The skin incision is closed in multiple layers with 3.0 vicryl absorbable suture in the subcutaneous layer and steristrips on the skin. A sterile bandage is applied. Patients are discharged home the same day as their procedure.
All surgical DLDR procedures used a VersaPulse PowerSuit 80 Watt Holmium YAG laser with a 550 micrometer diameter straight firing coated fiber. Energy settings were 15 Hz with 2 Watts per burst.
Data Analysis
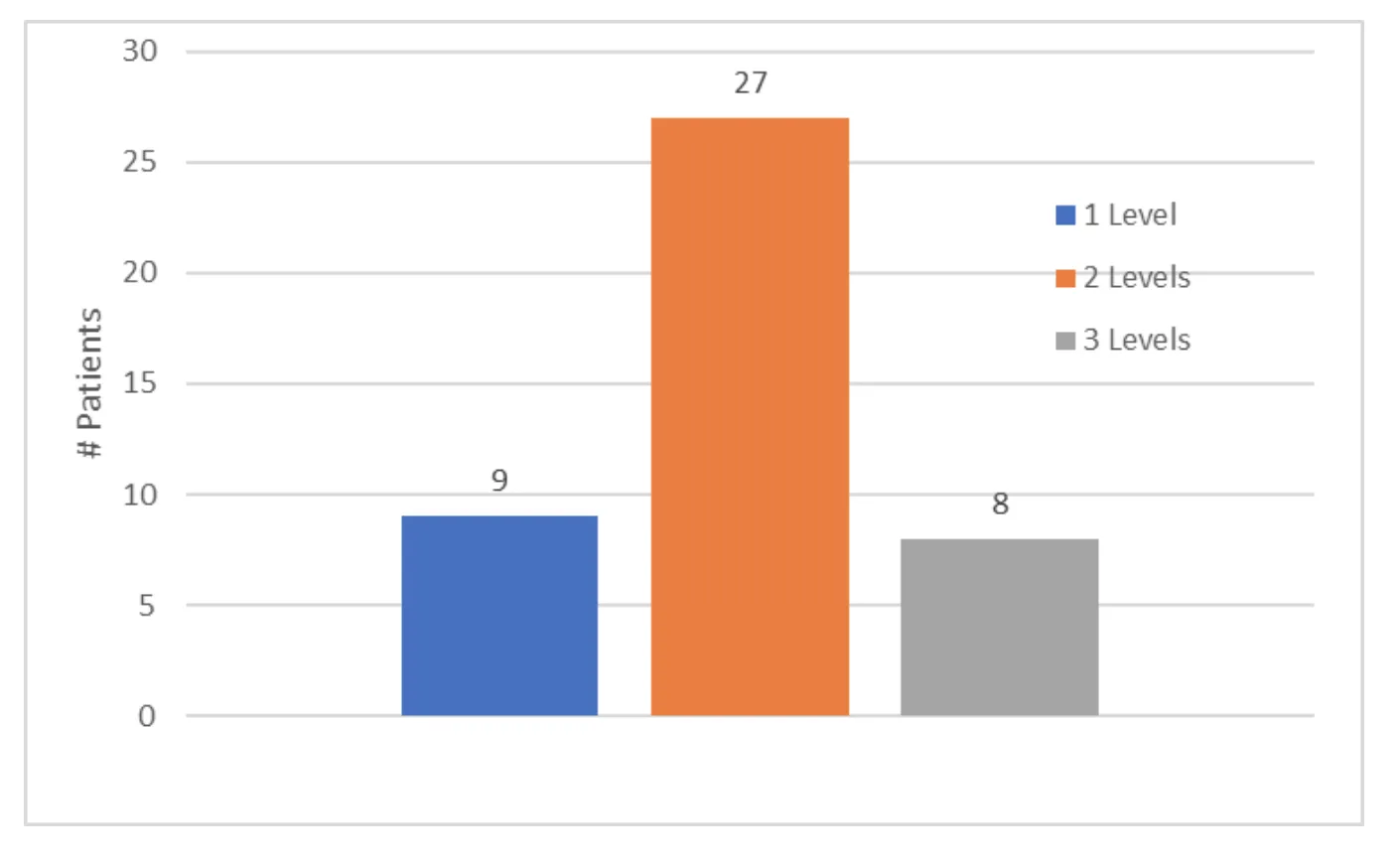
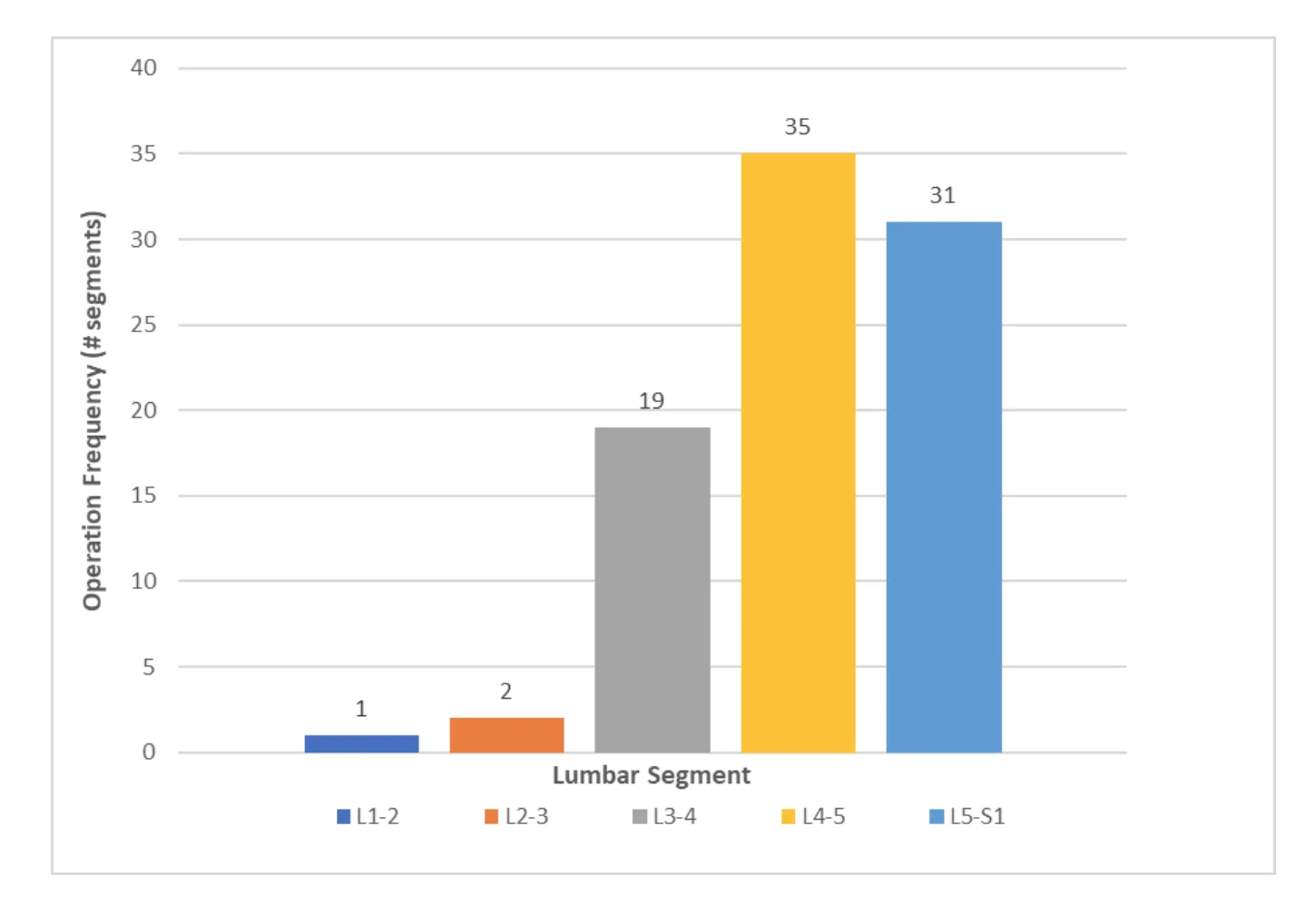
Forty-five (45) patients met inclusion criteria for the study. Mean patient age was 55 (range, 22 – 82). Male to female ratio was 2:1. Mean follow-up time was 72 months or 6 years (range, 24 -120). All DLDR procedures were performed outpatient with same-day discharge and less than 10cc of blood loss. There were no hospital transfers or complications. There were no post-operative infections. The L4-5 segment was most commonly operated on (n=35), followed by the L5-S1 segment (n=31). [Figure x] An average of 2 levels were operated on per patient.[Figure X] At last follow up, the mean patient reported post-operative % resolution of lower back pain and radicular symptoms were 92 ±10% and 93 ±10% respectively. Mean pre-operative VAS was 8.5±1.5. Mean post-operative VAS was significantly reduced to 1.4 ±1.5 (p<0.001).[Figure x] There was no significant difference in VAS score reduction among patients with 1, 2, or 3 levels operated on as determined by one-way ANOVA [F(2,41)=0.21, p=0.81]. Additionally, there was no significant difference in % relief of lower back pain and % radicular symptom relief for patients with 1, 2, and 3 levels operated on [F(2,41)=0.02, p=0.98] & [F(2,32)=0.10, p=0.9] respectively. Three (6%) patients required revision DLDR at a mean duration of 2.3 months after the initial surgery.(Table x) Of the revisions, one (2%) was performed at a segment above the index level and two (4%) revisions were performed at the index levels due to recurrent herniation. No significant differences in age, levels operated on, or number of levels operated on was found between patients that required revision DLDR vs. those that did not.
