

By Dr. Ara J. Deukmedjian, MD
Board Certified Neurosurgeon
Medically reviewed on June 23, 2026
Medical Disclaimer: The information provided within this article is for educational purposes only. Always consult a medical physician in regards to your own individual situation.
Key Points
✓ Lumbar radiculopathy is a pinched nerve in the low back, i.e., a compressed or irritated nerve root. ¹
✓ Affects up to 3–5% of adults in America, usually involving nerve roots at levels L4-L5 or L5-S1. ² ³
✓ Common causes include herniated disc, stenosis, osteophyte and spondylolisthesis. ¹
✓ Pain traveling into the legs, numbness, tingling and sometimes weakness characterize the condition. ¹
✓ Up to 25-50% do not experience recovery within 6 to 12 months without specific therapy. ⁴
✓ Urgent need for surgery occurs with bladder or bowel dysfunction, saddle anesthesia or progressive muscle weakness. ⁵
✓ Deuk Laser Disc Repair® treats pinched nerves due to herniated discs without fusion: 99.6% relief and 0.01% complications.
Pinched Nerve in the Lower Back?
A pinched nerve in the lower back is the everyday term for lumbar radiculopathy. A spinal nerve root that has been compressed as it leaves the spinal canal. A pair of nerve roots emerge between each pair of vertebral levels. In the lower back that is L1-S1. When one of those roots is pinched by a herniated disc, narrowed canal, ect. The result is the lower back pain plus radiating pain, numbness, tingling, or weakness moving down the buttock and leg along the sciatic nerve. ¹

The two bottom levels in the spine, L4-L5 and L5-S1, receive tremendous stress load and account for the vast majority of spinal nerve compressions and the corresponding sciatica- like symptoms people experience. Pain and the symptoms of numbness or tingling and weaknes that follow L5 or S1 in patients are often described as “ sciatica “ or “nerve pain”.
What Causes a Pinched Nerve in the Lower Back?
While a pinched nerve is the name most often given to this condition by patients and their doctors alike, it really isn’t a formal medical diagnosis. In order for proper treatment to begin, one must know what structurally has caused the pinching. Pinched nerves are commonly caused by:
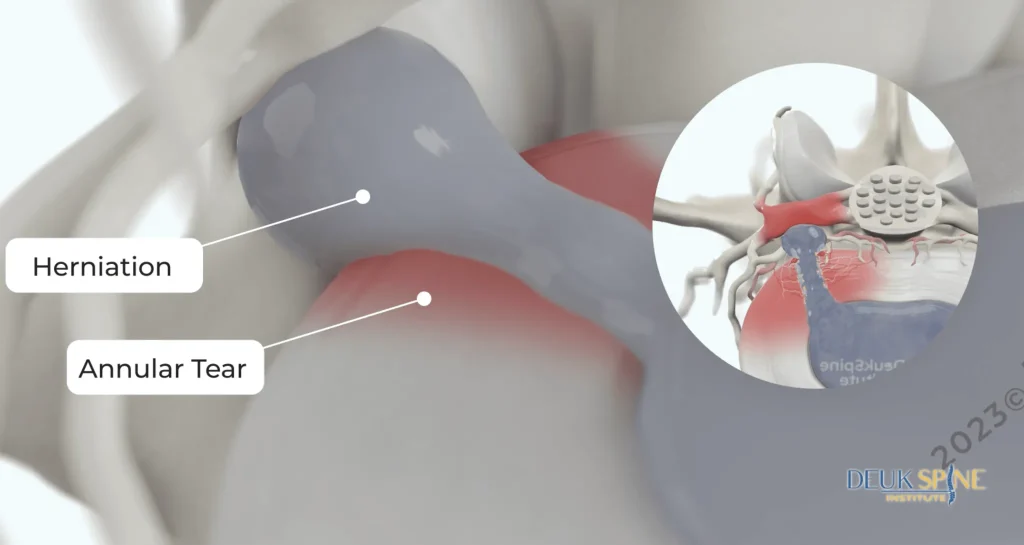
1. Herniated or bulging disc
There is a tough outer ring (annulus fibrosus) on each intervertebral disc, and a softer jelly-like center (nucleus pulposus). If the annulus cracks or tears the nucleus gel material is then forced outward and comes into contact with an adjacent nerve root. The disc also releases chemical inflammatory material that is irritating and noxious to the nerve, which explains why even small ruptures can cause terrible leg pain. Actually, this condition represents the most frequent single cause of acute lumbar radiculopathy in young and middle aged adults.
