


By Dr. Ara Deukmedjian, MD
Board-Certified Neurosurgeon, Deuk Spine Institute
Medically reviewed on March 25, 2026
Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
Key Points
Before diving into the details, here is what you need to know about disc displacement:
✓ Disc displacement is extremely common: Back pain affects up to 80% of the population at some point in their lives, and displaced or herniated discs are among the most frequent structural causes.
✓ There are four distinct types: Herniated discs, bulging discs, collapsed discs, and torn discs each involve different structural changes and require different treatment approaches.
✓ Conservative treatment is appropriate first for most patients: Research confirms that the majority of disc displacement cases improve with physical therapy, medications, and activity modification. Surgery is reserved for cases with neurological deficits or failed conservative care.
✓ Timing matters when surgery is needed: A 2025 systematic review found that early surgery, within 48 hours to 6 weeks of onset, achieves recovery rates above 90% for patients with motor deficits, while delayed surgery results in significantly worse outcomes.
✓ Not all surgeries are equal: Traditional open procedures including laminectomy, microdiscectomy, and spinal fusion carry significantly higher complication profiles, longer recovery times, and greater structural disruption than truly minimally invasive alternatives.
✓ Deuk Laser Disc Repair® treats the source: Unlike procedures that simply decompress without healing, DLDR removes the damaged tissue and treats the annular tear directly, achieving a 99.6% success rate across more than 2,000 procedures with zero complications.
✓ Motion preservation matters long-term: Fusion eliminates motion at the treated level and accelerates degeneration at adjacent levels. DLDR preserves the natural movement of the spine permanently.
✓ A second opinion can change your outcome: Many patients are offered only traditional fusion or open discectomy because those are the procedures their surgeon performs. An evaluation by a specialist in minimally invasive spine care may reveal far better options.

Disc Displacement: Types, Causes, Symptoms, and Treatment Options
Back pain is one of the most prevalent health conditions in the world, affecting up to 80% of people at some point during their lives. 1 Its effects span the full spectrum, from minor aches that resolve on their own to severe, disabling pain that significantly limits daily function. Among the many structural causes of spine-related pain, disc displacement stands out as one of the most common and consequential. When a disc in the spinal column shifts, herniates, or deteriorates significantly, it can press against spinal nerves and the cord itself, producing pain, numbness, weakness, and other neurological symptoms that require prompt evaluation and targeted treatment.
This comprehensive guide explains what disc displacement is, what causes it, how it presents clinically, what the different types involve, and what treatment options, from conservative care to the most advanced minimally invasive surgery, are available today.
What Is Disc Displacement?
Disc displacement is a broad clinical term describing any condition in which an intervertebral disc shifts, herniates, or deteriorates in a way that moves it outside its normal anatomical boundaries, compressing nearby spinal nerves or the spinal cord. The spinal column consists of 33 vertebrae separated by 23 intervertebral discs. Each disc acts as a shock absorber between the bony vertebrae, allowing the spine to flex, rotate, and bear weight. When a disc is displaced, these functions are compromised and pain, instability, and neurological symptoms can follow.
Disc displacement is generally categorized as either traumatic or non-traumatic in origin. Traumatic disc displacement results from an acute injury such as a vehicle accident, a sports collision, or a fall that generates sudden and significant spinal loading. Non-traumatic displacement develops gradually through degenerative processes such as osteoarthritis, age-related disc dehydration, and cumulative mechanical stress. 2 Treatment approaches and recovery timelines differ meaningfully between these two categories. According to StatPearls, lumbar disc herniation, the most common form of disc displacement, is defined as the displacement of nucleus pulposus material beyond the intervertebral space and represents one of the most frequent causes of radiculopathy and low back pain worldwide. 3
Most disc displacements occur in the lower back, specifically the lumbar spine, where mechanical loading is greatest. The next most common location is the cervical spine in the neck. Thoracic disc displacement is less frequent due to the stabilizing effect of the rib cage. Pain is typically felt on one side of the body and may worsen with sustained postures, activity, or specific movements such as bending and lifting.
What Causes Disc Displacement?
Multiple factors can contribute to the development of a displaced disc, and in most patients, more than one is present
Age-Related Degeneration
As people age, the intervertebral discs gradually lose water content, becoming less supple and more prone to cracking, collapsing, or bulging. The nucleus pulposus, the gel-like inner core of the disc, becomes drier and less able to absorb mechanical loads effectively. This degeneration begins as early as the third decade of life and accelerates over time, making disc displacement increasingly common after age 35.