Discussion:
Lumbar endoscopic surgery for the treatment of symptomatic disc disease has been a widely practiced technique for the past decade. With an average follow up of 72 months (6 years), this study successfully describes the long-term outcomes of lumbar DLDR for the treatment of symptomatic disc disease. After treatment, patients in this study reported a mean % resolution of presurgical lower back pain and radicular symptoms of 92% and 93% respectively at their last follow up. Mean VAS scores were significantly reduced from 8.5 to 1.4, further indicating the efficacy of this procedure. Complications from lumbar endoscopic surgery have been reported elsewhere with varying frequencies and include dural tear, postoperative hematoma, nerve root injury, and infection. There were no complications with DLDR patients during the long term follow up. The safety of lumbar DLDR has further been confirmed through this study’s findings of no hospital transfers, no complications, and minimal blood loss (<10cc) in all cases. In this study, 2 (4%) patients required revision DLDR surgery for recurrent disc herniation at the previously treated level(s). This recurrent herniation rate is consistent with prior published studies.8, 11, 14-17, 21-23
One unique component of the DLDR technique that is critical in achieving high patient reported % resolution of pain is the laser-assisted annular debridement. There has been much debate in the last decade regarding the pathogenesis of discogenic back pain. Recent studies have concluded that symptomatic degenerated discs have a distinct histological characteristic within the annulus fibrosus; the formation of a zone of vascularized granulation tissue that extends from the inner nucleus pulposus to the outer edges of the annulus fibrosis within the confines of an annular fissure.24 Furthermore, studies have shown that this granulation tissue is rich with various inflammatory cytokines, nerve growth factors and nerve fiber ingrowths.24-29 Additional studies have confirmed that this zone of granulation tissue with extensive pathologic nerve ingrowth is the cause of discogenic pain, such as is seen during evocative discography.[DLDR paper, 24] In the current study, patient’s back pain was confirmed with intraoperative evocative discography to be originating from the treated disc(s). All patients having annular debridement, a procedure unique to DLDR, had near complete resolution of preoperative back pain. From these results it is clear the annular tear plays a key role in back pain genesis and surgical debridement of the inflammatory products within the annular tear will eliminate on average 92% of the patients preoperative back pain.
Ideally, future studies could include randomized controlled trials comparing DLDR to other treatments such as disc arthroplasty, fusion and microdiscectomy. Physicians treating chronic lower back pain should consider annular debridement as a viable remedy with excellent long term results.
Conclusion:
Lumbar Deuk Laser Disc Repair is a safe and effective surgical treatment for back pain and radicular symptoms including sciatica, leg pain, weakness, numbness and paresthesias from symptomatic disc disease. The excellent results have been proven to stand the test of time with durable long term outcomes evaluated on average 6 years after surgery was performed.
References:
1. Ahn S-S, Kim S-H, Kim D-W, Lee B-H. Comparison of outcomes of percutaneous endoscopic lumbar discectomy and open lumbar microdiscectomy for young adults: a retrospective matched cohort study. World neurosurgery 2016;86:250-258.
2. Ahn Y, Lee HY, Lee S-H, Lee JH. Dural tears in percutaneous endoscopic lumbar discectomy. European Spine Journal 2011;20:58-64.
3. Ahn Y, Lee S-H, Lee JH, Kim JU, Liu WC. Transforaminal percutaneous endoscopic lumbar discectomy for upper lumbar disc herniation: clinical outcome, prognostic factors, and technical consideration. Acta neurochirurgica 2009;151:199-206.
4. Ahn Y, Lee S-H, Park W-M, Lee H-Y, Shin S-W, Kang H-Y. Percutaneous endoscopic lumbar discectomy for recurrent disc herniation: surgical technique, outcome, and prognostic factors of 43 consecutive cases. Spine 2004;29:E326-E332.
5. Chen H-C, Lee C-H, Wei L, Lui T-N, Lin T-J. Comparison of percutaneous endoscopic lumbar discectomy and open lumbar surgery for adjacent segment degeneration and recurrent disc herniation. Neurology research international 2015;2015.
6. Choi K-C, Lee J-H, Kim J-S et al. Unsuccessful percutaneous endoscopic lumbar discectomy: a single-center experience of 10 228 cases. Neurosurgery 2015;76:372-381.
7. Eun SS, Lee SH, Sabal LA. Long-term follow-up results of percutaneous endoscopic lumbar discectomy. Pain physician 2016;19:E1161-E1166.
8. Jhala A, Mistry M. Endoscopic lumbar discectomy: Experience of first 100 cases. Indian journal of orthopaedics 2010;44:184.
9. Jin-Sung Kim M. Percutaneous endoscopic lumbar discectomy as an alternative to open lumbar microdiscectomy for large lumbar disc herniation. Pain physician 2016;19:E291-E300.
