


Medical disclaimer:This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
If you’ve been told you have a bulging disc, you’re likely feeling concerned about what this means for your future. Will you need surgery? Is this a permanent condition? Will the pain ever go away? These are natural questions, and finding clear, honest answers can feel overwhelming when you’re already dealing with back or neck discomfort.
Here’s what you need to know right away: Bulging discs are remarkably common. In fact, research shows that, depending on your age, the majority of people without any back pain whatsoever have disc bulges visible on MRI Scans. The presence of a bulge doesn’t automatically sentence you to chronic pain or surgery.
What matters most is understanding what’s actually causing your symptoms, exploring all available treatment options, and making informed decisions based on an accurate diagnosis rather than fear. This comprehensive guide will walk you through everything you need to know about bulging discs, from understanding what they are and how they develop, to conservative treatments and advanced surgical options that preserve your spine’s natural function.
Understanding Bulging Discs: What’s Really Happening in Your Spine
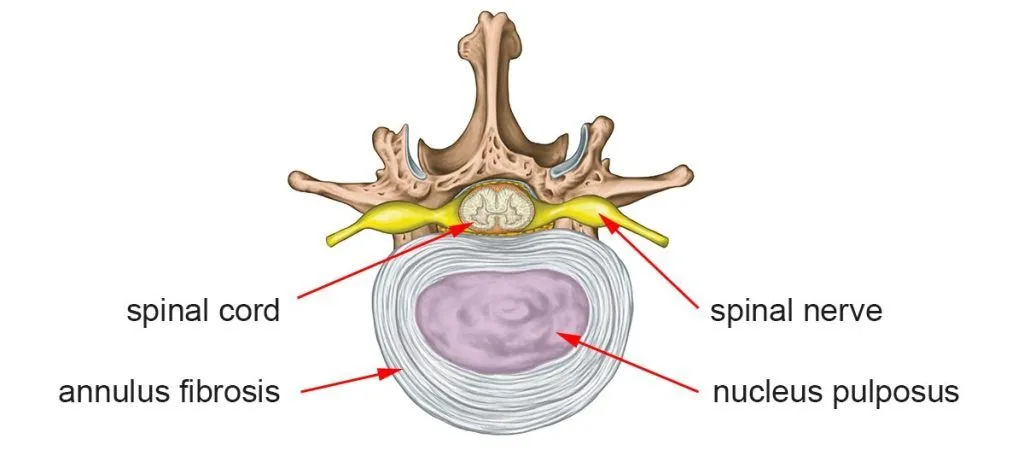
To understand bulging discs, you first need to understand disc anatomy. Your discs are complex structures designed to absorb shock, distribute forces, and allow controlled movement.
Each disc has two main components:
The nucleus pulposus: A gel-like inner core that provides cushioning and helps distribute compressive forces evenly across the disc. This gelatinous center is about 80% water in young, healthy discs.
The annulus fibrosus: A tough outer ring made of approximately 15-25 concentric layers of collagen fibers arranged in a crisscross pattern. This strong outer wall contains the nucleus pulposus and provides structural integrity to the disc.
What Exactly is a Bulging Disc?
A bulging disc occurs when the entire disc extends beyond its normal boundaries. Imagine squeezing a marshmallow between your fingers and watching it spread outward. The outer annulus fibrosus remains intact but stretches and bulges outward, typically affecting 25% or more of the disc’s circumference.
This differs from a contained protrusion, where a more focal bulge develops, or an extrusion (herniated disc), where the outer annulus develops a tear allowing the inner nucleus pulposus to leak out.
From a clinical standpoint, particularly based on our experience treating thousands of patients at Deuk Spine Institute, bulging and herniated discs lie on a continuum of disc pathology. While medical literature differentiates them technically, both arise from initial posterior annular damage that is traumatic in nature. Both can cause similar symptoms through the same mechanism: inflammation triggered by damaged disc material irritating nearby nerve structures.
How Common Are Bulging Discs?
Bulging discs are extraordinarily common, particularly in the lumbar (lower back) and cervical (neck) regions. A systematic review published in 2023 examining the natural history of lumbar disc problems found that disc abnormalities increase dramatically with age:1
- By age 30: Approximately 30% of asymptomatic individuals have disc bulges
- By age 40: About 40% show disc bulges on imaging
- By age 50: Approximately 60% have visible disc bulges
- By age 60 and beyond: 80% or more show disc degeneration and bulging
This is a crucial point that’s often misunderstood: The presence of a disc bulge on MRI does not mean you will have pain or need treatment. What matters is whether your specific bulge correlates with your symptoms.
The Critical Distinction: Bulging Disc vs. Herniated Disc
While the terms are often used interchangeably, understanding the distinction helps you comprehend your diagnosis and treatment options:
Bulging Disc (Broad-Based Protrusion):
- The outer annulus remains intact but stretches outward
- The disc extends beyond the vertebral margins in a broad, circumferential pattern (affecting 25% or more of the disc’s perimeter)
- Less likely to cause acute, severe symptoms
- May or may not compress nearby nerves
- Often discovered incidentally on imaging obtained for other reasons
Herniated Disc (Extrusion or Sequestration):
- The outer annulus develops a complete tear or rupture
- The inner nucleus pulposus leaks out through the tear into the spinal canal
- More likely to cause severe, acute symptoms
- The extruded material is highly inflammatory and chemically irritates nearby nerves
- Typically causes more dramatic symptoms requiring intervention
Despite these technical differences, from a treatment perspective and based on clinical experience, bulging discs and herniated discs are fundamentally similar. Both involve trauma to the disc that creates an annular tear. Both can cause inflammation. Both respond to similar treatments when properly diagnosed.
At Deuk Spine Institute, we’ve found that what patients call their condition matters far less than accurately identifying the source of their pain and addressing it appropriately.
If you’re confused by the different terms used to describe your disc condition, our guide on herniated disc, bulging disc, and slipped disc terminology explains all 10 names doctors and radiologists use for the same condition.
