


By Dr. Ara J. Deukmedjian, MD
Board Certified Neurosurgeon
Medically reviewed on June 25th 2026
Medical Disclaimer: The material contained within this article should be regarded purely for informative objectives. Consult a doctor in all cases related to the subject material within this text.
Key Points
✓ Spinal decompression surgery takes pressure off the spinal cord or nerve roots by removing whatever’s pressing on them: usually bone, ligament, or part of a disc. ¹
✓ For adults past 65, lumbar spinal stenosis is the number one reason spine surgery gets recommended. It shows up in roughly 11% of the general population, and the rate climbs from there with age. ¹ ²
✓ Open laminectomy does work for pain and disability scores improve and stay improved long-term. The catch is that about 14% of patients end up back in the OR within five years. ³
✓ Minimally invasive decompression matches open laminectomy for pain relief with shorter stays and fewer complications. ⁴
✓ Decompression does not require fusion in most cases. Fusion is for true instability, deformity, or fracture. ¹
✓ Complication rates for open and laminotomy decompression run 18–20%, with dural tears in 3.6–9% of cases. ⁵
✓ Endoscopic procedures like Deuk Laser Disc Repair® decompress the nerve without removing bone, cutting muscle, or fusing the spine.
What Is Spinal Decompression Surgery?
Spinal decompression is an overarching term for any surgery designed to take the pressure off your spinal cord or the nerves as they travel away from it. That pressure is what your surgeon calls “compression”. Compression is the reason you feel burning leg pain from sciatica, the heavy-leg drag from neurogenic claudication, the “pins-and-needles” tingling traveling down your arm from your neck discs, or the loss of strength or feeling from a compressed nerve.
The most common decompression operations are:
- Laminectomy – is when you cut out the lamina (back wall) of the vertebra, to expose the central canal space open.
- Laminotomy – this is just when you remove a small piece of the lamina to make a window in the back wall. It has a smaller window and it’s less of a big deal.
- Foraminotomy – this is when you remove part of the foramen which is where the nerve root comes out of the central canal out of the spinal column on the side.
- Discectomy / microdiscectomy – you are basically removing part of the herniated disk that is pressing down on the nerve.
- Endoscopic decompression – this is one of these above types of procedure that you do with instruments through the diameter of a pencil with a camera.
Who Needs Spinal Decompression Surgery?
Three things have to line up before decompression actually makes sense. There needs to be a structural problem on imaging. That problem has to match what the patient is feeling. And conservative care either hasn’t worked or isn’t a safe path to keep going down.
When all three boxes get checked, these are the diagnoses that most often point toward surgery:
1. Lumbar spinal stenosis (LSS)
In the low back, the spinal canal can get squeezed from several directions at the same tim. A ligamentum flavum that’s thickened over the years, facet joints worn down by arthritis, and discs that have started bulging backward into the canal. Once a patient is past 65, no other condition sends more people toward spine surgery than this one. Around 11% of the general population has it, and that number climbs hard with age. ¹ ²
What it feels like has a name: neurogenic claudication. The legs get heavy and painful when the patient stands or walks for any stretch of time, and the relief comes the second they lean forward or sit. Plenty of people stumble onto the “lean on the shopping cart at the grocery store” trick on their own, well before a doctor explains why it works.
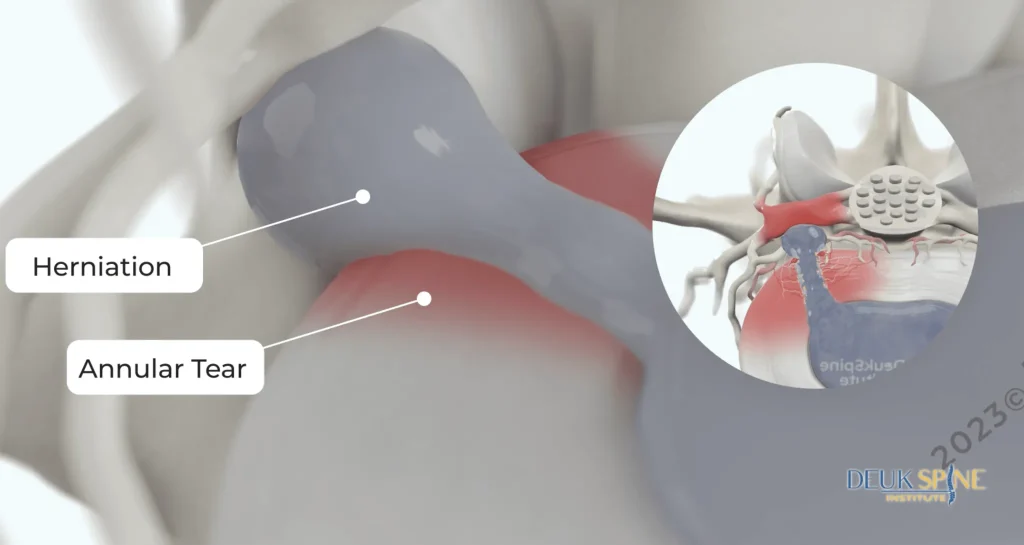
2. Herniated disc
When the soft inner gel of a disc tears through the outer wall, it can press straight onto a nerve root. The fix here is usually narrower than people expect: take out the piece of disc that’s actually causing trouble. You don’t have to remove the entire disc, and you don’t have to take off the back of the vertebra to get to it.
