

If an MRI report just told you that you have degenerative disc disease at L4-L5 or L5-S1, you probably left that appointment with more questions than answers. Does this mean your back pain will only get worse? Does it mean fusion surgery is inevitable? I’ve spent over 30 years as a board certified neurosurgeon treating patients with exactly this diagnosis, and I can tell you the honest answer up front. Degenerative disc disease treatment does not automatically mean surgery, and in many cases, the disc that shows up as “degenerated” on your scan isn’t even the source of your pain. What matters is figuring out which condition you actually have, and that takes more than a radiology report.
Diagnosis. Answers. Relief.
Submit your MRI for a free expert review by Dr. Ara Deukmedjian, M.D. —
board-certified neurosurgeon. No obligation. Real answers.
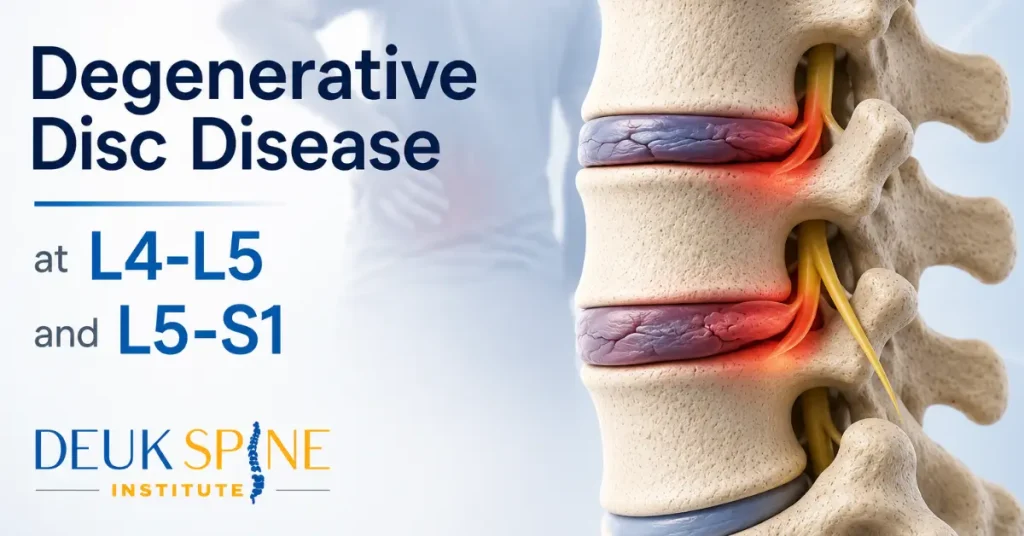
What Is Degenerative Disc Disease at L4-L5 and L5-S1?
Degenerative disc disease isn’t really a disease at all. It’s a descriptive term radiologists use for the natural wear pattern discs develop as the nucleus pulposus, the gel like center of the disc, loses hydration and height over time. The outer ring of the disc, called the annulus fibrosus, can develop small tears and lose some of its structural integrity as well. Whether that wear pattern is actually generating your pain is a separate question, one we answer with the Deuk Spine Exam®.
L4-L5 and L5-S1 are the two lowest discs in your lumbar spine, and they carry more mechanical load than any other discs in your back. That’s exactly why they show degenerative changes earlier and more often than discs higher up. If your MRI flagged degeneration at these two levels specifically, you’re looking at the most common pattern I see in my practice. If you want a deeper look at either level on its own, I’ve covered L4-L5 disc pain and L5-S1 disc pain in detail elsewhere.
Here’s what patients often misunderstand. A degenerated disc is not automatically a painful disc. Degeneration describes an appearance on imaging. Pain is a separate clinical question, and the two don’t always line up.
Common Symptoms When DDD at L4-L5 or L5-S1 Is Actually Painful
When a degenerated disc at these levels is genuinely the source of your pain, patients tend to describe a fairly consistent pattern.
- Localized low back pain that stays centered in the lower back rather than radiating clearly along a leg.