More About Bulging Discs: Key Facts to Understand
Bulging discs don’t heal on their own: Once the disc extends beyond its normal boundaries and the annulus weakens, it doesn’t spontaneously return to its original position. The structural changes are permanent, though symptoms may improve.
- Not all bulging discs cause pain: Many people live their entire lives with bulging discs that never cause symptoms. The bulge itself isn’t necessarily the problem; it’s whether the bulge causes inflammation and nerve compression that determines symptoms.
- Bulging discs can progress: Without proper care, a bulging disc can worsen over time as the disc continues to degenerate. The annulus may eventually tear, converting a bulge into a full herniation.
- Location determines symptoms: Where the bulge occurs in your spine dramatically affects what symptoms you experience. A cervical bulge causes different symptoms than a lumbar bulge.
- Treatment success depends on accurate diagnosis: The most important factor in successful treatment isn’t the severity of the bulge on imaging; it’s correctly identifying whether the bulge is truly causing your symptoms.
Bulging Discs in Different Parts of the Spine
The symptoms, complications, and treatment approaches for bulging discs vary significantly depending on where in your spine the problem occurs.

Cervical Bulging Discs (Neck Region)
The cervical spine consists of seven vertebrae (C1-C7) in your neck. Bulging discs most commonly occur at the C5-C6 and C6-C7 levels, which bear significant mechanical stress from head movements and weight.
Common symptoms of cervical bulging discs:
- Neck pain and stiffness, especially with certain movements
- Headaches originating at the base of the skull
- Shoulder pain that may radiate into the upper back
- Arm pain, numbness, or tingling (cervical radiculopathy)
- Weakness in specific muscle groups, depending on which nerve root is affected
- In severe cases, difficulty with fine motor skills, such as buttoning shirts or writing
Specific nerve root patterns:
When a cervical bulge compresses a nerve root, symptoms typically follow predictable patterns:
- C5 nerve (C4-C5 disc bulge): Pain and weakness in the shoulder and upper arm, difficulty lifting the arm away from the body
- C6 nerve (C5-C6 disc bulge): Pain radiating down the arm to the thumb, weakness in the biceps, and numbness in the thumb and index finger
- C7 nerve (C6-C7 disc bulge): Pain radiating to the middle fingers, weakness in the triceps and wrist extensors, and numbness in the middle fingers
- C8 nerve (C7-T1 disc bulge): Pain and numbness in the ring and pinky fingers, weakness in hand grip strength
Thoracic Bulging Discs (Mid-Back Region)
Thoracic disc problems are far less common than cervical or lumbar issues because the rib cage provides additional stability to this region. When thoracic bulges do occur, they’re most common at the lower thoracic levels (T8-T12).
Common symptoms of thoracic bulging discs:
- Mid-back pain that may wrap around the rib cage
- Pain that worsens with twisting or rotation
- Referred pain to the chest wall (sometimes mistaken for heart or lung problems)
- In rare severe cases, lower extremity weakness or bowel/bladder dysfunction may occur if the spinal cord is compressed
Because thoracic disc problems are uncommon and symptoms can mimic other conditions, accurate diagnosis is particularly important in this region.
Lumbar Bulging Discs (Lower Back Region)
The lumbar spine consists of five vertebrae (L1-L5) in your lower back, plus the sacral segments below. This region experiences the greatest mechanical stress during daily activities and is by far the most common site of symptomatic disc bulges.
The L3-L4, L4-L5, and L5-S1 levels are most frequently affected.2
Common symptoms of lumbar bulging discs:
- Lower back pain that may be sharp, dull, or aching
- Stiffness and limited flexibility, especially in the morning
- Pain that worsens with prolonged sitting, forward bending, or lifting
- Leg pain, numbness, or tingling (sciatica or lumbar radiculopathy)
- Weakness in specific leg muscles
- In severe cases, bowel or bladder dysfunction (a medical emergency)
Specific nerve root patterns:
Lumbar bulges cause symptoms in predictable distributions:
- L3 nerve (L2-L3 disc bulge): Pain in the front of the thigh, weakness in knee extension
- L4 nerve (L3-L4 disc bulge): Pain down the front and inner thigh, weakness in straightening the knee, and numbness along the inner shin
- L5 nerve (L4-L5 disc bulge): Pain down the outer leg to the top of the foot, weakness lifting the foot upward (foot drop), and numbness between the first and second toes
- S1 nerve (L5-S1 disc bulge): Pain down the back of the leg to the foot, weakness pushing up on tiptoes, and numbness on the bottom of the foot and outer toes
For more detailed information about sciatica and its various causes, see our comprehensive guide “Pain Radiating Below the Knee: When Sciatica Demands Your Attention.”3
Why Bulging Discs Don’t Always Cause Pain: The Inflammation Connection
One of the most important concepts in understanding disc-related pain is this: compression alone doesn’t cause most back pain; inflammation does.
For decades, the medical community believed that disc bulges caused pain primarily through mechanical compression of nerve roots. While nerve compression can certainly cause symptoms, recent research has fundamentally changed our understanding of disc pain.

The Chemical Inflammation Process
When a disc degenerates, develops an annular tear, or bulges significantly, inflammatory chemicals are released into the surrounding tissues. These chemical mediators include:4
- Prostaglandins: Lipid compounds that promote inflammation and pain
- Cytokines: Particularly TNF-alpha (tumor necrosis factor-alpha) and IL-6 (interleukin-6), which trigger inflammatory cascades
- Proteolytic enzymes: Molecules that break down the extracellular matrix and contribute to tissue damage
- Substance P: A neuropeptide involved in pain transmission
These inflammatory substances sensitize nerve endings, causing pain even without significant mechanical compression. This explains the paradox we see clinically: some people with large disc bulges have minimal symptoms, while others with relatively small bulges experience debilitating pain (the level of inflammation varies considerably between individuals).
A 2025 systematic review examining conservative treatments for lumbar disc herniation confirmed that addressing inflammation, rather than just mechanical decompression, is crucial for successful treatment outcomes.5
Clinical Implications of Understanding Inflammation
This understanding has profound implications for treatment:
- Conservative approaches that target inflammation: Anti-inflammatory medications, epidural steroid injections, and physical therapy that reduces inflammatory stress on the disc can all provide relief.