10. Lee DY, Ahn Y, Lee S-H. Percutaneous endoscopic lumbar discectomy for adolescent lumbar disc herniation: surgical outcomes in 46 consecutive patients. The Mount Sinai journal of medicine, New York 2006;73:864-870.
11. Lee DY, Lee S-H. Learning curve for percutaneous endoscopic lumbar discectomy. Neurologia medico-chirurgica 2008;48:383-389.
12. Lee DY, Shim CS, Ahn Y, Choi Y-G, Kim HJ, Lee S-H. Comparison of percutaneous endoscopic lumbar discectomy and open lumbar microdiscectomy for recurrent disc herniation. Journal of Korean Neurosurgical Society 2009;46:515.
13. Lee S-H, Chung S-E, Ahn Y, Kim T-H, Park J-Y, Shin S-W. Comparative radiologic evaluation of percutaneous endoscopic lumbar discectomy and open microdiscectomy: a matched cohort analysis. The Mount Sinai journal of medicine, New York 2006;73:795-801.
14. Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: a prospective, randomized, controlled study. Spine 2008;33:931-939.
15. Ryu K-S, Seocho-gu S. Percutaneous endoscopic lumbar discectomy for L5–S1 disc herniation: transforaminal versus interlaminar approach. Pain physician 2013;16:547-556.
16. Tacconi L, Baldo S, Merci G, Serra G. Transforaminal percutaneous endoscopic lumbar discectomy: outcome and complications in 270 cases. Journal of neurosurgical sciences 2018.
17. Tzaan W. Transforaminal percutaneous endoscopic lumbar discectomy. Chang Gung medical journal 2007;30:226.
18. Ruan W, Feng F, Liu Z, Xie J, Cai L, Ping A. Comparison of percutaneous endoscopic lumbar discectomy versus open lumbar microdiscectomy for lumbar disc herniation: a meta-analysis. International Journal of Surgery 2016;31:86-92.
19. Deukmedjian AJ, Cianciabella A, Cutright J, Deukmedjian A. Cervical Deuk Laser Disc Repair®: A novel, full-endoscopic surgical technique for the treatment of symptomatic cervical disc disease. Surgical neurology international 2012;3.
20. Deukmedjian AJ, Cutright SJ, Cianciabella CA, Deukmedjian A. Deuk Laser Disc Repair® is a safe and effective treatment for symptomatic cervical disc disease. Surgical neurology international 2013;4.
21. Gibson JA, Cowie JG, Iprenburg M. Transforaminal endoscopic spinal surgery: the future ‘gold standard’for discectomy?–A review. the surgeon 2012;10:290-296.
22. Nellensteijn J, Ostelo R, Bartels R, Peul W, van Royen B, van Tulder M. Transforaminal endoscopic surgery for symptomatic lumbar disc herniations: a systematic review of the literature. European Spine Journal 2010;19:181-204.
23. Yin S, Du H, Yang W, Duan C, Feng C, Tao H. Prevalence of Recurrent Herniation Following Percutaneous Endoscopic Lumbar Discectomy: A Meta-Analysis. Pain physician 2018;21:337-350.
24. Peng B, Wu W, Hou S, Li P, Zhang C, Yang Y. The pathogenesis of discogenic low back pain. The Journal of bone and joint surgery British volume 2005;87:62-67.
25. Aoki Y, Nakajima A, Ohtori S et al. Increase of nerve growth factor levels in the human herniated intervertebral disc: can annular rupture trigger discogenic back pain? Arthritis research & therapy 2014;16:R159.
26. Freemont A. The cellular pathobiology of the degenerate intervertebral disc and discogenic back pain. Rheumatology 2008;48:5-10.
27. Noorwali H, Grant MP, Epure LM et al. Link N as a therapeutic agent for discogenic pain. JOR Spine 2018;1:e1008.
28. Ohtori S, Inoue G, Miyagi M, Takahashi K. Pathomechanisms of discogenic low back pain in humans and animal models. The Spine Journal 2015;15:1347-1355.
29. Ohtori S, Miyagi M, Inoue G. Sensory nerve ingrowth, cytokines, and instability of discogenic low back pain: A review. Spine Surgery and Related Research 2018;2:11-17.
Deukmedjian Ara MD, Deukmedjian Arias, Mason Eric BS
International Society for Advancement of Spine Surgery 17 (ISASS 17)
Boca Raton, FL USA | April 12 – April 14, 2017; Session Title: Endoscopic Surgery
Session Date: 14.04.2017, Session Time Period: 1-2:00pm
Abstract(s): A-846-0000-00192
TITLE: Endoscopic Spine Surgery: Outcomes for the First 8 Years of Cervical Deuk Laser Disc
Repair® for Symptomatic Disc Herniations in 138 Patients
OBJECTIVE: To report standard perioperative measures and patient outcomes following outpatient Deuk Laser Disc Repair® (DLDR) surgeries of the cervical spine.