Injury and Trauma
A single acute injury can displace a disc that was previously healthy. Vehicle accidents, falls from height, sports contact injuries, and workplace accidents can all generate sufficient spinal loading to cause acute disc herniation, fracture of the vertebral endplate adjacent to the disc, or avulsion of disc material into the spinal canal. Workers in physically demanding occupations, including construction, warehousing, and healthcare, face elevated risk from cumulative microtrauma as well as acute injury events.

Improper Lifting Mechanics
Lifting heavy objects with poor technique, particularly with a flexed spine rather than using the leg muscles, generates disproportionate compressive and shear forces through the lumbar discs. Repeated improper lifting is one of the most common occupational contributors to lumbar disc displacement.

Obesity and Excess Body Weight
Excess body weight increases the baseline mechanical load carried by the intervertebral discs, particularly in the lumbar spine, across every posture and activity. Obesity is consistently identified as an independent risk factor for disc degeneration and displacement, accelerating the wear-and-tear process significantly.
Underlying Spinal Conditions
Structural conditions including scoliosis, kyphosis, and spondylolisthesis alter the distribution of mechanical forces through the spinal column. When the spine is structurally abnormal, certain discs bear disproportionate load, increasing their vulnerability to displacement and degeneration over time.

Genetic Predisposition
Genetic factors play a meaningful role in disc health and degeneration. Research has identified hereditary components in disc matrix composition, disc height maintenance, and susceptibility to early degeneration, meaning that some individuals are structurally predisposed to disc displacement regardless of their lifestyle.
Sedentary Lifestyle
Physical inactivity weakens the muscles that support the spine, reduces the nutrient exchange that keeps discs healthy, and increases the vulnerability of spinal structures to displacement under load. Sedentary individuals have higher rates of disc degeneration and symptomatic disc disease than those who engage in regular physical activity.
The Four Types of Disc Displacement
Understanding the specific type of disc displacement affecting you is essential for choosing the right treatment. Each type involves distinct structural changes and may respond differently to various therapeutic approaches.
1. Herniated Disc
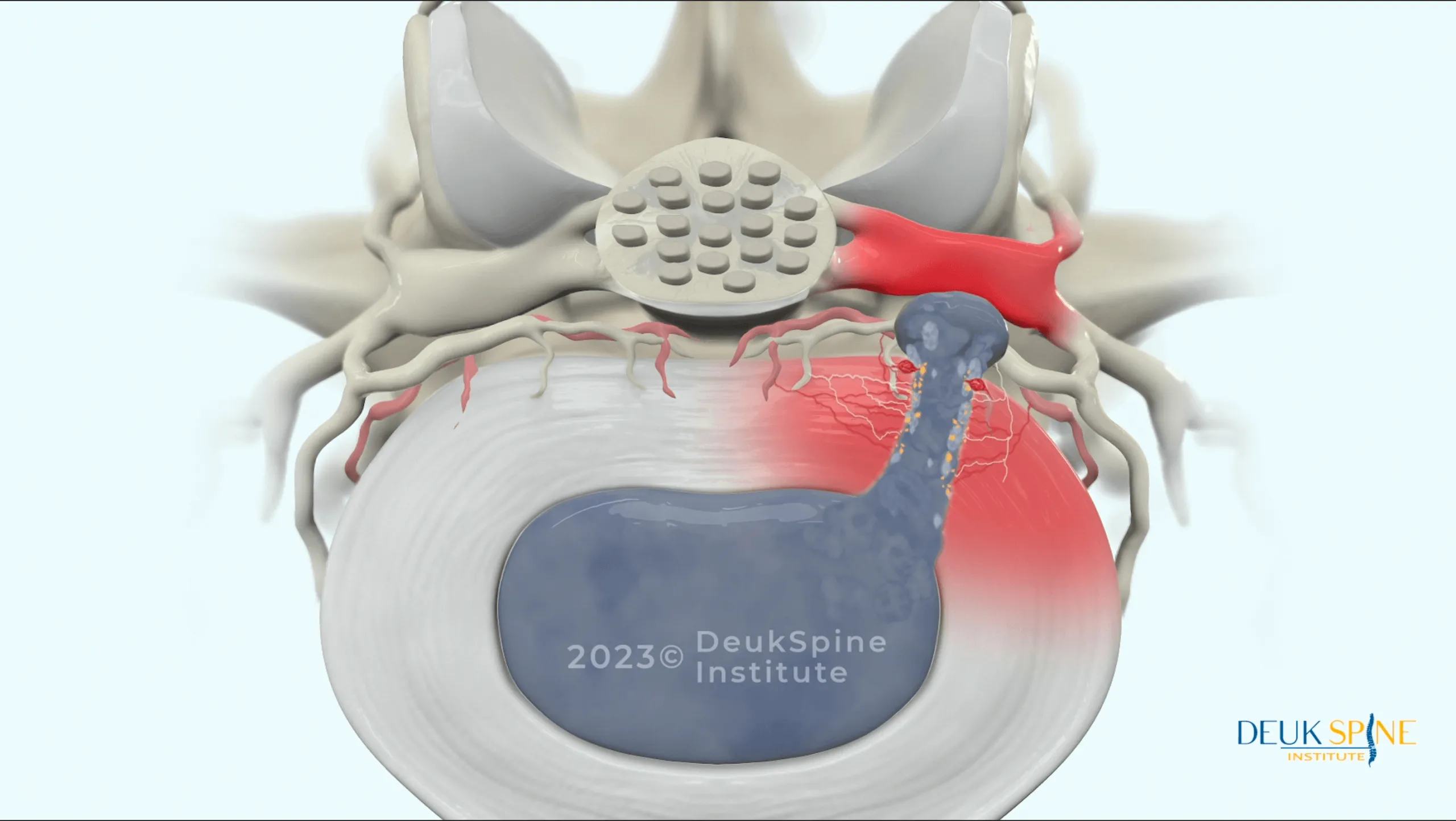
A herniated disc occurs when the outer wall of the disc, the annulus fibrosus, develops a tear and the inner gel-like material, the nucleus pulposus, pushes backward through the tear into the spinal canal or neural foramen. This herniated material can directly compress adjacent spinal nerve roots or the cord itself, triggering inflammation, irritation, and a characteristic pattern of radiating pain.