3. Foraminal stenosis
Bone spurs and disc material narrow the side tunnel where a single nerve exits. Patients experience sharp, electric pain following the exact path of that nerve down the arm or leg.
4. Cervical myelopathy
Pressure on the cervical spinal cord itself and not just a nerve root. This is one of the few situations where decompression is needed relatively quickly, because a pinched spinal cord compression can produce progressive, permanent dysfunction (clumsy hands, balance problems, falls).
5. Acute cauda equina syndrome
A surgical emergency. Sudden saddle numbness, loss of bladder or bowel control, and bilateral leg weakness from massive central disc herniation. This is the one situation where decompression is performed within hours, not weeks.
What Spinal Decompression Surgery Actually Looks Like
The phrase “decompression surgery” covers a wide range of operations. Patients are often surprised by how different the actual procedures are.
Open laminectomy (traditional decompression)
A 3–6 inch incision in the midline of the back. The paraspinal muscles are stripped off the bone. The lamina, the spinous process, and parts of the facet joints are removed with a high-speed drill and bone-biting instruments to expose and free the thecal sac and nerve roots. The muscles are reattached, the wound is closed in layers. Hospital stay is typically 1–4 days.
Open laminectomy works. A meta-analysis of studies with at least 5 years of follow-up found patients had significantly more satisfaction, less leg and back pain, less disability, and could walk farther without claudication compared to before surgery. The reoperation rate, however, was approximately 14%. ³
Minimally invasive surgery (MIS)
An incision smaller than an inch with tubular retractors that spread muscle rather than cutting it, and a microscope or endoscope for visualization. The same bone and ligament that need to come off still come off, but the muscles and posterior tension band are largely preserved.

A meta-analysis comparing minimally invasive decompression to open laminectomy in multilevel lumbar stenosis found MIS produced shorter hospital stays, less blood loss, and lower complication rates with comparable pain relief at one year. ⁴
Unilateral laminotomy with bilateral decompression
A muscle-sparing technique in which the surgeon approaches from one side, undercuts the spinous process, and decompresses both sides of the canal through a single small window. In a systematic review of 371 patients, VAS pain scores improved from 4.2–7.5 preoperatively to 1.4–3.0 at final follow-up, with an overall complication rate of 18–20% and a dural tear rate of 3.6–9%. ⁵
Endoscopic and laser-based decompression
The disc, the nerve, and the compression are directly viewed via small pencil port and removed. The source of pressure on the nerve is removed. No bone removal, no muscle slicing, no ligaments to sever and no implants needed. This outpatient surgery under minimal sedation allows for same-day discharge.
This is the category that includes Deuk Laser Disc Repair®.
The Risks Patients Are Rarely Told About
Spinal decompression is generally a safe operation in experienced hands, but “generally safe” is not “risk-free,” and informed consent means knowing the full list.
- Dural tear (CSF leak): The membrane around the spinal cord can tear during bone removal. Reported in 3.6–9% of unilateral laminotomy cases and higher in revision surgery. ⁵
- Reoperation: Roughly 14% of patients undergoing laminectomy for LSS return to the operating room within five years for recurrent stenosis, instability, or adjacent segment disease. ³
- Spinal instability: Take out too much bone — particularly at the facet joints — and the segment can lose its mechanical integrity. This is one of the single biggest reasons a patient who came in for a “simple decompression” walks back out being told they also need a fusion.
- Adjacent segment disease: The moment you decompress a level (and especially when you fuse one), the vertebrae directly above and below start absorbing load they were never meant to carry alone. They wear out faster. Sometimes much faster.
- Pain that doesn’t go away or comes back: Decompression fixes compression. That’s it. It doesn’t repair the torn disc, it doesn’t quiet down an arthritic facet joint, and it doesn’t undo years of muscular guarding and dysfunction. If any of those were driving the pain in the first place, they’ll still be there after surgery.
- Infection, bleeding, blood clots, anesthesia reactions: Standard risks for any inpatient spine procedure, and worth taking seriously even when they’re statistically uncommon.