BACKGROUND: Symptomatic disc injuries resulting in chronic neck pain and radicular symptoms including pain, numbness, weakness and paresthesia have been traditionally treated with cervical spine decompression and fusion. However, these procedures can result in extended recovery times, hospital stays, severe decreases in mobility, extensive post-operative pain, and the requirement of prolonged time off work, physical therapy, and narcotic use, as well as potentially severe complications from the surgical exposure or hardware implanted. Deuk Laser Disc Repair® (DLDR) has been previously reported (2012) as a safe and effective outpatient surgical option for patients that suffer from discogenic neck pain and/or radicular symptoms emanating from herniated discs and/or their effects on nerve roots.
METHODS: 138 patients underwent endoscopic cervical Deuk Laser Disc Repair® from June 2008 to March 2016 by a single neurosurgeon. Estimated blood lose (EBL), disc levels operated on, duration of anesthesia, surgical times, complications, and post-operative recovery times were recorded for all patients. In addition, patient outcomes were measured with both VAS scores for neck pain and percent resolution of preoperative neck pain and radicular symptoms.
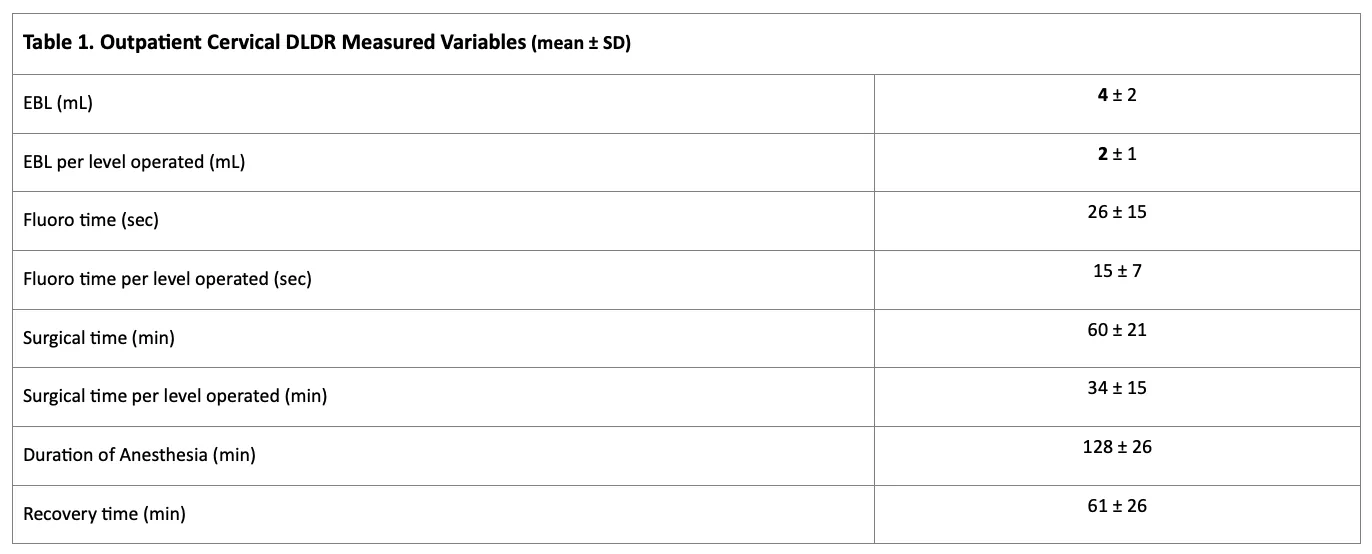
RESULTS: Mean patient age was 45 (range, 20-86) years. Male:female ratio was 3:2. EBL, fluoro times, surgical times, duration of anesthesia, and recovery times were reported for all patients (Table 1). Pre/post-operative VAS scores for neck pain were obtained (n=138) with a mean follow-up time of 13.4 weeks. VAS scores improved from a mean pre-operative score of 7.68 ± 1.86 to a mean postoperative score of 1.65 ± 2.05 (p<0.001). Confidence interval (95%) for VAS score reduction was found to be (5.61-6.47). Mean percent resolutions for preoperative axial pain and radicular symptoms were found to be 91.7% (n=135) and 93.6% (n=122) respectively. Single factor ANOVA revealed no significant difference in VAS score reduction among patients with 1, 2, 3, and 4 levels operated on p=0.56. Furthermore, there was no significant difference in percent resolutions of preoperative axial pain and preoperative radicular symptoms among patients with 1, 2, 3, and 4 levels operated on (p=0.65 & p=0.88). All patients were discharged home the same day as their operation. There were no emergency transfers and no postoperative complications or infections.