Herniated discs are classified by the vertebral levels involved. Common cervical herniations include C4-C5. Common lumbar herniations include L4-L5 and L5-S1. The specific level determines the nerve affected and the distribution of symptoms. A lumbar herniation at L4-L5, for example, often produces sciatic pain radiating down the leg.
Disc herniation can be caused by cumulative wear and tear, but it can also result suddenly from acute trauma. A 2024 systematic review published in PMC confirmed that disc herniation is the displacement of nucleus pulposus beyond the intervertebral space, that degeneration and trauma are the primary mechanisms, and that minimally invasive endoscopic discectomy techniques show the best results in terms of postoperative pain and functional recovery among surgical options. 4
2. Bulging Disc
A bulging disc occurs when the disc’s outer wall weakens and the internal pressure of the disc causes the entire disc to expand outward beyond its normal footprint, without necessarily tearing the outer wall completely. Unlike a herniated disc, a bulging disc does not release its inner material, but the outward expansion can still encroach on the spinal canal and compress nearby nerves.
Bulging discs are particularly common in the lumbar spine. A lumbar bulging disc may produce no symptoms initially, but over time it can cause buttock pain, leg pain, and the radiating symptoms of sciatica as it gradually impinges on nerve roots. Because the disc will not return to its original position on its own and the disc tissue becomes progressively drier and less flexible with age, untreated bulging discs tend to worsen over time.
Bulging and herniated discs are frequently confused but represent different stages and mechanisms of disc failure. Both warrant evaluation by a spine specialist.
3. Collapsed Disc
A collapsed disc, also called disc height loss or degenerative disc disease in advanced form, occurs when the disc loses a significant proportion of its normal height through severe degeneration or injury. As the disc collapses, the space between adjacent vertebrae decreases, which can cause the facet joints to take on abnormal loading, trigger bone spur formation, and narrow the neural foramen through which nerve roots exit the spinal column.
The resulting pressure on adjacent nerve roots and surrounding structures produces pain, numbness, tingling, and weakness. In severe cases, collapsed disc segments can cause spinal instability requiring surgical stabilization. Treatment depends on the extent of collapse, the degree of neurological involvement, and the patient’s overall spinal health.
4. Torn Disc (Annular Tear)
A torn disc involves damage to the annulus fibrosus, the tough outer collagen wall of the intervertebral disc. Annular tears can occur from trauma, from cumulative mechanical stress, or as part of the broader degenerative process. They are clinically significant for two reasons: first, they can allow the inner nucleus pulposus to herniate; second, the torn annular tissue itself generates a potent inflammatory response that is a primary source of discogenic pain even without herniation.
