


By Dr. Ara Deukmedjian, MD
Board Certified Neurosurgeon
Reviewed on July 10, 2026
Disclaimer: The information contained within this article is for educational purposes only and is not a substitute for personalized medical advice.
Key Points
✓ Adjacent Segment Disease (ASD) is accelerated degeneration of the disc, facet joints, or ligaments at the spinal level directly above or below a previous spinal fusion. ¹
✓ ASD develops because a fused segment transfers abnormal biomechanical load and motion to the neighboring vertebrae. ² ³
✓ Clinically symptomatic ASD occurs in roughly 2.9% of fused patients per year, with a cumulative 10-year incidence of approximately 25% after cervical fusion. ¹
✓ After lumbar fusion, reoperation for ASD is reported in 9–36% of patients at 5–10 year follow-up. ⁴ ⁵
✓ Risk factors include multi-level fusion, age over 60, female sex, smoking, pre-existing degeneration at the adjacent level, and sagittal imbalance. ⁶ ⁷
✓ Symptoms mirror the original problem: axial neck or back pain, radiculopathy, and, in severe cases, myelopathy. ⁸
✓ MRI is the diagnostic standard; flexion-extension x-rays are added when instability is suspected. ⁸
✓ ASD is largely preventable by choosing a motion-preserving decompression instead of fusion whenever the underlying pathology is a focal disc or nerve compression. ⁹ ¹⁰
✓ Deuk Laser Disc Repair® preserves the natural disc, does not fuse the spine, and eliminates the mechanical setup that causes ASD. 99.6% success rate. 0.01% complication rate. Across 2,700+ procedures.
The Quick Answer