CONCLUSIONS: 138 cervical DLDR procedures were performed successfully with statistically significant reductions of 92-94% in preoperative complaints including neck pain and radicular symptoms. No significant differences were found among single and multilevel patient VAS score reduction and zero complications or infections were recorded among all patients. This study indicates that Cervical Deuk Laser Disc Repair® is indeed a safe and effective surgical option for patients that suffer from axial and radicular symptoms deriving from herniated cervical discs.

Deuk Laser Disc Repair® is a Safe, Effective, and Long-Term Solution for Disc Disease Associated Thoracic Pain.
Deukmedjian Ara MD, Deukmedjian Arias
Poster No 43, 73rd Annual South Neurosurgical Society Meeting
Marco Island Fl, February 8-11, 2023.
Dear Doctor Deukmedjian:
On behalf of the SNS Scientific Committee, I am pleased to inform you that your abstract, titled Deuk Laser Disc Repair Is A Safe, Effective, And Long-term Solution For Disc Disease Associated Thoracic Pain, has been selected for E-Poster presentation at the 73d Southern Neurosurgical Society Annual Meeting, which is to be held at the JW Marriott Marco Island Beach Resort in Florida from February 9-11, 2023. Congratulations! Please review the following information carefully.
Confirmation
To confirm your involvement, please submit your E-Poster digital file no later than January 10, 2023. You have been assigned E-Poster #43.
Online Syllabus Publication
The E-Posters will be published in the online syllabus. There is no assigned time for specific review of individual E-Posters.
Submission Process
Please create your E-Poster as follows: |
If you have any questions, please do not hesitate to contact me at [email protected], or by phone at (630) 681-1040 ext. 302. We look forward to a successful and enjoyable meeting!
Background: Thoracic disc disease is largely responsible for the major, global prevalence of Thoracic Spine Pain(TSP), both axial and radicular. Deuk Laser Disc Repair®(DLDR) is an established, peer-reviewed and published, full-endoscopic surgical procedure proven to be effective in the treatment of symptomatic cervical and lumbar disc disease. The goal of this study was to determine if posterior transforaminal DLDR could provide a safe and effective long term treatment for disc disease associated thoracic axial(dorsalgia) and radicular(intercostal) pain.
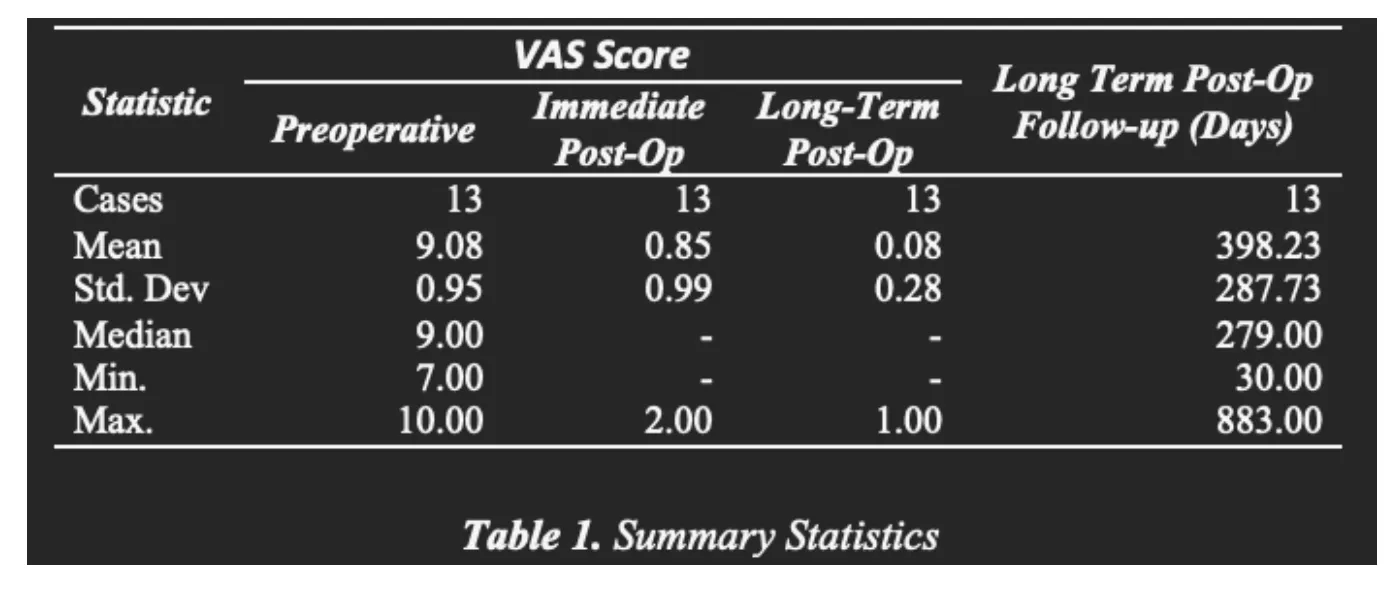
Methods: A prospective cohort of 13 consecutive patients with localized thoracic axial and radicular pain from 1-3 herniated or degenerated disc(s) underwent segmental, unilateral transforaminal endoscopic DLDR. Outcome measures included VAS, % resolution of preoperative axial and radicular pain, operative time, recovery time, EBL and perioperative complications. A paired sample t-test was carried out to test for significant differences in scores across time, but due to the small size of the study (n = 13) and due potential violations in assumptions (normality) a non-parametric alternative was determined to be most accurate. Since the samples are matched, the Wilcoxon signed-rank test was used for both comparing preoperative to immediate postoperative and the latter to the long-term follow-up VAS. Tests were carried out using R–programming and inferences are based on bootstraps (5,000 replications). The level of significance for both tests is standard at α = 0.05.