2. Spinal stenosis
The most frequent cause is related to degeneration with the natural process of aging and/or bony remodeling to cause a reduction in the caliber of the central spinal canal or foramena (a side opening between vertebrae that the nerve emerges from). Thickened and degenerative ligament and the accumulation of bone spurs are common offenders. The patients present with leg symptoms of heaviness, pain, or cramps that are exacerbated by prolonged standing or walking and are most frequently alleviated with sitting and forward bending with the posture one maintains while walking behind a shopping cart (shopping-card relief.) This causes most commonly l3-l5 radiculopathy in older people.
3. Degenerative disc disease and bone spurs
As discs degenerate with age they become compressed and their height decrease and the body then begins laying down extra bone on the edges of the vertebral body, which may then extend into the foramen space and compress the nerve root. This is the most common source of the foramen being too small for the nerve to fit as one moves their neck. This is the most common source of l3, l4 and l5 radiculopathy with a variety of diagnoses possible in any one given case with the most frequent being the aforementioned issues.
4. Spondylolisthesis
When one vertebral body slips forward over the body beneath it there will naturally be some reduction in the space in the foramena that has the nerve emerge and go along its course which can cause pinching. In older individuals with instability, this can lead to l5 radiculopathy.
5. Piriformis syndrome and extraspinal causes
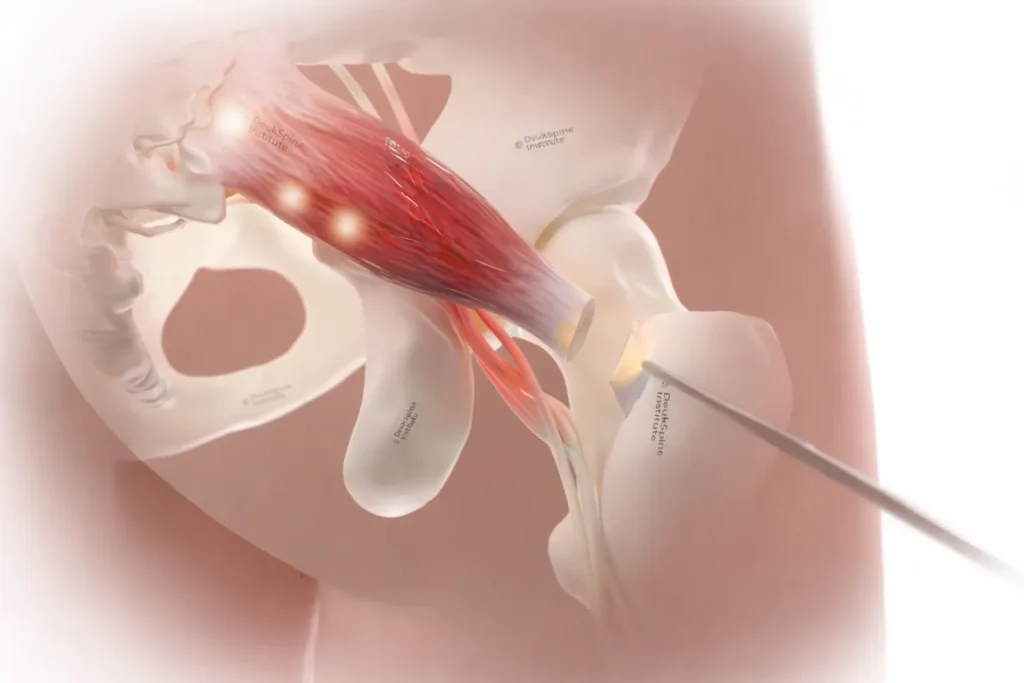
It should be known that all leg pain does not come from the inside of the spine. The piriformis muscle located deep within the buttocks can cause the sciatic nerve to get irritated or compressed as the muscle either passes underneath or through the muscle fiber, which will cause some leg pain that mimics a herniated disc. Trauma, tumors, and infections are less frequent causes that should be addressed.
Symptoms: What a Pinched Nerve Actually Feels Like
Pinched lumbar nerve symptoms are pain that does not stay in the back. It follows the path of the affected nerve into the leg. Specific patterns include: ¹
What Is L5 Radiculopathy?
- L5 nerve root: Pain on the outer part of the back of the thigh, the side and the outside of the lower leg, onto the dorsum (top of) the foot and into the big toe, or Foot drop and inability to pull the foot at the ankle upwards
- L1-L4 nerve root: Pain on the front of the thigh and the medial shin
- S1 nerve root: Pain on the posterior thigh and calf, to the outer aspect of the foot. Weak ability to push through the forefoot.
Pain radiating from the nerve root may involve numbness or pins-and-needles and may lead to muscle weakness in the leg.