If a surgeon has recommended spinal fusion for a herniated disc, stenosis, or degenerative disc disease. Stop and get a second opinion. Fusion permanently eliminates motion at the treated level, and that lost motion has to go somewhere. It transfers to the disc and facet joints immediately above and below. Over the following decade, those adjacent segments degenerate faster than they would have otherwise. Sometimes to the point of requiring another fusion. ¹ ² ⁹
This is Adjacent Segment Disease. And it is one of the most under-disclosed long-term consequences of spinal fusion.
In the majority of patients whose fusion was recommended for a herniated disc, foraminal stenosis, or discogenic pain. The underlying problem can be treated through a 7 mm endoscopic procedure. Without cutting muscle, removing the lamina, or fusing anything. ⁹ ¹⁰
What Is Adjacent Segment Disease?
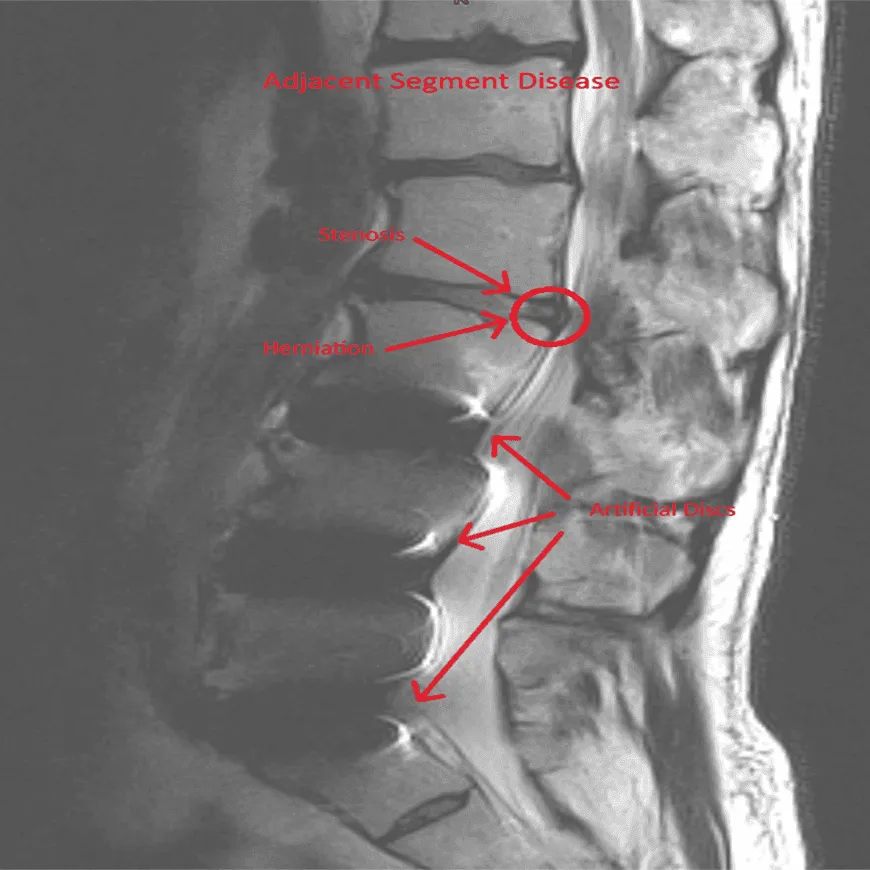
Adjacent Segment Disease, or ASD, describes accelerated degeneration and new symptomatic pathology at the mobile spinal segment directly above or below a previous fusion. ¹ The distinction matters:
- Adjacent segment degeneration is a radiographic finding on MRI or x-ray. New disc collapse, bone spurs, or facet arthritis at the level next to a fusion. It is common and often asymptomatic. ¹¹
- Adjacent segment disease is when that degeneration produces clinical symptoms. Neck or back pain, radiculopathy, or neurological compromise that require treatment. ¹
Both are direct downstream consequences of fusing a joint that was designed to move.
Why fusion causes ASD
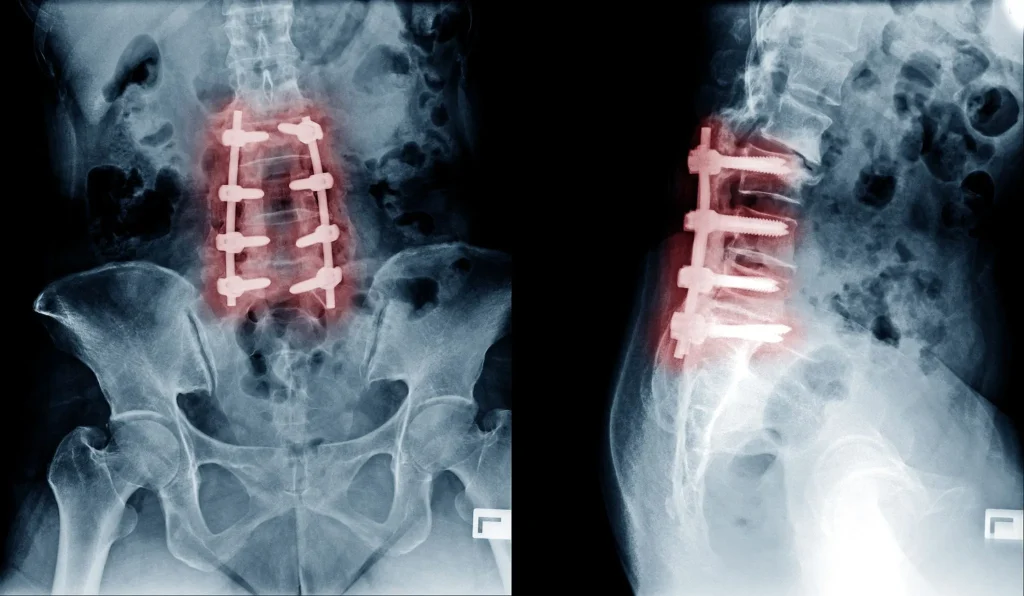
The healthy spine distributes load and motion across multiple mobile segments. When two vertebrae are locked together with plates, rods, screws, or an interbody cage, that segment can no longer contribute to bending or rotation. The mechanical work is redistributed to the levels above and below.