Discogenic pain, meaning pain originating from within the disc itself rather than from nerve compression, is frequently underdiagnosed because it does not always produce the dramatic radiating symptoms associated with herniation. Patients may experience deep, achy, difficult-to-localize back pain that worsens with loading, flexion, and sustained postures. Annular tears are best identified on MRI, specifically high-intensity zone (HIZ) lesions visible on T2-weighted sequences.
Symptoms of Disc Displacement
Symptoms vary significantly depending on the type of displacement, the spinal level affected, and whether the spinal cord, individual nerve roots, or both are involved.
Common symptoms across all types:
- Localized neck or back pain at the affected spinal level
- Radiating pain traveling into the arm (cervical displacement) or leg (lumbar displacement) along a specific nerve distribution
- Numbness, tingling, or a “pins and needles” sensation in the extremities
- Muscle weakness in specific groups of the arm, hand, leg, or foot
- Muscle spasms adjacent to the affected level
- Pain that intensifies with sitting, standing, bending, or specific movements
Symptoms requiring urgent evaluation:
- Progressive weakness that is worsening over days
- Loss of bladder or bowel control (a sign of cauda equina syndrome, a surgical emergency)
- Bilateral leg symptoms or difficulty walking
- Rapidly increasing neurological deficits including loss of sensation
If you are experiencing any of these symptoms, evaluation by a spine specialist is essential. Delayed treatment of progressive neurological deficits is associated with significantly worse outcomes.
Diagnosing Disc Displacement
Discover a new solution to your back pain problem with a free virtual MRI review from Dr. Ara Deukmedjian. Avoid fusion and get lasting back pain relief.

An accurate diagnosis requires a combination of clinical assessment and advanced imaging.
Physical and neurological examination: The physician evaluates reflexes, sensation, motor strength, and provocative signs such as the straight leg raise test (for lumbar radiculopathy) or the Spurling test (for cervical radiculopathy) to identify the pattern of neurological involvement and narrow the differential diagnosis.
MRI: The gold standard for evaluating disc displacement. MRI clearly visualizes disc herniations, bulging discs, annular tears, nerve root compression, and spinal cord involvement. The specific appearance on MRI guides treatment decisions and surgical planning.
CT scan: Useful for evaluating bony structures, bone spurs, and the degree of foraminal narrowing. Often combined with myelography in complex cases.
Electrodiagnostic studies: Electromyography (EMG) and nerve conduction studies (NCS) can confirm nerve root involvement and help differentiate disc-related radiculopathy from peripheral nerve entrapment.
Conservative Treatment for Disc Displacement
For the majority of patients with disc displacement who do not have significant neurological deficits, conservative management is the appropriate first step. Research consistently confirms that most patients improve substantially with non-surgical care.
A 2025 systematic review published in the Journal of Clinical Medicine evaluated non-surgical treatment options for lumbar disc herniation and found that exercise therapy, platelet-rich plasma injections, and structured rehabilitation programs all contribute meaningfully to symptom relief and functional recovery, supporting a structured conservative approach as the primary initial treatment in most cases. 5
A 2025 PMC case series further documented that lumbar disc herniations can experience spontaneous resorption over time with conservative management, and that clinical symptoms frequently improve in parallel with radiological resolution of the herniation, providing further evidence for conservative care as a first approach in appropriate patients. 6
Physical Therapy
A structured physical therapy program targeting the specific spinal level and disc pathology is one of the most important components of conservative disc displacement management. Therapy focuses on core strengthening to reduce disc loading, postural correction, flexibility training, and aerobic conditioning. A 2025 meta-analysis of randomized controlled trials confirmed that exercise therapy significantly improved pain scores, disability index scores, and quality-of-life measures in patients with lumbar disc herniation. 7

Medications
Non-steroidal anti-inflammatory drugs (NSAIDs) reduce both pain and the inflammatory component of disc-related symptoms. Short courses of oral corticosteroids can be useful for managing acute severe flares. Nerve-specific medications such as gabapentinoids address the neuropathic component of radiating pain. Muscle relaxants are used short-term for associated spasm.
Epidural Steroid Injections
Epidural steroid injections (ESIs) deliver corticosteroids directly to the epidural space adjacent to the compressed nerve root. They can provide meaningful temporary pain relief, allowing patients to engage more effectively in physical therapy and facilitating recovery. While their benefits are temporary and do not address the structural disc problem, ESIs are a valuable component of multimodal conservative care.
Activity Modification
During acute phases, avoiding activities and positions that significantly worsen symptoms allows the disc and surrounding structures to begin recovery. Ergonomic adjustments to workstations and sleeping positions can reduce disc loading and accelerate improvement.