- Surgical removal of inflammatory tissue: Procedures that precisely remove the damaged, inflammatory disc material (like Deuk Laser Disc Repair®) address the root cause of pain without removing entire discs or fusing vertebrae.
- Compression relief alone may not be enough: Traditional surgeries that simply decompress nerves without addressing inflammatory disc material may provide incomplete relief.
- Natural healing: The body’s immune system can sometimes gradually remove inflammatory disc material through a process called spontaneous resorption, which explains why many patients improve with time and conservative care.
Common Causes and Risk Factors for Bulging Discs
Understanding what causes disc bulges can help you make informed decisions about prevention and treatment. While some risk factors are beyond your control, others can be modified to reduce your risk.
Age-Related Degeneration
The most common cause of bulging discs is degenerative disc disease. These are natural changes that occur as we age:
Water content decreases: Healthy discs are about 80% water in youth. As we age, discs lose hydration, becoming less flexible and more prone to injury. By middle age, discs may be only 70% water.
- Height loss: Dehydrated discs lose height, altering spinal mechanics and increasing stress on facet joints and other structures.
- Weakened annulus: The outer ring becomes less resilient with age as collagen fibers deteriorate, making the disc more susceptible to bulging and tearing.
- Reduced nutrient supply: Adult discs have a limited blood supply and rely on diffusion for nutrition. This process becomes less efficient with age, impairing the disc’s ability to repair minor damage.
Mechanical Stress and Trauma
Certain activities and events place excessive stress on spinal discs:
- Heavy lifting: Improper lifting technique, especially with twisting motions, creates enormous pressure on discs. Lifting a 50-pound object with poor form can place 500+ pounds of pressure on lumbar discs.
- Repetitive bending: Occupations requiring frequent forward bending accelerate disc wear. Studies show that occupations involving repetitive lifting and bending are associated with significantly higher rates of disc problems.6
- Prolonged sitting: Sitting increases intradiscal pressure by up to 40% compared to standing. Modern sedentary lifestyles place tremendous chronic stress on lumbar discs.
- Acute trauma: Car accidents, falls, sports injuries, or any sudden impact can cause immediate disc damage that may not become symptomatic for weeks or months.
- Vibration exposure: Long-distance truck drivers and heavy equipment operators face a higher risk due to whole-body vibration, which can accelerate disc degeneration.
Lifestyle and Genetic Factors
Several modifiable and non-modifiable factors influence disc health:
- Obesity: Excess body weight increases mechanical load on spinal discs, particularly in the lumbar region. Research consistently shows higher rates of disc problems in individuals with elevated BMI.
- Smoking: Nicotine constricts blood vessels, impairing the already limited blood flow to discs. This reduces nutrient delivery and waste removal, accelerating degeneration. Studies show smokers experience more severe disc degeneration and poorer treatment outcomes.
- Physical inactivity: Weak core muscles fail to adequately support the spine, placing greater stress on passive structures such as discs. Regular movement is also essential for disc nutrition through diffusion.
- Genetics: A family history of disc problems can increase an individual’s susceptibility to disc problems. Some people inherit a tendency toward earlier disc degeneration or weaker disc tissue.
- Poor posture: Chronic postural imbalances create uneven disc loading. Forward head posture and slouched sitting positions place sustained stress on cervical and lumbar discs.
- Occupation: Physically demanding jobs involving heavy lifting, frequent bending, or prolonged static postures can significantly increase risk.
Diagnosis: The Foundation of Successful Treatment
Accurate diagnosis is absolutely essential for successful treatment, yet many patients struggle through months or years of unsuccessful treatments because their condition wasn’t properly assessed initially.

The Critical Importance of Physical Examination
While imaging studies like MRI are invaluable, they cannot diagnose the source of your pain on their own. As I frequently tell patients: “MRI scans don’t tell you where pain comes from; patients do.”
A comprehensive physical examination should include:
- Medical history: Detailed discussion of when symptoms started, what makes them better or worse, how they’ve progressed, and what treatments you’ve tried.
- Range of motion testing: Assessment of how your spine moves in different directions and which movements reproduce your symptoms.
- Neurological examination: Testing of strength, sensation, and reflexes in your arms or legs to identify nerve involvement.
- Provocative tests: Specific maneuvers designed to reproduce your symptoms and identify their source. For lumbar issues, this includes the straight leg raise test. Spurling’s test is often used for cervical problems.
- Palpation: Careful examination of your spine to identify areas of tenderness, muscle spasm, or structural abnormalities.
The physical examination findings must correlate with imaging studies for accurate diagnosis. A disc bulge seen on MRI that doesn’t correspond to your symptoms may be an incidental finding unrelated to your pain.
Imaging Studies: What They Show and What They Don’t
Magnetic Resonance Imaging (MRI):
MRI is the gold standard for visualizing bulging discs and their effects on surrounding structures.7 It provides detailed images showing:
- The exact location, size, and type of disc abnormalities
- Whether nerve roots are being compressed
- The degree of disc degeneration
- The presence of other conditions, like spinal stenosis or facet joint arthritis
- Inflammatory changes in the surrounding tissues
However, MRI findings must be interpreted in the clinical context. Studies consistently show that many people without pain have disc bulges on MRI. The bulge you see on imaging may or may not be causing your symptoms.
X-Rays:
While X-rays cannot visualize discs directly (they only show bones), they can provide valuable information:
- Vertebral alignment and curvature
- Disc space height (indirect measure of disc health)
- Bone spurs that might contribute to nerve compression
- Signs of instability with flexion-extension views
CT Scans:
Computed tomography offers excellent bony detail and may be useful when:
- MRI is contraindicated (patients with certain metal implants or pacemakers)
- Evaluating bone spurs or foraminal narrowing caused by bony overgrowth
- Surgical planning requires precise visualization of bony anatomy
Electrodiagnostic Studies (EMG/NCS):
These tests measure electrical activity in muscles and nerves:
- Confirm the presence and severity of nerve root compression
- Identify which specific nerve root is affected
- Distinguish lumbar radiculopathy from peripheral nerve problems
- Assess whether nerve damage is acute or chronic
The Value of Getting a Second Opinion
Given the complexity of diagnosing disc-related pain and the significant variation in treatment recommendations among spine specialists, seeking a second opinion is often one of the smartest decisions you can make.