Biomechanical studies have shown that intradiscal pressure and range of motion at the adjacent segment increase by 30–70% after a single-level fusion, and even more after multi-level constructs. ² ³ Over years, this abnormal load accelerates disc dehydration, annular tearing, facet arthrosis, and ligamentum flavum thickening. The exact same degenerative cascade that caused the original problem. Now driven mechanically by the fusion itself.
How Common Is Adjacent Segment Disease?
The published rates depend on the region of the spine and length of follow-up.
Cervical fusion (ACDF)
Hilibrand and colleagues’ landmark long-term study of anterior cervical discectomy and fusion patients reported that symptomatic ASD developed at a rate of approximately 2.9% per year. With a cumulative incidence of 25.6% at 10 years. ¹ Approximately two-thirds of those patients ultimately required a second cervical operation.
Lumbar fusion
The reported reoperation rate for ASD after lumbar fusion ranges from 9% to 36% at 5–10 year follow-up. Depending on the number of levels fused and patient selection. ⁴ ⁵ A large meta-analysis found the pooled rate of radiographic adjacent segment degeneration after lumbar fusion was 26.6%, with symptomatic ASD in 8.5%. ⁴
Multi-level constructs
Rates rise sharply with each additional fused level. Two-level and three-level fusions carry substantially higher ASD risk than single-level procedures. Because the mechanical stress transferred to the adjacent segments compounds. ⁶ ⁷
Risk Factors for Adjacent Segment Disease
Not every fused patient develops ASD. The following factors independently increase risk: ⁶ ⁷
- Multi-level fusion (two or more levels).
- Age over 60 at the time of fusion. Older spines have less biomechanical reserve.
- Smoking. Impairs disc nutrition and accelerates degeneration.
- Pre-existing degeneration at the adjacent level on the pre-op MRI. The most important single predictor.
- Sagittal imbalance or loss of lumbar lordosis after fusion. Poor alignment forces the adjacent level to compensate.
- Facet joint violation by pedicle screws during instrumentation.
- Laminectomy above the fusion, which destabilizes the adjacent segment posteriorly.
Where Does Adjacent Segment Disease Occur?
ASD is most common at the levels with the highest baseline motion. Because they inherit the largest share of transferred mechanical load. ⁸

- Lumbar spine: L4–L5 and L5–S1 for fusions below, or the segment immediately above an L4–L5 fusion.
- Cervical spine: C5–C6 and C6–C7. The lower three subaxial levels account for the majority of symptomatic cervical ASD.
Symptoms of Adjacent Segment Disease
Symptoms depend on which structure at the adjacent segment breaks down. And which nerve it compresses. ⁸ Broadly, ASD produces one or more of the following:
Cervical ASD symptoms
- Axial neck pain, often worse with extension.
- Radiating pain into the shoulder, arm, or hand following a specific nerve root (radiculopathy).
- Tingling, numbness, or weakness in the upper extremity.
- Signs of myelopathy in severe cases: gait imbalance, hand clumsiness, hyperreflexia. This is a red flag requiring urgent evaluation.
Lumbar ASD symptoms
- Recurrent low back pain that is often described as feeling “just like before the first surgery.”
- Radiating leg pain, numbness, or weakness (sciatica).
- Neurogenic claudication. Leg pain and heaviness with walking or standing that improves with sitting or leaning forward.
- New spondylolisthesis (slippage) at the segment above the fusion.
Because these symptoms so closely mirror the original problem, many patients assume the first fusion “failed.” In reality, the fusion often did exactly what it was designed to do at the operated level. The pain is coming from the new segment that the fusion overloaded.
How Adjacent Segment Disease Is Diagnosed
1. History and physical exam
A careful history distinguishes recurrent same-level symptoms (possible pseudarthrosis or hardware failure) from new adjacent-level symptoms. The neurological exam maps the involved nerve root the same way it would for any radiculopathy.