When Surgery Is Necessary for Disc Displacement
When conservative treatment fails to provide adequate relief after an appropriate trial of care, typically 4 to 6 weeks of structured treatment, or when neurological deficits are present or progressing, surgical intervention becomes appropriate.
A 2025 systematic review published in ScienceDirect examining indications for surgery in lumbar disc herniation found that early surgery, within 48 hours to 6 weeks of symptom onset, achieved recovery rates above 90% for patients with motor deficits, while delayed surgery (more than 6 weeks) resulted in prolonged symptoms and significantly worse outcomes, particularly in severe cases. 8 The most consistent surgical indications across 20 reviewed studies were imaging-confirmed nerve root compression and severe or refractory pain.
A 2025 systematic review of treatment guidelines for lumbar disc herniation published in Neurospine similarly concluded that surgery frequently results in immediate resolution of radicular pain, and that patients who met surgical indications and underwent surgery had better improvement than those managed conservatively when neurological deficits were present. 9
Emergency surgery is required for cauda equina syndrome, characterized by sudden onset of bilateral leg weakness, saddle area numbness, and loss of bladder or bowel control. This is a spinal emergency requiring immediate evaluation and surgical decompression.
Surgical Treatment Options for Disc Displacement
The surgical approach chosen matters enormously for both short-term recovery and long-term spinal health. Not all spine surgery is equivalent.
1. Deuk Laser Disc Repair: The Gold Standard in Minimally Invasive Disc Surgery
Deuk Laser Disc Repair ® (DLDR) is the most advanced surgical option available for disc displacement caused by herniated discs, bulging discs, annular tears, and related degenerative disc conditions. It is a truly minimally invasive, motion-preserving procedure that treats the actual structural source of pain, not just its symptoms.
What it is: DLDR is performed through an incision of 4 to 7 mm, approximately the size of a pencil eraser, under sedation in an outpatient surgical center. There is no hospital admission, no general anesthesia in most cases, and no overnight stay. The entire procedure takes approximately one hour.
How it works: Using live fluoroscopic imaging, the surgeon guides a narrow tube directly into the symptomatic disc. A high-definition endoscopic camera is inserted to provide real-time visualization of the disc interior. A precision Holmium:YAG laser is then used to remove only the 5 to 10% of disc tissue that is herniated or inflamed, leaving the healthy disc structure completely intact. Critically, the laser also treats the annular tear itself, the primary source of discogenic pain, promoting natural healing of the disc wall. Bones, muscles, and surrounding soft tissues are not cut, drilled, or otherwise disturbed.
Why DLDR is superior to traditional disc surgery:
- No fusion: The spine retains its full natural range of motion permanently. Adjacent segments are not subjected to increased stress, eliminating the risk of adjacent segment disease.
- No hardware: No screws, rods, plates, or cages are implanted. There are no hardware-related complications, no metal detector concerns, and no need for future hardware removal.
- No bone removal: Traditional open procedures including laminectomy and microdiscectomy require removal of bone and facet joint material, creating spinal instability that often leads to fusion. DLDR requires none of this.
- No muscle disruption: The approach does not cut through the major spinal muscles, eliminating the severe postoperative pain associated with open spine surgery.
- Rapid recovery: Most patients walk out of the surgical center within one hour of the procedure. The majority return to daily activities within two to three days and to desk work within a week. Compare this with the 6 to 12 weeks of restricted activity and months of recovery required after fusion or open laminectomy.
- No opioids: Patients do not require narcotic pain medication after DLDR. Traditional open spine surgeries generate such significant tissue trauma that prolonged opioid use is typically necessary for recovery. DLDR eliminates this need entirely.
- Proven results: Over 20 years and more than 2,000 procedures, DLDR has achieved a 99.6% success rate in eliminating back and neck pain caused by disc displacement, with zero complications on record.
Conditions DLDR treats:
- Herniated discs (cervical and lumbar)
- Bulging discs
- Annular tears
- Sciatica and lumbar radiculopathy
- Cervical radiculopathy and pinched nerves
- Degenerative disc disease
- Disc-related spinal stenosis
- Chronic back and neck pain
Cost and access: Deuk Spine Institute accepts workers’ compensation, personal injury, auto accident insurance, and patients with minimal or no coverage. Submit your MRI for a free review to determine whether you are a candidate.
2. Laminectomy and Foraminotomy
A laminectomy removes the lamina, the bony plate at the back of the vertebra, to decompress nerves by creating more space in the spinal canal. A foraminotomy widens the neural foramen, the opening through which nerve roots exit the spine, to relieve foraminal stenosis and nerve root compression.