- Pain that worsens with sitting, since sitting places more load on the L4-L5 and L5-S1 discs than standing.
- Stiffness after periods of rest, particularly first thing in the morning, that loosens somewhat with movement.
- Pain that flares with bending or twisting, especially lifting motions that compress the front of the disc and open the injured posterior annulus.
- A dull, deep ache rather than the shooting, electric quality typical of nerve compression.
If your symptoms sound like this list, that’s a reasonable signal your disc could be the generator. But a signal isn’t a diagnosis, which is exactly why correlation with imaging and a physical exam matters so much.
Why Your DDD Diagnosis Doesn’t Always Mean It’s Causing Your Pain
This is one of the most important things I tell patients, and it’s backed by decades of published research. A landmark study by Jensen and colleagues in the New England Journal of Medicine examined lumbar MRI scans of 98 people who had no back pain whatsoever, and found that 64 percent of them had a disc bulge, protrusion, or extrusion at one or more levels, most commonly at L4 to L5 and L5 to S1 (Jensen et al., NEJM, 1994). In other words, the majority of people walking around with zero back pain have disc findings that look identical to what shows up on a symptomatic patient’s scan.
I bring this up because I’ve seen too many patients get steered toward major surgery based on an MRI report alone, without anyone confirming that the “degenerated” disc is the actual generator of their pain. That’s backward. The image tells you what a disc looks like. It doesn’t tell you why you hurt.
This is why I developed the Deuk Spine Exam®, which combines physical examination findings, a detailed pain history, and imaging review to identify which specific structure is generating a patient’s pain, with 99 percent diagnostic accuracy in my clinical experience. Without that correlation step, degenerative disc disease treatment decisions are little more than guesswork.
When Degenerative Disc Disease Becomes Painful, The Role of the Annular Tear and Inflammation
So if degeneration alone doesn’t explain pain, what does? In my clinical experience treating patients at the L4-L5 and L5-S1 levels, the answer almost always comes back to the same mechanism, a tear in the posterior annulus.
As a disc degenerates, small tears can form in the back portion of the annulus fibrosus. When that happens, the body responds the way it responds to any tissue injury, with inflammation. Under normal circumstances, that inflammatory response would resolve within a couple of weeks as the tissue heals. But a disc has very limited blood supply, so the tear often doesn’t heal on its own. The inflammation becomes chronic.
Over months and years, that chronic inflammation triggers a process called neoinnervation, where new pain sensing nerve fibers actually grow into the damaged, inflamed tissue of the annulus. Those nerve fibers weren’t there originally. Once they’re present, they transmit pain signals every time the disc is loaded, which for L4-L5 and L5-S1 means every time you sit, stand, bend, or lift.
Mechanical stress on the weakened annulus and pressure from any adjacent herniated nucleus pulposus material can add to this pain, but chronic inflammation within the posterior annular tear is the driver I see most consistently in patients whose disc degeneration has become symptomatic axial back pain.
One clarification I make with every patient, this is different from a pinched nerve. If a fragment of disc material compresses a nerve root, you’ll typically feel a shooting, electric quality sensation radiating down a leg along a specific path, driven largely by chemical irritation of the nerve rather than compression alone. That’s radicular pain, and it’s a different clinical problem from the localized axial back pain that comes from the disc itself. Some patients have one. Some have both. Sorting out which is present is part of an accurate diagnosis.
Is Surgery Necessary for Degenerative Disc Disease? The Treatment Ladder
Not every patient with painful DDD at L4-L5 or L5-S1 needs surgery, and I tell patients this directly. Most people should move through a treatment ladder, starting with the least invasive options that carry a real chance of resolving symptoms.
- Physical therapy. Targeted strengthening and mobility work can meaningfully help patients whose structural damage is minimal, though it has real limits once a significant annular tear is present.
- Anti-inflammatory medication. These can reduce pain temporarily, but they don’t address the structural tear generating the chronic inflammation.
- Activity modification and posture work. Useful for managing symptoms day to day, though postural changes are usually a compensatory response to pain rather than the root cause of it.