Put the techniques head to head, and the pattern is consistent: minimally invasive approaches show lower complication rates than open laminectomy, with one-year pain relief that holds up about the same. ⁴
Conservative Care: What Should Happen First
Outside of true emergencies: cauda equina, progressive myelopathy, severe or worsening motor weakness. Every major guideline says the same thing: start with non-surgical care. ¹
- Activity modification: Back off the positions that load a stenotic segment. Long periods of standing and any sustained extension are usually the worst offenders.
- Physical therapy: A flexion-biased program, with real attention paid to core strength and hip mobility, tends to move the needle most.
- Oral medications: NSAIDs handle the inflammatory piece. When nerve pain is the dominant symptom, neuropathic agents like gabapentin or duloxetine often work better than standard analgesics.
- Epidural steroid injections: Genuinely useful — for narrowing down the diagnosis and for short-term relief. Just don’t mistake them for a long-term answer, because they aren’t one.
Once 6 to 12 weeks of real conservative care have come and gone with no meaningful improvement, and the MRI lines up with what the patient is actually feeling, then surgical decompression earns its place in the conversation. Not before.
Decompression vs. Decompression-Plus-Fusion: The Key Question
This is the single most important distinction in the entire conversation, and it’s where many patients are over-treated.
Decompression alone removes the pinching on the nerve and leaves the joint moving.
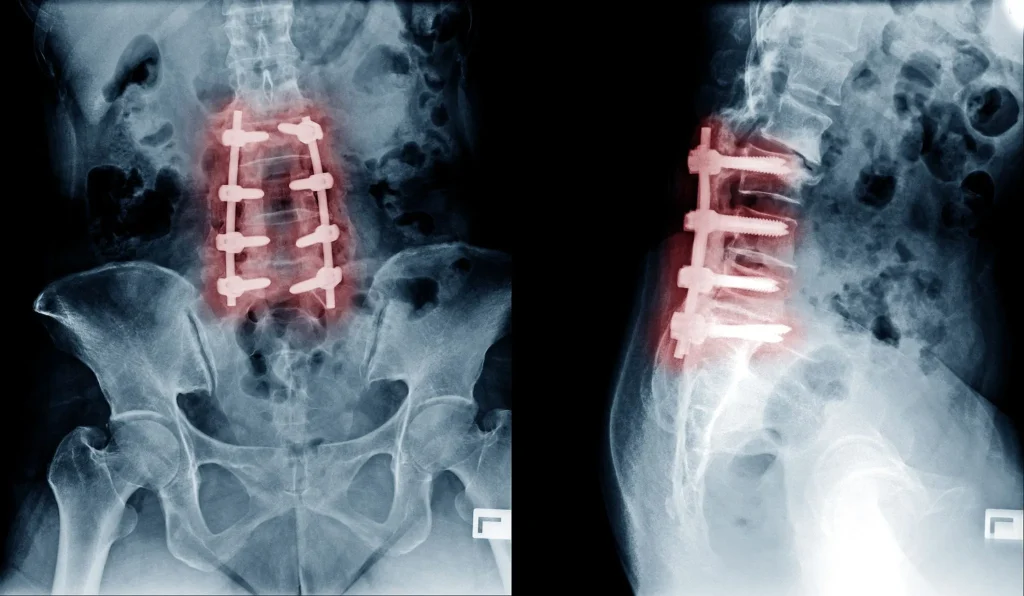
Decompression with fusion does the above and then permanently locks two or more vertebrae together using screws, rods, and bone graft.
Fusion is appropriate when the spine is unstable. Like true spondylolisthesis with progression, scoliosis, fracture, tumor, or significant deformity. Fusion is not appropriate as a default add-on to decompression for pain alone, and yet it is frequently recommended that way. A second opinion is always warranted when fusion is proposed in the absence of documented instability.
How Deuk Laser Disc Repair® Decompresses the Nerve Without a Laminectomy
When the nerve compression is coming from a herniated, bulging, or torn disc. The most common pain generator in working-age adults is a herniated disc. Removing bone from the back of the spine to indirectly “make more room” treats the symptom, not the cause.
The Deuk Laser Disc Repair® (DLDR) procedure is an outpatient endoscopic procedure using light sedation. Dr. Deuk uses direct endoscopic visualization through a 4 -7mm incision to reach the damaged area of your disc through natural anatomic pathways. Then locates the precise location of your annular defect or herniation; delivers targeted laser energy that removes the responsible tissue and seals the tear in the annular wall.
What DLDR does not do is just as important:
- It does not remove the lamina.
- It does not cut or strip paraspinal muscles.
- It does not fuse any segment.
- It does not implant screws, rods, plates, or cages.
- It does not destabilize the spine.
- It does not restrict normal motion.