Both procedures are more invasive than DLDR. They require cutting through muscle, removing bone, and in the case of laminectomy, frequently create enough spinal instability that fusion is performed simultaneously. Recovery typically takes 2 to 6 months. The procedures relieve nerve compression but do not treat the disc itself or the annular tear contributing to discogenic pain.
3. Traditional Spinal Fusion
Spinal fusion involves removing the disc, placing bone graft material between the vertebrae, and securing the construct with metal hardware including screws, rods, and cages. The adjacent vertebrae are permanently joined as a single solid bone segment. Fusion is appropriate for conditions involving true spinal instability, spondylolisthesis with significant slippage, or severe deformity that requires structural correction.
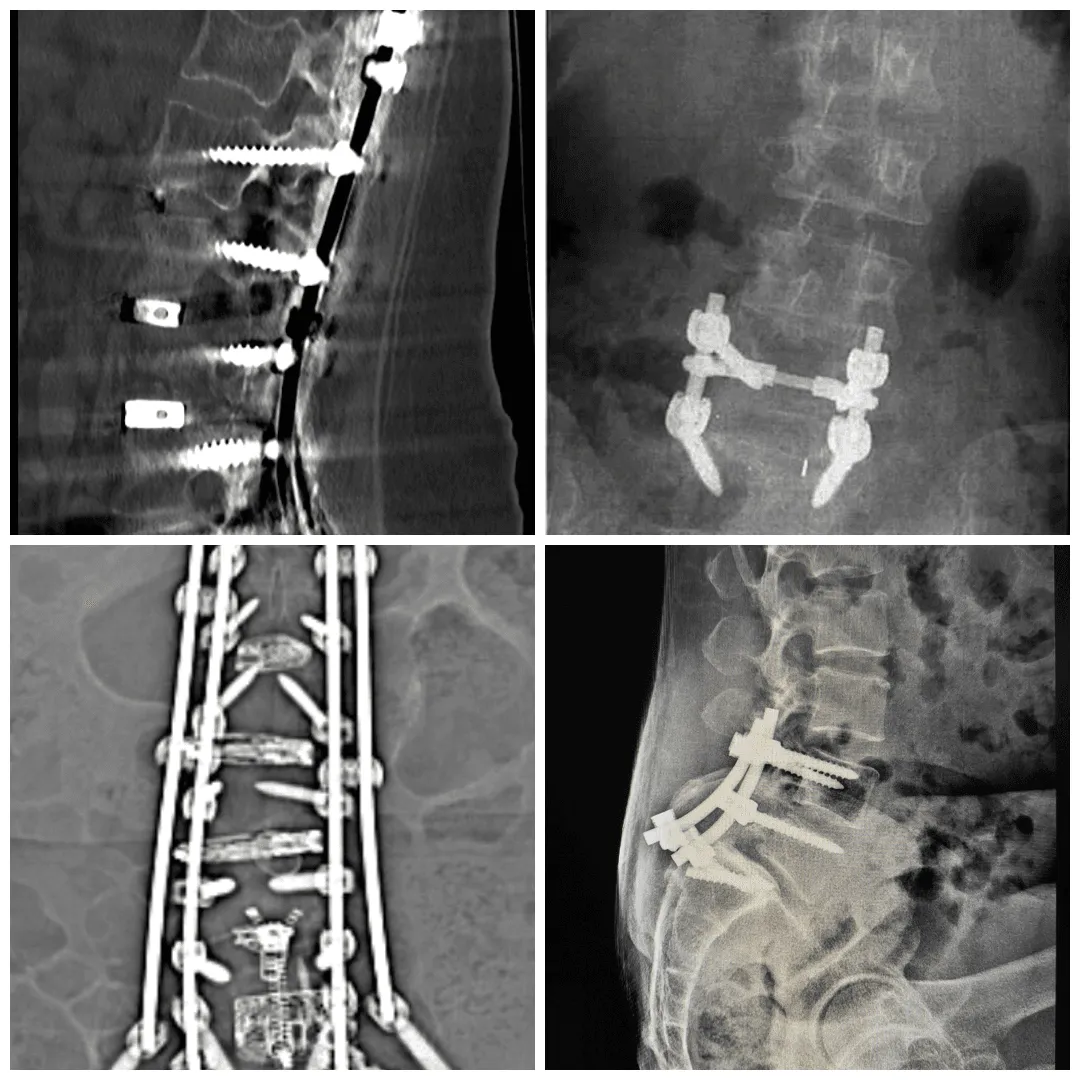
For disc displacement without spinal instability, fusion is generally not the optimal treatment. It permanently eliminates motion at the fused level, transfers biomechanical stress to adjacent segments, and carries a well-documented risk of adjacent segment disease. Recovery takes 6 to 12 months and involves extensive activity restrictions. Hardware complications including screw loosening and cage subsidence require reoperation in a meaningful percentage of patients.