Weakness, including difficulty with weight-bearing may be present along with muscle atrophy, which develops gradually. Any sitting for extended periods, bending forwards, or increased straining through coughing or sneezing exacerbates symptoms and pain from any spinal nerve irritation that produces significant inflammation within or about the nerve roots. Lying flat with a pillow beneath the knee can often provide relief. A pinched nerve can indeed cause problems in itself; but it only becomes an emergency when it directly impacts crucial bodily systems or nerve damage that can cause progressive disability, such as by impacting the bowel and bladder control in this particular condition; if any loss of control over your bowel or bladder and new inability to urinate and new groin,buttock or inner- thigh pain happens simultaneously the result could be an ongoing serious problem if not promptly addressed.
Rapid weakness or developing leg paralysis: If the loss or rapidly progress weakness of a limb or even two is happening.
These can signal cauda equina syndrome, spinal infection, fracture, or tumor and a delay of even hours can produce permanent damage. ⁵
How a Pinched Nerve Is Diagnosed
Proper work-up is the thing that saves patients years of guessing. Workup may consist of:
- Physical examination and history that include not only which symptoms the patient experiences but also exactly where those symptoms occur to precisely locate the involved nerve root. Provocative tests, such as straight-leg raise, will typically show the nerve root to be under tension.
- Magnetic Resonance Imagining(MRI) which is the modality of choice for soft tissues and details discs and nerve compression.
- CT scan or x-rays may be obtained if the bones need to be specifically assessed, i.e., instability or fractures.
- Electromyogram/nerve conduction studies may be of value to rule out compression other than at the spinal nerve.
Imaging alone is not the diagnosis. MRI abnormalities are extremely common in people with no pain whatsoever, so the findings must correlate with the physical exam and the symptom pattern to identify the true pain generator. This is the single biggest mistake in spine medicine.
Conservative Treatment: The First Six Weeks

For non-emergency pinched nerves, the standard of care is 6 to 12 weeks of conservative treatment first. ⁶ The majority of acute nerve pain improves in this timeframe without surgery. Reasonable measures include:
- Activity modification (avoid prolonged sitting, heavy lifting, and forward bending) while staying generally active. Strict bed rest is no longer recommended.
- Physical therapy focused on core stabilization, hip mobility, and nerve glide techniques.
- NSAIDs and short courses of oral steroids to control inflammation around the nerve root. ³
- Neuropathic pain medications (such as gabapentin) in selected cases. ³
- Epidural steroid injections for severe, persistent radicular pain that has not responded to oral medication.
What the data shows you should know: although conservative care helps most people initially, 25% to 50% of patients with lumbar radiculopathy still have pain one year later. ⁴ If you are still in significant pain after six weeks of honest conservative effort, the problem is no longer “give it more time. It is identify the structural cause and treat it directly.
When to Consider Surgery
Surgery is appropriate when any of the following apply: ⁵ ⁶
- Red-flag Signs: cauda equina, progressive weakness, infection, tumor, unstable fracture
- Persistent radicular pain beyond 6–12 weeks of appropriate conservative care
- Objective neurological deficits: weakness, reflex loss & atrophy on exam
- An MRI finding that clearly correlates with the nerve pain
The question is no longer whether to act, but which procedure causes the least permanent change to your spine while reliably eliminating the compression.
The Problem with Invasive Lumbar Surgery
Traditional open surgery approaches an pinched lumbar nerve with: laminectomy, discectomy, and spinal fusion. These range from reasonable to overkill depending on the case. Fusion in particular is frequently recommended for problems that do not require it. Once a level is fused, the motion segment is gone, and the discs above and below now absorb the load that segment used to share. Which could lead to adjacent segment disease. This often pushes patients into a second and sometimes third surgery years later.
Equally important: a meaningful share of spine surgeries do not fully relieve the original pain. Failed back surgery syndrome is estimated to affect 10 to 40 percent of spine surgery patients, with the highest rates after multi-level operations and fusions. This is why a second opinion before spine surgery is one of the most protective steps a patient can take.
How Deuk Laser Disc Repair® Treats the Pinched Nerve at Its Source
When the structural cause of a pinched lumbar nerve is a contained or extruded disc (the most common scenario), Deuk Laser Disc Repair® treats it directly without the trade-offs of traditional surgery.
This minimally invasive surgery is an outpatient endoscopic procedure performed under light sedation through a 4 to 7 millimeter incision that is smaller than a dime. Deuk Spine Institute uses endoscopic visualization, a Holmium YAG laser removes only the inflamed, pain generating tissue inside the disc. Including the torn annular fibers and the herniated nucleus pulposus pressing on the nerve. The healthy disc surrounding the bone, the ligaments, and the segment’s natural motion are all preserved. Nothing is fused. No metal hardware is implanted. No artificial disc is inserted.
Across more than 2,750 procedures, Deuk Laser Disc Repair® has delivered an average pain relief rate of 99.6%, a 0.01% complication rate, and a 0% infection rate. Each disc is treated in roughly 20 minutes. Our patients go home within an hour and return to normal activities within three days with light restrictions.