2. MRI
MRI is the imaging test of choice. It shows disc dehydration, disc height loss, foraminal narrowing, facet arthrosis, and ligamentum flavum thickening at the adjacent segment. ⁸ Comparison with the pre-fusion MRI, when available, confirms new degeneration rather than pre-existing findings.
3. Flexion-extension x-rays
Dynamic x-rays evaluate for instability or new spondylolisthesis at the adjacent level. Instability changes the surgical decision-making significantly. ⁸
4. CT scan
CT is added when bony detail matters. To evaluate the fusion mass itself for pseudarthrosis (non-union), or to assess facet joint anatomy and pedicle screw position.
The asymptomatic ASD caveat
Population MRI studies have shown that adjacent-segment radiographic degeneration is present in a large proportion of fused patients within five years. Even without symptoms. ¹¹ The imaging finding alone does not justify another surgery. The imaging, exam, and symptoms must all point to the same segment as the pain generator.
Non-Surgical Treatment for Adjacent Segment Disease
When a patient develops symptomatic ASD, the first step is the same evidence-based conservative program used for any new radiculopathy or discogenic pain. National guidelines and the SPORT trial support an initial 6–12 week course of non-operative management in the absence of red flags. ¹²
- Physical therapy focused on core stabilization, hip mobility, and posture. Extension-based programs are usually avoided in ASD because the adjacent segment is already overloaded.
- Activity modification and ergonomic correction to reduce mechanical stress on the already compromised segment.
- NSAIDs as first-line pharmacotherapy. Short-course oral steroids in selected acute cases. Opioids are not appropriate long-term treatment.
- Image-guided transforaminal epidural steroid injection at the affected nerve root. Both therapeutic and diagnostic. It helps confirm the pain generator before any surgical decision. ¹²
When conservative care fails after 6–12 weeks. Or when there is progressive neurological deficit, disabling pain, or red flags. Decompression should be discussed. But the type of decompression matters enormously.
Surgical Treatment: The Case Against “Extending the Fusion”
The traditional surgical answer to ASD is to extend the fusion by one more level. This is exactly the approach that created the problem in the first place. And the biomechanical logic is unchanged:
- Loss of motion at yet another segment, forever.
- The next adjacent level now becomes the new highest-stress segment. Long-term studies confirm ASD rates continue to accumulate after revision fusion. ⁹
- Longer recovery, higher revision surgery complication rates, and higher rates of pseudarthrosis with each additional level. ⁷
For most patients with symptomatic ASD, whose underlying pathology at the adjacent segment is a herniated disc, foraminal stenosis, or focal nerve compression. Extending the fusion is treating the whole segment for what is a focal problem. ⁹ ¹⁰
The Motion-Preserving Alternative: Deuk Laser Disc Repair®

The best treatment for adjacent segment disease is the treatment that would have prevented it in the first place. A motion-preserving, focally targeted decompression.
Deuk Laser Disc Repair® is a full-endoscopic laser decompression developed and refined by Dr. Deukmedjian over more than 15 years of dedicated endoscopic practice.
How it works
- A 7 mm skin incision is made off the midline under fluoroscopic guidance.
- A tubular dilator is passed between paraspinal muscles. The muscles are spread, not cut.
- A high-definition endoscope with an integrated working channel is advanced directly to the pathology under continuous saline irrigation.
- Under magnified live video, a side-firing holmium laser precisely vaporizes the offending disc herniation, bone spur, or thickened ligament. The lamina, facet joint, and spinal ligaments are preserved.
- The patient’s own natural disc is left in place to continue functioning as a shock absorber and to preserve motion at the treated segment.
- The incision is closed with a single stitch or skin adhesive.
Because no bone is cut, no hardware is placed, and no segment is fused. The procedure creates no new biomechanical liability for the next adjacent level. There is no “next” ASD to worry about.
What the outcomes show
Across more than 2,700 procedures, DLDR® has a published 99.6% success rate and 0.01% complication rate. The vast majority of patients are discharged the same day, walking within hours, and back to sedentary work within 3–7 days.