- Epidural or diagnostic injections. These can calm inflammation temporarily and, just as importantly, help confirm which level is generating your pain.
- Spinal fusion. Traditionally presented as the endpoint for disc related back pain, fusion removes the disc entirely and locks the adjacent vertebrae together with hardware. It eliminates motion at that level, which can relieve pain, but it also permanently changes how your spine moves and places additional stress on the discs above and below. For some patients, particularly those with instability or advanced collapse at the segment, fusion is genuinely the right call. For patients whose pain is coming from an inflamed annular tear without significant instability, it’s a much bigger intervention than the problem requires.
Here’s where I push back on the idea that fusion is your only surgical option. If conservative care hasn’t resolved your pain and imaging plus a Deuk Spine Exam® confirm the L4-L5 or L5-S1 disc itself, specifically the inflamed annular tear, is your pain generator, there’s a treatment option between “keep trying physical therapy” and “fuse the spine.”
How Deuk Laser Disc Repair® Treats Disc-Sourced DDD Pain
Deuk Laser Disc Repair® (DLDR®) is the procedure I developed specifically to address the inflamed annular tear that’s actually causing pain in disc-sourced DDD, rather than removing the disc or fusing the segment. Through a 4mm or 7mm incision, smaller than a dime, I access the posterior annulus and perform a debridement, removing the inflammatory tissue and any herniated nucleus pulposus material contributing to the irritation. I don’t seal the tear with any synthetic material. The tear heals naturally over roughly 9 to 12 months once the inflammatory source has been cleared.
Because there’s no bone drilling and no hardware, your spine keeps its natural motion at that segment. The procedure takes about 20 minutes per disc, is done on an outpatient basis, and most patients are walking within an hour. No opioids are required for post-operative pain control in the vast majority of cases. In my clinical experience across over 2,700 Deuk Laser Disc Repair® procedures, patients report an average of 99 percent pain relief for the treated pain source, with a complication rate of 0.01 percent.
This approach only makes sense, of course, when the disc itself has been confirmed as the pain generator. That’s the entire reason accurate diagnosis comes before any treatment recommendation in my practice.
Common Questions About Degenerative Disc Disease Treatment
Can degenerative disc disease at L4-L5 or L5-S1 heal on its own?
The degenerative changes themselves don’t reverse, but that doesn’t mean you’re stuck with pain forever. If the pain is coming from an inflamed annular tear, treating that tear directly, rather than waiting for the disc to regenerate, is what resolves symptoms.
Is fusion the only surgical option for degenerative disc disease?
No. Fusion is the option most patients are told about first, largely because it’s been available longest, but it isn’t the only surgical path for disc-sourced pain. A motion preserving option like DLDR® treats the same inflamed tissue without removing the disc or locking the segment with hardware.
How do I know if my back pain is coming from L4-L5, L5-S1, or somewhere else?
This requires correlating your symptom pattern, physical exam findings, and imaging together, which is exactly what the Deuk Spine Exam® is built to do. Guessing based on the MRI report alone leaves out half the picture.
Getting an Accurate Answer for Your L4-L5 or L5-S1 Diagnosis
If you’ve been told you have degenerative disc disease and you’re trying to figure out whether surgery is really necessary, the first step isn’t scheduling an operation. It’s confirming whether the disc flagged on your MRI is actually why you hurt. That single distinction changes everything about what comes next, from which conservative treatments are worth trying to whether a motion preserving procedure like DLDR® could apply to your case.
I offer a free MRI review for exactly this reason. Send us your imaging, and my team will help you understand what’s actually going on in your spine before you commit to any treatment path, conservative or surgical. If you’re dealing with chronic back pain at L4-L5 or L5-S1 and you want a clear answer instead of another guess, reach out to Deuk Spine Institute to schedule your free MRI review and take the first real step toward finding out what’s causing your pain.

No cost · No obligation
Live Pain Free
Upload your MRI for a free expert review by Dr. Ara Deukmedjian, M.D. — board-certified neurosurgeon. Ten minutes can change your life.