This is especially true if:
- You’ve been recommended for surgery, but have questions about whether it’s necessary
- Conservative treatments haven’t provided relief, and you’re unsure about next steps
- Your diagnosis seems unclear or doesn’t match your symptoms
- You want to explore all treatment options, including advanced minimally invasive approaches
- The recommended surgery involves fusion or other procedures that permanently alter your spine
What a second opinion provides:
- Confirmation that your diagnosis is correct and complete
- Alternative perspective on treatment options you may not have known existed
- Identification of overlooked factors contributing to your pain
- Peace of mind that you’re making an informed decision
Important consideration: The challenge with spine surgery is that most surgeons recommend what they know how to do, rather than necessarily what’s best for you. A surgeon who primarily performs fusion will likely recommend fusion. A pain management specialist who doesn’t perform surgery will recommend injections. An endoscopic spine surgeon will evaluate whether you’re a candidate for minimally invasive approaches.
This isn’t a matter of dishonesty; it’s human nature. We tend to see problems through the lens of our training and experience. This is why seeking opinions from specialists with different skillsets helps you make truly informed decisions.
Upload your MRI for a free second opinion: At Deuk Spine Institute, we offer a free virtual consultation and MRI review. This service has helped countless patients discover treatment options they didn’t know existed. Upload your latest MRI.

Conservative Treatment: What Your Doctor Will Likely Prescribe First
For most patients with bulging discs, an initial trial of conservative treatment is appropriate and often successful. Research indicates that patients with disc problems can improve with comprehensive conservative care.8
The keyword here is “comprehensive.” Not all conservative treatments are equally effective, and the quality of implementation matters significantly.
Medications for Pain and Inflammation Management
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs):
Medications like ibuprofen, naproxen, or celecoxib help reduce inflammation and pain. They work best when used regularly during flare-ups rather than only when pain is severe.
Important considerations: Long-term use carries risks, including gastrointestinal bleeding, kidney problems, and cardiovascular concerns. Always use the lowest effective dose for the shortest duration necessary.
Acetaminophen:
This pain reliever can be helpful for mild to moderate pain, particularly when combined with other treatments. It doesn’t reduce inflammation, but it can improve pain tolerance and help you participate more effectively in physical therapy.
Muscle Relaxants:
Medications such as cyclobenzaprine or methocarbamol can help reduce muscle spasms that often accompany disc problems, improving mobility and comfort. These typically cause drowsiness and are used short-term.
Neuropathic Pain Medications:
For nerve-related pain (radiculopathy), medications like gabapentin or pregabalin specifically target nerve pain pathways. These can be particularly helpful for burning, shooting, or electric-shock sensations.
Oral Corticosteroids:
A short course of oral steroids may be prescribed for severe acute inflammation to rapidly reduce swelling and pain.
Important note: While opioid medications may provide short-term relief for acute pain, they are not recommended for long-term management of chronic disc pain due to risks of dependence, tolerance, and limited long-term effectiveness.
Physical Therapy and Exercise
A well-designed physical therapy program is one of the most effective conservative treatments for bulging discs. A 2025 meta-analysis published in Frontiers in Medicine found that exercise therapy can significantly improve pain, disability, range of motion, and quality of life in patients with lumbar disc problems.9
An evidence-based program might include:
Core Strengthening:
Building strength in abdominal and back muscles provides better support for the spine, reducing stress on discs. However, it’s crucial to perform exercises correctly as improper core work can worsen disc problems.
Recommended exercises include planks, bird-dogs, dead bugs, and bridges, all performed with proper form and appropriate progression.
Flexibility Training:
Gentle stretching of tight muscles, particularly hip flexors, hamstrings, and lumbar paraspinals, can improve movement patterns and reduce strain on the lower back.
Nerve Gliding Exercises:
Specific movements that help nerves move more freely through surrounding tissues, potentially reducing radicular symptoms.
Postural Training:
Learning proper body mechanics for daily activities helps minimize disc stress. This includes proper lifting technique, sitting posture, standing posture, and sleeping positions.
Manual Therapy:
Hands-on techniques by a physical therapist can help improve joint mobility and reduce muscle tension.
The effectiveness of physical therapy depends heavily on the quality of the program and patient compliance. Working with a therapist who specializes in spinal conditions and has experience treating disc problems is essential.
Activity Modification and Lifestyle Changes
Avoid aggravating activities:
- Limit heavy lifting, repetitive bending, and prolonged sitting while your disc heals
- This doesn’t mean complete rest; remaining moderately active is important for healing and maintaining function
Maintain a healthy weight:
For overweight individuals, losing even 5-10% of body weight can significantly reduce the mechanical load on spinal discs and improve symptoms.
Smoking cessation:
Quitting smoking improves blood flow to discs, enhancing healing capacity and slowing degeneration. This is one of the most impactful lifestyle changes you can make for spine health.
Ergonomic modifications:
- Adjust workstations to promote proper posture
- Use lumbar support when sitting
- Ensure proper mattress support for sleeping
- Take frequent breaks from static positions
Stay active with appropriate exercises:
Low-impact activities like walking, swimming, or cycling help maintain disc nutrition through diffusion and overall spinal health. Research shows that regular moderate activity is protective against disc degeneration.
Injection-Based Therapies
When oral medications and physical therapy provide insufficient relief, several injection options may be considered:
Epidural Steroid Injections (ESIs):
These involve injecting corticosteroid medication and local anesthetic into the epidural space around inflamed nerve roots. ESIs can reduce inflammation and provide pain relief lasting weeks to months in some patients.
Limitations:
- Relief is often temporary (3-6 months on average)
- Repeated injections may weaken bone and soft tissues
- They don’t address the underlying disc problem
- Not all patients respond favorably
Selective Nerve Root Blocks:
These more targeted injections deliver medication directly around specific nerve roots, serving both diagnostic and therapeutic purposes.