For patients who already have a fusion and now have symptomatic ASD at the adjacent level. DLDR® can often decompress the new segment without extending the fusion. Provided there is no instability at that level.
Who Is a Candidate. And Who Isn’t
Endoscopic decompression is not appropriate for every ASD patient. It is best suited for patients with:
- MRI-confirmed disc herniation, foraminal stenosis, or focal compression at the adjacent level.
- Symptoms and exam findings that correlate with the imaging.
- Failure of 6–12 weeks of appropriate conservative care.
- No radiographic instability at the affected segment.
It is less appropriate for patients with:
- Documented dynamic instability or new spondylolisthesis at the adjacent level.
- Severe central canal stenosis with myelopathy.
- Fracture, tumor, or infection.
- Failed fusion (pseudarthrosis) at the original level. Which is a different problem requiring its own workup.
These situations may still require a more traditional decompression or a revision. An honest surgeon will tell you which category you are in.
How to Choose the Right Surgeon After a Fusion
Managing symptomatic ASD is technically more demanding than a first-time decompression. Because of altered anatomy, scar tissue, and the biomechanical constraints of the existing hardware. Surgeon experience matters more here, not less. ⁷
Before consenting to any procedure, ask:
- Are you board certified and fellowship trained? In neurological surgery or orthopedic spine surgery.
- How many endoscopic decompressions have you personally performed in the last 12 months? Recent volume matters. Not lifetime totals.
- How many of those were at a level adjacent to a prior fusion? ASD cases are their own subset.
- What is your published success and complication rate? A high-volume endoscopic surgeon can quote their own outcome data.
- Why do you recommend this specific procedure over the alternatives? The plan should be proportional to the pathology.
- What will you not do? A surgeon who defaults to extending the fusion for every ASD is not the right surgeon for a focal nerve-compression problem.
- Have you gotten a second opinion? If a revision fusion has been recommended, get one. It costs a phone call and can prevent an irreversible decision.
Fix the adjacent level without another fusion.
Whether you’re facing a first fusion or already have symptoms at the level above or below one, extending the fusion recreates the exact mechanical problem that caused Adjacent Segment Disease in the first place. Send your MRI for a free review by Dr. Deukmedjian and learn whether Deuk Laser Disc Repair® can decompress the affected segment through a 7 mm incision — no hardware, no bone removal, no new biomechanical liability.
- 99.6%
- Average pain relief
- 0.01%
- Complication rate
- 7mm
- Incision, outpatient
FAQs
What is the main cause of adjacent segment disease?
The primary driver is the mechanical load transferred to neighboring vertebrae after a fusion eliminates motion at the treated segment. Intradiscal pressure and range of motion at the adjacent level increase by 30–70% after single-level fusion. Accelerating disc degeneration, facet arthrosis, and ligamentum flavum thickening. ² ³ Age-related degeneration and pre-existing damage at the adjacent level compound the risk. ⁶
How soon after a fusion does adjacent segment disease develop?
Radiographic changes can appear within 1–2 years. Symptomatic ASD most commonly presents 5–10 years after fusion, at an average rate of approximately 2.9% per year for cervical fusion, with a cumulative 10-year incidence around 25%. ¹
Can adjacent segment disease be prevented?
The single most effective preventive strategy is to avoid fusion when the underlying pathology is a focal disc or nerve compression. Motion-preserving procedures such as full-endoscopic decompression and Deuk Laser Disc Repair® treat the pathology without eliminating segmental motion. Which is the biomechanical setup for ASD. ⁹ ¹⁰ Smoking cessation, weight management, and correction of sagittal alignment also reduce risk. ⁶ ⁷
Does adjacent segment disease always require surgery?
No. Symptomatic ASD is treated the same way as any new radiculopathy or discogenic pain. Guideline-based non-operative care first: physical therapy, NSAIDs, activity modification, and a transforaminal epidural steroid injection if needed. Most patients improve within 6–12 weeks. ¹² Surgery is considered when conservative care fails, when neurological deficit progresses, or when pain is severe and disabling.