Summary
A pinched nerve in the lower spine is not random and rarely hopeless. It is a specific, identifiable problem with a specific, identifiable cause, most often a disc, a narrowed canal, or a bone spur compressing a single named nerve root. The right answer depends entirely on which structure is doing the pinching.
For most patients, the path looks like this: identify the exact cause with a proper exam and MRI, give appropriate conservative care a real 6 to 12 weeks, and if pain persists, choose the treatment that fixes the cause while changing the spine as little as possible. Fusion should be reserved for the cases that biomechanically need it, not used as a default. When the cause is disc-driven, a motion-preserving laser procedure can eliminate the compression in 20 minutes without sacrificing the rest of your spine.
If you are months into a pinched nerve and conservative care is not getting you back to the life you had, you have options. They are just not always the ones the first surgeon you meet will offer.
Treat the disc. Save the motion.
Find out if your pinched nerve can be fixed without a fusion.
Months into sciatica or a pinched nerve and conservative care isn’t working? Send your MRI for a free review by Dr. Deukmedjian and learn whether a no-fusion, motion-preserving option like Deuk Laser Disc Repair® could treat your specific condition.
- 99.6%
- Average pain relief
- 0.01%
- Complication rate
- 2,750+
- Procedures since 2004
FAQ’s
How long before a pinched nerve in the lower back can heal?
Nerve pain for most people improves within 6 to 12 weeks of appropriate conservative care. 25% to 50% of patients still have pain symptoms 1 year later without targeted treatment, which is why persistent symptoms beyond six weeks warrant a precise diagnosis instead of prolong waiting. ⁴ ⁶
Will a pinched nerve heal on it’s own?
Possibly, yes, when the cause is inflammation around a small disc bulge. The human body can reabsorb portions of herniated disc material over time. A pinched nerve caused by: spinal stenosis, bone spurs, or a large extrusion is far less likely to resolve without treatment and may worsen as degenerative changes progress. ¹
Is Sciatica and a pinched nerve different?
Sciatica is one form of lumbar radiculopathy or nerve pain. Discomfort along the sciatic nerve distribution (back of the thigh, calf, and foot) caused by irritation of the L1-S1 nerve roots. All sciatica is caused by a pinched nerve, but not every pinched lumbar nerve is sciatica. An L4 pinched nerve, for example, causes pain in the front of the thigh, not in the lower back traveling down the leg. ¹
Is walking good for a pinched nerve in the lower back?
Yes. Walking is usually one of the better activities for a pinched nerve because it keeps the spine mobile without loading it heavily. People with spinal stenosis are an exception. Some find walking worsens leg symptoms, while sitting or leaning forward relieves them. Pain that worsens with walking and improves with leaning forward is a strong clinical clue for stenosis. ¹
When should I medical help for a pinched nerve in my lower back?
See a doctor promptly if pain is severe, lasts longer than a week or two: includes weakness in the leg or foot, or follows a significant injury. Seek emergency care immediately for loss of bladder or bowel control, groin numbness, or rapidly worsening weakness. These are signs of cauda equina syndrome, a true surgical emergency. ⁵
Will I need surgery for my pinched nerve?
Surgery is needed when there is a clear structural cause on the MRI. Also there are neurological deficits or red-flag symptoms. ⁶ When surgery is appropriate, motion-preserving options like Deuk Laser Disc Repair® should be considered before fusion whenever the underlying cause is disc-driven.
Is Deuk Laser Disc Repair® right for my pinched nerve?
It is the right answer for structural problems in a disc problem. Herniation, bulge, annular tear, or contained disc-driven nerve compression. It will not help with for true instability, significant deformity, fractures, tumors, or infections. A free MRI review identifies which category your specific condition falls into.
Sources
- Berry JA, Elia C, Saini HS, Miulli DE. A Review of Lumbar Radiculopathy, Diagnosis, and Treatment. Cureus. 2019;11(10):e5934.
- Alentado VJ, Lubelski D, Steinmetz MP, Benzel EC, Mroz TE. Optimal Duration of Conservative Management Prior to Surgery for Cervical and Lumbar Radiculopathy. Global Spine J. 2014;4(4):279–286.
- Doral Health & Wellness. Lumbar Radiculopathy Management.
- Rehabilitation outcomes in patients with lumbar radiculopathy due to disc herniation: a multicenter prospective study. PMC.
- Rider LS, Marra EM. Cauda Equina and Conus Medullaris Syndromes. StatPearls. National Library of Medicine.
- Cho S, Lim YC, Kim EJ, et al. Analysis of Conservative Treatment Trends for Lumbar Disc Herniation with Radiculopathy. Healthcare (Basel). 2023;11(16):2353.