4. Artificial Disc Replacement
Artificial disc replacement removes the damaged disc and replaces it with a synthetic implant designed to preserve motion at the treated level. It is an alternative to fusion for single-level disc disease in selected patients. The procedure requires an anterior (abdominal) approach, which carries risks related to proximity to major blood vessels and abdominal organs. Implant dislocation, wear, loosening, and infection are recognized complications. Recovery takes 6 to 12 weeks for return to light activity.
Benefits and Risks of Disc Surgery
Understanding what disc surgery can and cannot offer is essential for informed decision-making.
Benefits
- Elimination or significant reduction of radicular pain and neurological symptoms
- Reduced dependence on pain medications
- Ability to return to work and normal activities
- Prevention of permanent neurological damage when surgery is performed at the appropriate time
- With DLDR specifically: motion preservation, no hardware, outpatient recovery, and return to daily life within days
Risks (Traditional Open Surgery)
- Anesthesia reactions including allergic responses and respiratory complications
- Surgical site infection
- Bleeding requiring transfusion
- Deep vein thrombosis or pulmonary embolism
- Nerve injury causing chronic pain, weakness, or sensory loss
- Cerebrospinal fluid leak from dural tear
- Incomplete removal of herniated material requiring revision surgery
- Spinal instability from bone and joint removal
- Adjacent segment disease in fusion cases
With DLDR, the risk profile is dramatically reduced due to the absence of bone removal, hardware, muscle cutting, and fusion.
Talk with Dr. Deuk about how Deuk Laser Disc Repair® can help you live pain-free again. Start your recovery journey today with a free 10-minute virtual consultation.
Frequently Asked Questions
Q: What is the difference between a herniated disc and a bulging disc?
A: Both involve the intervertebral disc extending beyond its normal boundaries, but the mechanism and severity differ. A bulging disc occurs when the outer wall of the disc weakens and the entire disc bulges outward, typically without a discrete tear. The inner nucleus pulposus remains contained. A herniated disc involves a tear in the outer wall through which the inner nucleus pushes out into the spinal canal or neural foramen. Herniated discs are generally associated with more acute onset, more pronounced nerve compression, and higher likelihood of producing radicular symptoms. A bulging disc tends to develop more gradually and may be asymptomatic initially. Both conditions can cause significant pain and neurological symptoms and both can be treated effectively with Deuk Laser Disc Repair®.
Q: Can a displaced disc heal on its own without surgery?
A: Yes, in some cases. Research published in PMC in 2025 documents that lumbar disc herniations can undergo spontaneous resorption over time, with clinical symptoms improving alongside radiological evidence of resolution. Conservative management with physical therapy, anti-inflammatory medications, and activity modification is appropriate for most patients without significant neurological deficits. However, spontaneous resorption is more likely in certain herniation subtypes and in younger patients, and it does not occur reliably in all cases. Patients with progressive neurological deficits, severe or refractory pain, or loss of bladder and bowel function require surgical evaluation without delay. Waiting excessively for spontaneous resolution in the face of progressive motor weakness carries the risk of permanent nerve damage.
Q: How do I know if I need surgery for disc displacement?
A: Surgery is generally indicated when conservative care has been tried appropriately for 4 to 6 weeks without adequate improvement, when neurological deficits including muscle weakness or sensory loss are present or worsening, when pain is severe enough to prevent basic function despite optimal non-surgical management, or when cauda equina syndrome symptoms are present (which constitutes a surgical emergency). A 2025 systematic review confirmed that early surgery for patients with motor deficits achieves recovery rates above 90%, while delayed surgery results in significantly worse outcomes. If you are unsure whether surgery is necessary, an evaluation by a neurosurgeon trained in both conservative and surgical management, with review of your MRI, will provide the clearest guidance.
Q: Is Deuk Laser Disc Repair available for both neck and lower back disc displacement?
A: Yes. Deuk Laser Disc Repair is effective for disc displacement in both the cervical spine (neck) and lumbar spine (lower back), including herniated discs, bulging discs, annular tears, degenerative disc disease, and disc-related spinal stenosis at any of these levels. The procedure uses the same minimally invasive endoscopic laser approach adapted to the anatomy of the affected region. Dr. Ara Deukmedjian will review your MRI during a free consultation to determine whether DLDR is the right surgical option for your specific disc condition.