When Conservative Treatment Isn’t Enough: Recognizing the Signs
While conservative treatment succeeds for most patients, recognizing when it’s not working is crucial for preventing permanent damage and unnecessary prolonged disability.
Clear Indications That It’s Time to Consider Surgery
Progressive motor weakness:
If you’re experiencing increasing weakness in your leg or foot despite conservative treatment, nerve damage may be progressing. Prolonged compression can lead to permanent muscle atrophy and functional loss that won’t fully recover even after successful decompression.
Specific warning signs include:
- Foot drop (difficulty lifting your foot)
- Weakness in climbing stairs
- Difficulty rising from a seated position
- Progressive loss of grip strength (for cervical problems)
Severe, intractable pain:
Pain that prevents sleep, interferes with work, or limits basic daily activities represents more than an inconvenience. This is a legitimate indication for definitive treatment when conservative approaches have been exhausted.
Failed conservative treatment:
If you’ve undergone 6-12 weeks of comprehensive conservative care (not just one or two approaches, but a genuine multidisciplinary program) without meaningful improvement, continuing the same ineffective treatments indefinitely makes little sense.
Cauda equina syndrome (MEDICAL EMERGENCY):
This rare but serious condition occurs when a massive disc problem compresses multiple nerve roots, causing:
- Bowel or bladder dysfunction
- Saddle anesthesia (numbness in the area that would contact a saddle)
- Bilateral leg weakness
- Sexual dysfunction
This condition requires urgent surgical decompression to prevent permanent neurological damage.
The Minimally Invasive Approach: Starting With the Least Damage
When surgery becomes necessary, starting with the least invasive, most tissue-preserving approach makes logical sense. This philosophy aligns with the medical principle of “primum non nocere,” which translates to: First, do no harm.
Why minimally invasive surgery makes sense as a first surgical option:
- Preserves future options: If a minimally invasive procedure doesn’t provide complete relief, you can still undergo more aggressive surgery later. However, if you start with fusion or other destructive procedures, you can limit the option of less invasive treatments permanently.
- Faster recovery: Minimally invasive procedures typically allow you to return to activities in weeks rather than months, minimizing disruption to your life.
- Lower complication rates: Less tissue trauma means lower risk of infection, bleeding, and other surgical complications.
- Preserves spinal motion and stability: Motion-preserving procedures maintain your spine’s natural biomechanics, avoiding the long-term consequences of fusion.
- Addresses the actual problem: Precision removal of only the damaged, inflammatory disc material treats the root cause while leaving healthy structures intact.
Real Patient Story: From Daily Struggle to Total Relief
John had lived with constant lower back pain for years. “My pain was relentless, holding me back from walking the beach, climbing stairs, or even enjoying retirement,” he remembers. Most days, his discomfort sat between a 7 and 8 on the pain scale, making simple activities feel impossible.
After trying conservative care without lasting results, John chose the minimally invasive Deuk Laser Disc Repair to treat his herniated L3-4 and L4-5 discs. With just tiny incisions and no fusion hardware, the procedure targeted the source of his disc pain directly.
The change was immediate. “Just one day after surgery, I could climb stairs without holding on, the pain was gone, and I didn’t even need pain medication,” John says. Within a day, he was moving freely again and quickly returned to many activities he once loved.
John’s experience highlights key points about this treatment:
- Long-term relief: Patients who choose this procedure can achieve dramatic outcomes even without relying on traditional pain management.
- Multiple levels of back issues can be resolved: John’s two affected discs were both treated with one minimally invasive approach.
- Recovery can be fast: Patients often notice relief and improved function within a day of surgery.
- Chronic pain doesn’t have to define your later years: Even long-standing pain can be resolved with the right treatment.
Watch his story, here.

Precautions to Prevent Worsening Your Condition
While pursuing treatment for your bulging disc, certain activities and movements should be avoided to prevent worsening your condition or causing additional damage.
Activities That Can Aggravate Bulging Discs
Heavy Lifting:
Why it’s problematic: Lifting places enormous compressive forces on your spinal discs. The actual load on your spine is far greater than the weight you’re lifting due to mechanical disadvantages. For example, lifting a 50-pound object can place 500+ pounds of pressure on lumbar discs.
What to avoid:
- Any lifting over 10-15 pounds during acute pain phases
- Lifting while twisting or bending
- Lifting objects far from your body
- Repetitive lifting throughout the day
What to do instead:
- Use proper lifting technique (bend knees, not waist)
- Keep objects close to your body
- Ask for help with heavy items
- Use assistive devices (dollies, carts) when possible
Gym Activities and Exercise Modifications
Deadlifts:
Why they’re problematic: Deadlifts place maximum compressive and shear forces on lumbar discs, particularly at L4-L5 and L5-S1. The forward-bent starting position increases intradiscal pressure dramatically.
Recommendation: Avoid conventional deadlifts entirely during acute phases. Even after recovery, consider safer alternatives, such as trap bar deadlifts or Romanian deadlifts with very light weights and perfect form.
Squats:
Why they’re problematic: Heavy back squats compress the spine significantly. Poor form (i.e., forward lean, excessive depth, or rounding of the lower back) dramatically increases disc stress.
Recommendation: During acute phases, avoid squats entirely. After recovery, use light weights with excellent form, maintain neutral spine position, and avoid excessive depth. Consider alternatives like leg press or split squats that place less spinal load.
Romanian Deadlifts (RDLs):
Why they’re problematic: RDLs involve maintaining a hinged position that places sustained load on the posterior disc, exactly where most bulges occur.
Recommendation: Avoid during the acute and recovery phases. If performed after full recovery, use very light weights and impeccable form.
Weighted Machines (Leg Press, Seated Row, Lat Pulldown):
Why some are problematic: Seated exercises that round the spine (especially seated rows with poor form) can aggravate disc problems. Leg press with excessive weight or poor foot position can also stress the lumbar spine.