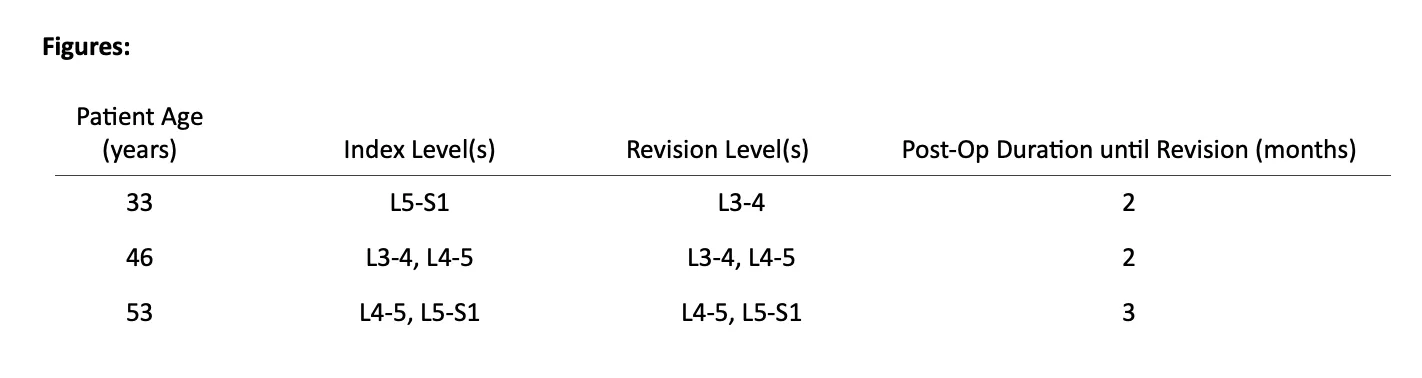
Results: All patients had significant improvement in preoperative symptoms with an average resolution of preoperative axial thoracic pain of 98.50% immediately postoperatively and 99.20% long-term postoperatively. Additionally, the average resolution of preoperative thoracic radicular symptoms for immediately postoperatively and long-term postoperatively was 96.50% and 95.90%, respectively. A Wilcoxon signed-rank test (one-tailed) showed that there is strong evidence that VAS scores for all patients (n = 13) immediately post-op are significantly lower compared to the measurements before the operation (Z = 3.22, p < 0.01). The mean VAS improved from 9.8 preoperatively to 0.85 and 0.08 immediately postoperatively and long-term postoperatively, respectively. Mean operative and recovery times were 64 minutes and 45 minutes, respectively. There were no perioperative complications. Mean, immediate postoperative follow up was 2 days. Mean, long-term follow up was 398 days. Recurrent disc herniation did not occur in any patients. A Wilcoxon signed-rank test (two-tailed) showed that there are no significant differences in VAS scores (immediately) post-op and during the follow-up measurements (Z = 1.86, p = 0.062). Both measurements have the same median score (M = 0). It should be noted that the difference is significant for α = 0.1 and more data would be required for the future.
Conclusion: Based on this preliminary study, outpatient transforaminal Deuk Laser Disc Repair® can be a safe and effective treatment for painful thoracic disc herniation with 99% and 96% long-term axial pain and radicular symptom relief respectively. There were no perioperative complications.
Background
Background Bolstering: Thoracic spine pain (TSP) is prevalent in up to as much as 10.5% of the general population making TSP a major concern for healthcare providers globally. Symptoms of thoracic disc disease include, however, are not limited to: pain that travels around the body and into one or both legs, numbness or tingling in areas of one or both legs, muscle weakness in certain muscles of one or both legs, and increased reflexes in one or both legs that can cause spasticity in the legs.
Methods
Data Results
Median score immediately post-op (M = 0) is significantly lower compared to pre-op (M = 0).