Sources
- Arthritis Research & Therapy (2015). “Osteoarthritis: a review of its pathophysiology and management strategies.” PMC4339077.
https://pmc.ncbi.nlm.nih.gov/articles/PMC4339077/ - Mayo Clinic (2024). “Osteoarthritis: Symptoms and Causes.”
https://www.mayoclinic.org/diseases-conditions/osteoarthritis/symptoms-causes/syc-20351925 - StatPearls Publishing (2024). “Osteoarthritis.” NCBI Bookshelf, NBK560878.
https://www.ncbi.nlm.nih.gov/books/NBK560878/ - Nutrients (2024). “The Role of Diet and Nutritional Supplements in Osteoarthritis Management.” PMC11425427.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11425427/ - Journal of Clinical Medicine (2025). “Association Between Osteoarthritis and Systemic Inflammation: A Clinical Review.” MDPI, 14(4):1196.
https://www.mdpi.com/2077-0383/14/4/1196 - International Journal of Molecular Sciences (2025). “Molecular Mechanisms Underlying Osteoarthritis Progression.” PMC12278955.
https://pmc.ncbi.nlm.nih.gov/articles/PMC12278955/ - Pain Physician (2024). “Efficacy of Emerging Minimally Invasive Treatments for Osteoarthritis.” PubMed PMID 40224631.
https://pubmed.ncbi.nlm.nih.gov/40224631/ - Exploratory Research in Clinical and Translational Medicine (2025). “Advances in Imaging and Diagnostics for Osteoarthritis.” ScienceDirect: S2772529425014389.
https://www.sciencedirect.com/science/article/pii/S2772529425014389 - Journal of Orthopaedic Research (2025). “Biomechanical Factors in the Development of Osteoarthritis.” PMC12242731.
https://pmc.ncbi.nlm.nih.gov/articles/PMC12242731/
Frequently Asked Questions
What is the difference between a herniated disc and a bulging disc?
Both involve the intervertebral disc extending beyond its normal boundaries, but the mechanism and severity differ. A bulging disc occurs when the outer wall of the disc weakens and the entire disc bulges outward, typically without a discrete tear. The inner nucleus pulposus remains contained. A herniated disc involves a tear in the outer wall through which the inner nucleus pushes out into the spinal canal or neural foramen. Herniated discs are generally associated with more acute onset, more pronounced nerve compression, and higher likelihood of producing radicular symptoms. A bulging disc tends to develop more gradually and may be asymptomatic initially. Both conditions can cause significant pain and neurological symptoms and both can be treated effectively with Deuk Laser Disc Repair.
Can a displaced disc heal on its own without surgery?
Yes, in some cases. Research documents that lumbar disc herniations can undergo spontaneous resorption over time, with clinical symptoms improving alongside radiological evidence of resolution. Conservative management with physical therapy, anti-inflammatory medications, and activity modification is appropriate for most patients without significant neurological deficits. However, spontaneous resorption is more likely in certain herniation subtypes and in younger patients, and it does not occur reliably in all cases. Patients with progressive neurological deficits, severe or refractory pain, or loss of bladder and bowel function require surgical evaluation without delay. Waiting excessively for spontaneous resolution in the face of progressive motor weakness carries the risk of permanent nerve damage.
How do I know if I need surgery for disc displacement?
Surgery is generally indicated when conservative care has been tried appropriately for 4 to 6 weeks without adequate improvement, when neurological deficits including muscle weakness or sensory loss are present or worsening, when pain is severe enough to prevent basic function despite optimal non-surgical management, or when cauda equina syndrome symptoms are present (which constitutes a surgical emergency). A 2025 systematic review confirmed that early surgery for patients with motor deficits achieves recovery rates above 90%, while delayed surgery results in significantly worse outcomes. If you are unsure whether surgery is necessary, an evaluation by a neurosurgeon trained in both conservative and surgical management, with review of your MRI, will provide the clearest guidance.
Is Deuk Laser Disc Repair available for both neck and lower back disc displacement?
Yes. Deuk Laser Disc Repair is effective for disc displacement in both the cervical spine (neck) and lumbar spine (lower back), including herniated discs, bulging discs, annular tears, degenerative disc disease, and disc-related spinal stenosis at any of these levels. The procedure uses the same minimally invasive endoscopic laser approach adapted to the anatomy of the affected region. Dr. Ara Deukmedjian will review your MRI during a free consultation to determine whether Deuk Laser Disc Repair is the right surgical option for your specific disc condition.