DLDR is available for the lumbar, cervical, and thoracic spine. Patients walk out the same day and return to normal activity within 72 hours with light restrictions. For facet pain and SI joint pain; common companions to disc disease. Deuk Plasma Rhizotomy® deactivates the pain-carrying nerve without burning, hardware, or fusion.
Decompress the nerve without removing bone or fusing your spine.
Months of back pain and now they want to operate? Before you agree to a laminectomy or fusion, send your MRI for a free review by Dr. Deukmedjian and learn whether an endoscopic, motion-preserving option like Deuk Laser Disc Repair® can take the pressure off your nerve — no bone removal, no muscle cutting, no hardware.
- 99.6%
- Average pain relief
- 0.01%
- Complication rate
- 72hrs
- Back to normal activity
FAQs
What is spinal decompression surgery in simple terms?
What is spinal decompression surgery, in really simple terms? “I would say it’s basically any type of surgery designed to remove the pressure on the spinal cord or the nerve roots,” explains Dr. Chen, referring to operations where the surgeon is cutting away pieces of bone (laminectomy), ligaments, or disc material to relieve pinching on a nerve. The outcome is an opening where the nerves can no longer be pinched, the inflammation subsides, and the resulting sciatica or heavy feeling and lack of sensation in the leg improves.
Is spinal decompression surgery major surgery?
That varies with the technique. A traditional open laminectomy is a big inpatient surgery with a multi-day hospitalization, a considerable amount of blood lost, and a meaningful recovery. An outpatient and lightly sedated minimally invasive or endoscopic decompression procedure will have most people home on the day of their surgery. Despite being called a “decompression” by both types of procedure the actually operative procedure is drastically different.
What is the success rate of spinal decompression surgery?
In long term (5+ yr) studies of lumbar stenosis, patients enjoy less leg and back pain and less disability than before the operation, with a nearly 14% repo rate across that interval. 3 The operation succeeds to a great extent depending on which patients are chosen, surgeon’s experience, and correlation between image finding with symptoms.
What is the difference between decompression and fusion?
Decompression removes tissue that is pinching a nerve and leaves the joint mobile. Fusion permanently locks two or more vertebrae together with hardware. Many patients are told they need both — they often only need the first. Fusion is appropriate for documented instability, deformity, or fracture, not for pain in an otherwise stable spine.
How long does it take to recover from spinal decompression surgery?
Open laminectomy: 6–12 weeks for most daily activities, 3–6 months for full recovery, sometimes longer. Minimally invasive decompression: 2–6 weeks. Endoscopic procedures such as Deuk Laser Disc Repair®: roughly 72 hours back to normal activity with light restrictions.
What are the most common complications?
Dural tears (3.6–9%), recurrent stenosis or herniation, iatrogenic instability sometimes requiring a second operation, adjacent segment disease, infection, and persistent pain. ⁵ Overall complication rates for open and unilateral-laminotomy decompression run 18–20%. ⁵ Minimally invasive techniques produce lower complication rates with comparable pain relief. ⁴
Can spinal decompression surgery be done without removing bone?
Yes — when the source of compression is a herniated disc rather than bony stenosis. Endoscopic, laser-based procedures such as Deuk Laser Disc Repair® remove only the herniated disc fragment through a tiny port without resecting lamina, facets, or ligament.
Will I need a fusion after decompression?
Not in most cases. Fusion is reserved for documented instability, deformity, or fracture. If a surgeon is recommending fusion as a default add-on to a routine decompression, a second opinion is strongly warranted.
Does insurance cover spinal decompression surgery?
Most major insurance plans, Medicare, and workers’ compensation cover medically necessary decompression procedures. Coverage for specific advanced techniques varies by carrier. Deuk Spine Institute’s team verifies benefits during a free MRI review.
Sources
- Katz JN, Zimmerman ZE, Mass H, Makhni MC. Diagnosis and Management of Lumbar Spinal Stenosis: A Review. JAMA. 2022.
- Jensen RK, Jensen TS, Koes B, Hartvigsen J. Prevalence of lumbar spinal stenosis in general and clinical populations: a systematic review and meta-analysis. European Spine Journal. 2020.
- Machado GC, Ferreira PH, Yoo RI, et al. Long-Term Outcomes of Laminectomy in Lumbar Spinal Stenosis: A Systematic Review and Meta-Analysis. Global Spine Journal. 2022.
- Minimally Invasive Decompression versus Open Laminectomy in Multilevel Lumbar Stenosis: A Systematic Review and Meta-Analysis. World Neurosurgery. 2025.
- Algarni N, Al-Amoodi M, Marwan Y, et al. Unilateral laminotomy with bilateral spinal canal decompression: systematic review of outcomes and complications. BMC Musculoskeletal Disorders. 2023.
- Munakomi S, Cruz R. Lumbar Spinal Stenosis. StatPearls. National Library of Medicine. 2024.