Sources:
https://www.umms.org/ummc/health-services/orthopedics/services/spine/patient-guides/herniated-thoracic-disc (Symptoms of Thoracic Pain)
https://pmc.ncbi.nlm.nih.gov/articles/PMC2720379/ (Prevalence of Thoracic Pain in the general population)
Figures:
Data Summary:
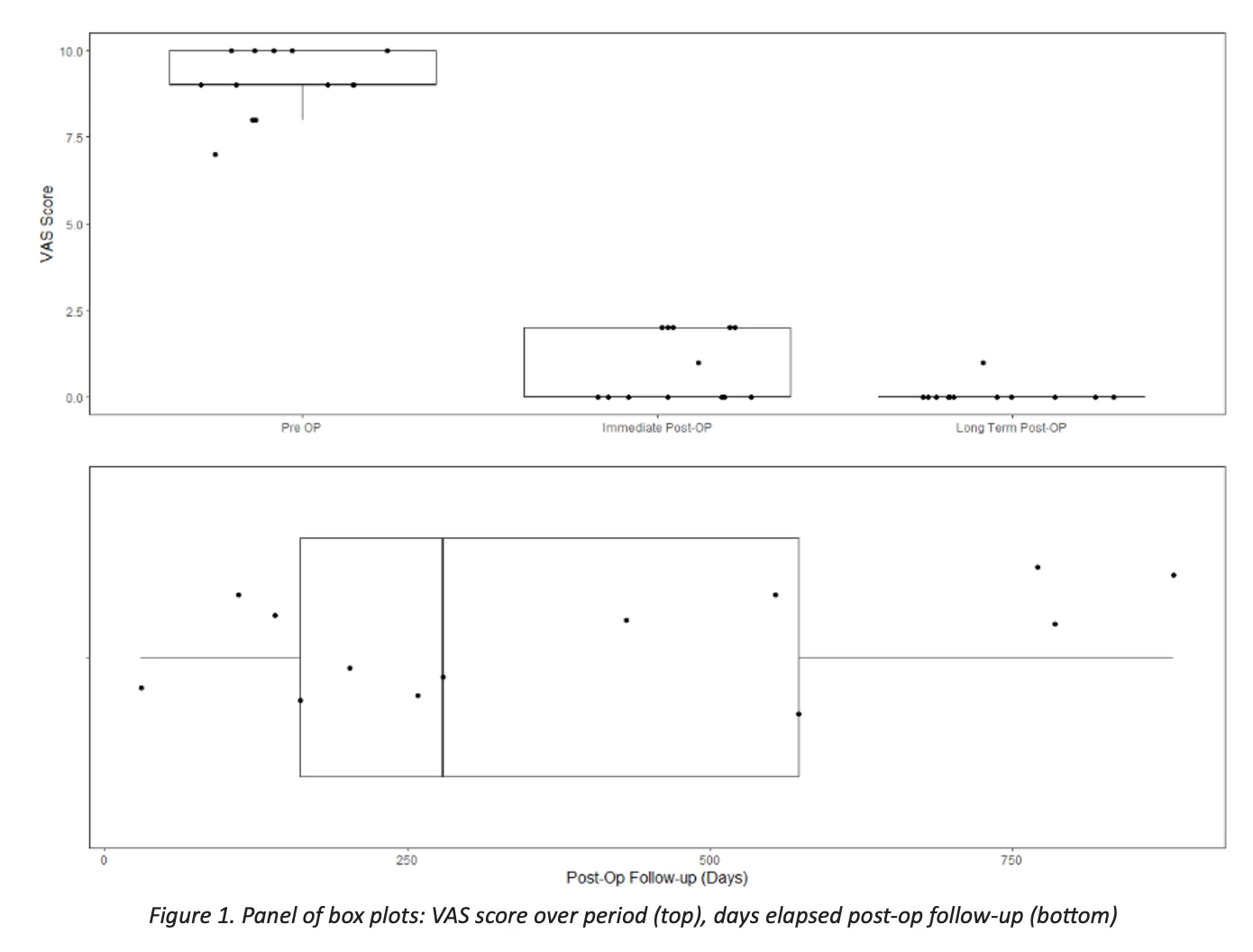
In order to address the research question VAS scores are measured in three phases for a set of patients (n = 13) who underwent Deuk Laser Disc Repair. VAS scores are measured before the operation, right after and after a certain period of time has passed.
Table 1 and Figure 1 below give a comprehensive summary of the collected data. The most noticeable change in the data is the drop in VAC scores from the pre-op to the (immediate) post-up follow – up. The difference can be inferred visually in the box plots (figure 1) as well as by the statistics in the summary table, pre-op (m = 9.08, s.d.= .95) vs. post-op (m = 9.08, s.d.= .95). No noticeable or significant differences are seen however between the immediate and long-term values of VAS. As the long-run follow-up is taken at different times after the post-op delay in days is also taken into account. On average the follow-up was done after 500 days with 75% of them under 573 days. Nonetheless as shown in figure 2 below there is no correlation between the amount of time and change in VAC scores in the follow up. One may conclude that the delay in measurement plays no role, which is an indication that the whole change in VAC happens right after the post-op phase.