Recommendation:
- Leg press: Keep lower back pressed firmly against the pad, avoid excessive weight
- Seated row: Maintain neutral spine, avoid rounding forward
- Lat pulldown: Generally safe with proper form
- Avoid machines that require twisting or excessive forward flexion
Running:
Why it’s problematic: Running creates repetitive impact forces that compress spinal discs with each foot strike. The jarring can aggravate already-inflamed disc tissue and nerve roots.
Recommendation: During acute phases, avoid running completely. After symptoms improve, start with walking, progress to elliptical training (lower-impact), and gradually return to running if tolerated. Consider running on softer surfaces (trails, tracks) rather than concrete.
Core Work (Sit-ups, Crunches, Leg Raises):
Why certain exercises are problematic: Traditional sit-ups and crunches involve repeated forward flexion, the exact movement that increases pressure on posterior disc bulges. Leg raises can create enormous strain on the lumbar spine if performed with poor form.
Recommendation: Avoid traditional sit-ups and crunches. Instead, perform planks, bird-dogs, dead bugs, and pallof presses that strengthen the core through stabilization rather than flexion.
Contact Sports and High-Impact Activities
Football, Hockey, Rugby:
These sports involve high-velocity collisions, twisting, and unpredictable impacts, all of which can severely aggravate or worsen a bulging disc. Avoid during acute phases and approach cautiously even after recovery.
Martial Arts:
Grappling sports (jujitsu, wrestling) involve extreme spinal positions and sudden forces. Striking sports risk impact trauma. Consider low-impact alternatives until fully recovered.
Basketball, Volleyball:
Jumping and landing create compressive forces. Sudden directional changes involve twisting. These activities should be avoided during acute phases and approached gradually during recovery.
Golf: The Perfect Storm of Problematic Movements
Golf is particularly challenging for people with disc problems due to the biomechanics of the golf swing:
Why golf aggravates disc problems:
- Rotational torque: The golf swing involves powerful rotation of the thoracic and lumbar spine, creating enormous rotational stress on discs.
- Asymmetric loading: The same-side dominance (always swinging from one side) creates repetitive asymmetric stress patterns.
- Forward flexion: Addressing the ball requires bending forward, increasing disc pressure before you even swing.
- Explosive force: Driving the ball involves generating maximum power through your spine in a fraction of a second.
- Repetition: A typical round involves 70-100 full swings plus numerous practice swings.
Professional golfers like Tiger Woods have experienced severe disc problems requiring multiple surgeries, illustrating how demanding this sport is on the spine.
Recommendations for golfers:
During acute phases, avoid golf completely. During recovery, practice putting only (minimal spinal stress). When returning to full golf:
- Warm up thoroughly before playing
- Focus on smooth, controlled swings rather than maximum distance
- Use proper mechanics with less torso rotation
- Take frequent breaks
- Consider professional instruction to improve mechanics
- Stop immediately if pain develops
Understanding the Biomechanics: Why These Activities Cause Problems
These activities share common biomechanical features that stress-injured discs:
- Compressive loading: Forces that squeeze the disc vertically, increasing internal disc pressure
- Flexion (forward bending): Increases pressure on the posterior annulus, where most bulges occur
- Rotation (twisting): Creates shear forces that stress the annular fibers in different directions
- Lateral bending: Increases pressure on one side of the disc asymmetrically
- Repetition: Even modest forces become problematic when repeated hundreds or thousands of times
- Sudden, explosive movements: Don’t allow gradual force distribution or protective muscle activation
Understanding these principles helps you evaluate which activities are safe and which should be avoided or modified.
Surgical Treatment Options: From Traditional to Revolutionary
When conservative treatment hasn’t provided adequate relief and surgery becomes necessary, understanding all your options is essential. Not all surgical procedures are equal; they vary dramatically in invasiveness, recovery time, long-term outcomes, and impact on spinal function.
Traditional Surgical Approaches
Microdiscectomy:
This has been the standard surgical treatment for disc problems for decades. The procedure involves:
- Accessing the spine from the back through a 1-2 inch incision
- Removing a portion of the lamina (laminotomy) to access the disc
- Removing the bulging or herniated portion pressing on the nerve root
Recovery typically requires several days in the hospital, 4-6 weeks for return to light activities, and 3-6 months for full recovery.
While microdiscectomy can be effective, it involves removing bone to access the disc, which can weaken spinal stability and potentially lead to future complications.
Laminectomy:
This procedure involves removing a larger portion of the lamina to decompress the spinal canal. It’s typically reserved for cases with significant spinal stenosis in addition to disc bulging.
Recovery is generally longer and more challenging than with microdiscectomy, and removing substantial bone can compromise spinal stability.
Spinal Fusion:
When disc problems are accompanied by spinal instability or involve multiple levels, some surgeons recommend fusion. This procedure permanently joins two or more vertebrae together using bone grafts and hardware (screws and rods).
However, fusion has significant drawbacks:
- Eliminates motion at the fused segment
- Alters spinal biomechanics permanently
- Increases stress on adjacent levels (potentially accelerating their degeneration)
- Requires extensive recovery time of 6-12 months
- Higher complication rates than motion-preserving procedures
Research consistently shows that fusion carries an increased risk of adjacent segment disease, where levels above or below the fusion develop problems requiring additional surgery.10
Deuk Laser Disc Repair®: A Revolutionary Motion-Preserving Alternative
After witnessing the limitations and complications of traditional spine surgery throughout my training and career, I became convinced that a better approach was needed. This led to the development of Deuk Laser Disc Repair® (DLDR), a minimally invasive, motion-preserving procedure that addresses the pathological disc material while leaving healthy structures intact.