Is extending the fusion the right treatment for ASD?
Almost never, unless there is documented instability at the adjacent level. Extending the fusion recreates the exact mechanical problem that caused ASD in the first place. And research shows ASD continues to accumulate at the next adjacent level after revision fusion. ⁹ A focal endoscopic decompression addresses the actual pain generator without the long-term biomechanical cost.
How successful is endoscopic decompression for adjacent segment disease?
Published outcomes for full-endoscopic decompression in appropriately selected patients report meaningful improvement in pain and function in 85–95% of cases. Statistically equivalent to or better than open microdiscectomy. With less blood loss, shorter hospital stays, and faster return to work. ⁹ ¹⁰ Deuk Laser Disc Repair® reports a 99.6% success rate across more than 2,700 procedures.
How long does recovery take after endoscopic decompression for ASD?
Most patients are discharged the same day, walking within hours, and back to desk work within 3–7 days. Return to full activity typically takes 4–6 weeks depending on the procedure and the patient.
Does insurance cover treatment for adjacent segment disease?
Most major U.S. insurance plans, Medicare, and workers’ compensation cover medically necessary decompression for symptomatic ASD, though coverage for specific advanced endoscopic techniques varies by carrier. Deuk Spine Institute verifies benefits during a free MRI review.
Is adjacent segment disease considered a disability?
Whether ASD is classified as a disability depends on the degree of functional impairment. Severe untreated ASD with progressive weakness or uncontrolled radicular pain can qualify. However, most patients respond well to targeted treatment and return to normal activity.
Sources
View Sources
- Hilibrand AS, Robbins M. Adjacent segment degeneration and adjacent segment disease: the consequences of spinal fusion? The Spine Journal. 2004;4(6 Suppl):190S-194S.
- Weinhoffer SL, Guyer RD, Herbert M, Griffith SL. Intradiscal pressure measurements above an instrumented fusion. A cadaveric study. Spine. 1995;20(5):526-531.
- Cunningham BW, Kotani Y, McNulty PS, et al. The effect of spinal destabilization and instrumentation on lumbar intradiscal pressure. Spine. 1997;22(22):2655-2663.
- Xia XP, Chen HL, Cheng HB. Prevalence of adjacent segment degeneration after spine surgery: a systematic review and meta-analysis. Spine. 2013;38(7):597-608.
- Ghiselli G, Wang JC, Bhatia NN, Hsu WK, Dawson EG. Adjacent segment degeneration in the lumbar spine. J Bone Joint Surg Am. 2004;86(7):1497-1503.
- Park P, Garton HJ, Gala VC, Hoff JT, McGillicuddy JE. Adjacent segment disease after lumbar or lumbosacral fusion: review of the literature. Spine. 2004;29(17):1938-1944.
- Radcliff KE, Kepler CK, Jakoi A, et al. Adjacent segment disease in the lumbar spine following different treatment interventions. The Spine Journal. 2013;13(10):1339-1349.
- Harrop JS, Youssef JA, Maltenfort M, et al. Lumbar adjacent segment degeneration and disease after arthrodesis and total disc arthroplasty. Spine. 2008;33(15):1701-1707.
- Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: a prospective, randomized, controlled study. Spine. 2008;33(9):931-939.
- Kim CH, Chung CK, Choi Y, et al. The long-term reoperation rate following surgery for lumbar herniated intervertebral disc disease: a nationwide sample cohort study with a 10-year follow-up. Spine. 2019;44(19):1382-1389.
- Nakashima H, Kawakami N, Tsuji T, et al. Adjacent segment disease after posterior lumbar interbody fusion: based on cases with a minimum of 10 years of follow-up. Spine. 2015;40(14):E831-E841.
- Weinstein JN, Lurie JD, Tosteson TD, et al. Surgical versus nonoperative treatment for lumbar disc herniation: four-year results for the Spine Patient Outcomes Research Trial (SPORT). Spine. 2008;33(25):2789-2800.