A Different Philosophy of Treatment:
Traditional lumbar spine surgery operates on premises that made sense decades ago but have proven problematic:
- Removing bone to access the disc
- Often removing large portions of the disc
- Sometimes, fusing vertebrae when instability is present
This approach has several fundamental flaws:
- Treats surrounding healthy tissue as collateral damage
- Permanently alters spinal biomechanics when fusion is performed
- Requires significant tissue dissection, leading to prolonged recovery
- Carries a substantial risk of complications
DLDR® takes an entirely different approach:
- Precisely removes only the damaged portion of the disc causing symptoms
- Leaves the healthy disc intact to preserve function
- Maintains natural spinal motion without fusion or hardware
- Minimizes tissue trauma through advanced endoscopic techniques
How Deuk Laser Disc Repair® Works:
DLDR® is performed through a tiny 4-7mm incision, so small it can be covered with a simple band-aid. Through this minimally invasive opening:
- A specialized endoscope provides high-definition visualization
- Advanced laser technology targets only the damaged disc material
- Typically, just 5-10% of the total disc is removed, only the inflammatory portion
- The laser’s precision allows work around delicate neural structures
- The natural disc continues to provide cushioning and allow normal motion
The procedure typically takes approximately one hour to perform and is done on an outpatient basis. This means that patients go home on the very same day.
The Science Behind Precision:
The key to DLDR®’s success lies in its precision. Because tissues aren’t unnecessarily traumatized, patients typically:
- Experience minimal postoperative pain
- Walk out of recovery within an hour
- Return to work within days rather than months
- Maintain full spinal motion permanently
Recovery Timeline and Outcomes:
One of the most dramatic differences between DLDR® and traditional surgery is the recovery experience:
- Day of surgery: Most patients notice significant pain relief as soon as they wake from twilight anesthesia. They leave the recovery room within an hour and go home the same day.
- First week: The tiny incision heals within days. Most patients require only over-the-counter pain medication, if anything. Many return to desk work within 3-5 days.
- 2-4 weeks: Complete healing occurs. Patients can resume most normal activities with minor restrictions.
- Long-term: Because no fusion was performed, no adjacent segment disease develops. Patients maintain a full range of motion and can expect normal function for decades.
Proven Outcomes:
DLDR® isn’t experimental; it’s an established, proven procedure with:
- 99.6% patient reported success rate in eliminating disc-related pain
- Zero complications in over 2,700 patients treated
- Over 15 years of clinical experience
- Published in peer-reviewed medical literature
- Covered by most major insurance plans
Benefits Beyond Pain Relief:
The advantages of DLDR® extend far beyond simply relieving symptoms:
- Preservation of natural anatomy: Normal biomechanics remain intact
- No hardware complications: No metal screws, plates, or rods
- Minimal scarring: The 4-7mm incision heals with virtually no visible scar
- No narcotics needed: The procedure is so precise that postoperative narcotic pain medication is typically unnecessary
- Preserves future options: Unlike fusion, DLDR® doesn’t eliminate other treatment options if needed in the future
Deuk Plasma Rhizotomy®: For Facet-Related Pain
In some cases, bulging discs occur alongside facet joint arthritis. When facet joints are a significant pain generator, Deuk Plasma Rhizotomy® offers a revolutionary solution.
This procedure eliminates joint pain naturally by permanently disconnecting pain nerves to the affected joint through a 4mm incision. The proprietary technology and patented technique pioneered at Deuk Spine Institute allows patients to enjoy long-term pain-free movement.
Key advantages:
- 10-minute outpatient procedure
- 4mm incision
- Permanent pain relief
- Fast recovery
- No hardware or implants
For patients with combined disc and facet problems, both procedures can be performed together for comprehensive relief.
Key Takeaways: What You Need to Remember
If you’re dealing with a bulging disc, here are the most important points to remember:
Bulging discs are extremely common: Up to 80% of people over 60 have disc bulges visible on MRI, yet many experience no pain. The presence of a bulge doesn’t automatically mean you need treatment; what matters is whether it’s causing symptoms.
Bulging discs and herniated discs are similar: While technically different, both arise from annular tears and disc trauma. Both cause inflammation and can produce similar symptoms. From a treatment perspective, they’re managed similarly.
Location matters tremendously: Cervical, thoracic, and lumbar bulges cause distinct symptoms and require location-specific treatment.
Inflammation drives pain, not just compression: Understanding that chemical inflammation is often more important than mechanical pressure helps explain why anti-inflammatory treatments are so effective.
Physical examination is as important as MRI: Imaging findings must correlate with clinical symptoms. An MRI alone cannot diagnose the source of your pain.
Second opinions are invaluable: Different specialists offer different perspectives and treatment options. Seeking expert second opinions ensures you understand all available options before making life-changing decisions.
Most cases improve with conservative care: Many patients improve with comprehensive conservative treatment, including physical therapy, medications, activity modification, and time.
Certain activities make bulging discs worse: Heavy lifting, high-impact exercise, contact sports, golf, and gym exercises like deadlifts and squats can aggravate disc problems and should be avoided or modified during acute phases.
Not all surgeries are equal: Traditional approaches involving fusion permanently alter your spine. Modern minimally invasive procedures like Deuk Laser Disc Repair preserve natural motion while achieving superior outcomes with dramatically faster recovery.
Recovery is possible: Whether through conservative treatment or advanced minimally invasive surgery, the vast majority of patients with bulging discs can achieve significant pain relief and return to active, fulfilling lives.
Don’t delay necessary treatment: While avoiding surgery when possible is reasonable, unnecessarily delaying surgery when genuinely needed can result in permanent nerve damage, chronic pain sensitization, and prolonged disability.
Frequently Asked Questions
-
What’s the difference between a bulging disc and a herniated disc?
While medical literature differentiates these conditions technically, they’re fundamentally similar from a clinical and treatment perspective.
- Bulging disc: The entire disc extends beyond its normal boundaries in a broad, circumferential pattern. The outer annulus fibrosus remains intact but stretched.
- Herniated disc: The outer annulus develops a complete tear, allowing the inner nucleus pulposus to leak out into the spinal canal.
Both conditions arise from disc trauma, creating an annular tear. Both can cause inflammation and nerve compression. Both respond to similar treatments when properly diagnosed.
At Deuk Spine Institute, based on treating thousands of patients, we’ve found that what you call the condition matters far less than accurately identifying whether it’s causing your symptoms and addressing it appropriately. Both bulging and herniated discs can be successfully treated with motion-preserving minimally invasive procedures that address the inflammatory disc material without permanently altering your spine.
-
Can a bulging disc heal on its own without surgery?
The structural changes of a bulging disc are permanent—once the disc extends beyond its normal boundaries, it doesn’t spontaneously return to its original position. However, symptoms can improve significantly without surgical intervention for most patients.
Research indicates that patients can experience substantial improvement with appropriate conservative treatment.8
The natural healing process involves several mechanisms:
- Acute inflammation subsides over time.
- The immune system can gradually resorb some herniated disc material
- The nervous system adapts to chronic compression
- Strengthening surrounding muscles provides better spinal support
However, “healing” doesn’t mean the disc returns to its pre-injury state. Once the annulus develops tears, permanent structural changes typically persist. While symptoms may resolve, underlying disc degeneration remains.
Key factors influencing success with conservative treatment:
- Size and type of disc pathology
- Degree of nerve compression
- Your age and overall health
- Adherence to treatment recommendations
- Whether progressive weakness develops
If symptoms persist beyond 6-12 weeks of comprehensive conservative treatment, or if progressive weakness develops, surgical evaluation is warranted.
-
How do I know if my bulging disc needs surgery?
Surgery should be considered when:
- Conservative treatment has failed: You’ve undergone 6-12 weeks of comprehensive conservative care (physical therapy, appropriate medications, injections, activity modifications) without meaningful improvement.
- Progressive motor weakness: You’re experiencing increasing weakness in specific muscle groups (foot drop, hand weakness, difficulty climbing stairs) despite treatment. Prolonged nerve compression can cause permanent muscle atrophy.
- Severe pain impacting quality of life: Pain prevents sleep, interferes with work, or limits basic daily activities despite appropriate conservative treatment.
- Cauda equina syndrome: This medical emergency involves bowel or bladder dysfunction, saddle anesthesia, and bilateral leg weakness, which requires immediate surgical decompression.
- Neurological symptoms worsening: Numbness, tingling, or weakness that’s progressively worsening rather than improving.
However, even when surgery becomes necessary, you have options. Traditional procedures, such as fusion, permanently alter your spine. Modern minimally invasive techniques like Deuk Laser Disc Repair® address the problem while preserving natural motion and biomechanics.
Getting a second opinion from a specialist experienced in motion-preserving techniques ensures you understand all your options before committing to surgery.
-
What activities should I avoid with a bulging disc?
Certain activities can significantly aggravate bulging discs and should be avoided or modified:
-
Definitely avoid:
- Heavy lifting (anything over 10-15 pounds during acute phases)
- Deadlifts, squats, and Romanian deadlifts in the gym
- High-impact running or jumping activities
- Contact sports (football, hockey, rugby, martial arts)
- Golf (combines rotation, flexion, and explosive force)
- Exercises involving repeated forward bending (sit-ups, toe touches)
- Activities requiring twisting while loaded
- Prolonged sitting without breaks
-
Modify carefully:
- Weight machines: Use light weights, maintain perfect form, and avoid exercises requiring spinal flexion or rotation
- Yoga: Avoid poses requiring deep forward bending or twisting
- Cycling: Maintain upright posture, avoid racing position
- Swimming: Generally safe, but avoid aggressive butterfly stroke
-
Generally safe:
- Walking (excellent low-impact exercise)
- Gentle stretching within a pain-free range
- Water aerobics
- Stationary bike with upright posture
- Light resistance training with proper form
- Core stabilization exercises (planks, bird-dogs, dead bugs)
The key is understanding biomechanics: avoid activities that involve heavy compression, forward flexion, rotation, or explosive movements. Listen to your body. If an activity increases pain, stop immediately.
As symptoms improve, you can gradually return to activities, but this should be done progressively under the guidance of a physical therapist or physician who understands your specific condition.
-
How long does recovery take after bulging disc surgery?
Recovery time varies dramatically depending on which surgical procedure is performed:
-
Traditional Microdiscectomy:
- Hospital stay: 1-2 days
- Return to light activities: 4-6 weeks
- Full recovery: 3-6 months
- Physical therapy is typically needed for several months
- Some permanent activity restrictions may apply
-
Spinal Fusion:
- Hospital stay: 2-4 days
- Bone fusion takes 3-6 months to solidify
- Return to work: 3-6 months
- Full recovery: up to one year
- Permanent loss of motion at fused segment
- Risk of adjacent segment disease requiring future surgery
-
Deuk Laser Disc Repair® (Minimally Invasive):
- Same-day outpatient procedure with no hospital stay
- Most patients experience immediate relief from leg pain
- Return to desk work: 3-5 days
- Complete healing: 2-3 weeks
- No prolonged activity restrictions
- Full range of motion is preserved permanently
- No risk of adjacent segment disease
The dramatic difference stems from the fundamental approach. Traditional surgeries involve significant tissue trauma and often permanent alteration of spinal anatomy. Minimally invasive endoscopic approaches preserve healthy tissue and maintain normal biomechanics, resulting in dramatically faster recovery and superior long-term outcomes.
For patients who qualify, starting with the least invasive, most tissue-preserving approach makes logical sense. If a minimally invasive procedure doesn’t provide complete relief, more aggressive options remain available. However, if you start with fusion, you may be limiting future options.
-
Sources
1: https://pmc.ncbi.nlm.nih.gov/articles/PMC4464797
2: https://deukspine.com/blog/l3-l4-l5-disc-bulge-treatment
3: https://deukspine.com/blog/what-is-causing-my-sciatica
4: https://pmc.ncbi.nlm.nih.gov/articles/PMC4151534/
5: https://pmc.ncbi.nlm.nih.gov/articles/PMC11985520/
6: https://www.frontiersin.org/journals/neurology/articles/10.3389/fneur.2025.1706784/full
7: https://deukspine.com/blog/herniated-disc-mri
8: https://www.e-neurospine.org/journal/view.php?number=1714
9: https://www.frontiersin.org/journals/medicine/articles/10.3389/fmed.2025.1531637/full
10: https://deukspine.com/blog/true-cost-of-spinal-fusion


