


By Dr. Ara Deukmedjian, MD – Board Certified Neurosurgeon
Key Points
✓ An X-ray cannot diagnose a herniated disc. MRI is the only imaging tool that accurately shows what is happening to the soft tissues in your spine. If no current MRI exists, no treatment should be on the table yet.
✓ There are nearly 10 different terms for the same category of disc injury: bulge, herniation, protrusion, extrusion, sequestration. They are not interchangeable, and the confusion they create is one of the most common reasons patients end up with the wrong treatment plan.
✓ A bulging disc and a herniated disc are anatomically different. A bulge means the outer wall is intact but weakened. A herniation means it has torn and inner disc material has escaped into the spinal canal. Despite that distinction, the treatment approach is often the same for both.
✓ Pain level does not predict injury severity. A large extrusion can hurt less than a small protrusion compressing the right nerve root. The MRI finding drives the diagnosis; not how much it hurts.
✓ Traditional surgery removes the disc fragment. Deuk Laser Disc Repair® repairs the damaged material and seals the annular tear through a 4–7 mm incision, with no disc removal and no fusion. Motion is fully preserved.

Disc problems, such as bulging and herniated discs, are common causes of back and neck pain. These conditions occur when the cushion-like discs between your vertebrae are damaged, potentially pressing on surrounding nerves and causing symptoms like sciatica. Magnetic resonance imaging (MRI) is the definitive non-invasive imaging tool used by healthcare providers to accurately visualize the spine’s soft tissues. The clarity provided by the MRI is essential for distinguishing among various disc injuries, which is the crucial first step in creating an effective, personalized treatment plan.
The Conditions: Bulge vs. Herniation
In a general sense, bulging and herniated discs fall under the same category of spinal conditions, though they are anatomically distinct. In fact, there are nearly 10 different terms used to describe these disc conditions, which is one of the leading sources of patient confusion. For a full breakdown of what each term means, see our guide on herniated disc, bulging disc, and slipped disc terminology.
A bulging disc involves the disc extending beyond its normal space, whereas a herniated disc occurs when the inner material actually breaks through the outer layer. Despite these anatomical differences, the treatment approach is often the same, as both conditions can result in similar levels of discomfort. Because the severity of the pain doesn’t always correlate with the type of displacement, distinguishing between these terms is vital for a precise reading of an MRI and for tailoring a recovery plan.

Image: Cross-section diagram of a spinal segment showing the vertebra, spinal cord, spinal nerve, and the intervertebral disc with its outer layer (annulus fibrosus) and inner core (nucleus pulposus).
Bulging Disc: A Contained Protrusion
A bulging disc is generally the milder of the two conditions. It occurs when the intervertebral disc extends outward around its entire circumference, or at least more than 25% of the perimeter.
- Anatomy: The disc’s tough outer wall (the annulus fibrosus) is stretched, weakened, and bulging, but it remains intact.
- Significance: It is often considered a normal sign of age-related wear (degenerative disc disease). It may be asymptomatic or cause symptoms only if the broad outward push irritates a nerve.
Herniated Disc: A Ruptured Containment
A herniated disc (sometimes called a “slipped disc”) involves a tear or rupture in the outer wall of the disc.
- Anatomy: The inner, jelly-like material (nucleus pulposus) leaks out through the tear and directly into the spinal canal.
- Significance: Because the inner material is highly inflammatory, a herniation is more likely to cause acute, severe symptoms such as sharp, radiating pain (radiculopathy or sciatica) due to direct nerve root compression and chemical irritation.
Patient Success
Years of pain from a herniated disc relieved!

Decoding Disc Pathology on Your MRI Report
The radiologist uses specific, precise terminology to classify a disc injury based on the images. This classification informs the treatment plan, differentiating between a general bulge and a true tear.
Disc bulge:
- Intact, but stretched and weakened.
- Contained within the outer wall.
- Broad-based, extending outward across 25% of the disc’s circumference.
Disc herniation:
- Torn or ruptured.
- Leaks out through the tear into the spinal canal.
- Focal, with disc material displaced outside the disc space.
Further Classification of Herniation on an MRI
Disc herniations are further classified based on the shape of the displaced material. This information is critical for surgical planning.
- Disc protrusion (contained herniation):
- Key MRI feature: The displaced material is focal (involving less than 25% of the circumference), and the base (the part touching the parent disc) is wider than the dome or tip of the material extending into the spinal canal.
- Significance: Indicates a focal weakness or partial tear; the material is somewhat contained.
- Disc extrusion (non-contained herniation):
- Key MRI feature: The displaced material has a narrower base at the site of exit than the material extending into the spinal canal. This often gives it a “mushroom” shape.
- Significance: The inner material has broken through the entire outer disc wall. Extrusions are highly inflammatory and often require targeted pain management.
- Disc sequestration (free fragment):
- Key MRI feature: A fragment of the extruded disc material has broken off completely from the parent disc and is now a “free fragment“ floating in the spinal canal.
- Significance: These fragments can cause multi-level compression but sometimes have a higher chance of being reabsorbed by the body’s immune system over time. Monitoring a free fragment often involves repeat MRIs to track its size and location.
Get Answers. Find Relief.
Upload your latest MRI for a complimentary review and personal consultation with Dr. Deukmedjian to start your pain-free journey.

Interpreting the Impact: Nerve Impingement and Stenosis
The most critical information in your MRI report concerns how the disc is affecting the adjacent nerves and spinal structures.
Nerve Impingement (Compression)
The radiologist will specifically note whether the disc material is touching, displacing, or compressing a nerve root. This finding confirms the source of your radiating symptoms.
- Grading compression: Reports often use terms like “mild effacement,” “moderate compression,” or “severe displacement” to grade the severity of nerve root involvement. A severe compression is a key indicator for advanced non-invasive or surgical treatment consideration.
- Common site: The L5-S1 disc is the most frequently affected level, often compressing the S1 nerve root, which causes classic sciatica symptoms down the back of the leg and into the foot.
Spinal Stenosis
A large disc abnormality, often combined with age-related changes like bone spurs, can narrow the space available for the spinal cord or nerve roots.
- Central canal stenosis: Narrowing of the main spinal canal, which can impact the spinal cord itself.
- Foraminal stenosis: Narrowing of the small opening (foramen) where the nerve root exits the spine.
Measuring the stenosis: The MRI allows providers to accurately measure the remaining cross-sectional area of the spinal canal. This measurement helps determine the functional impact of the disc on the patient’s mobility, especially when standing or walking, and guides the treatment plan toward decompression if necessary.
Treatment Options Guided by MRI Findings
The specific findings on your bulging disc MRI or herniated disc MRI provide the roadmap for precision treatment, ensuring that interventions are targeted and effective.
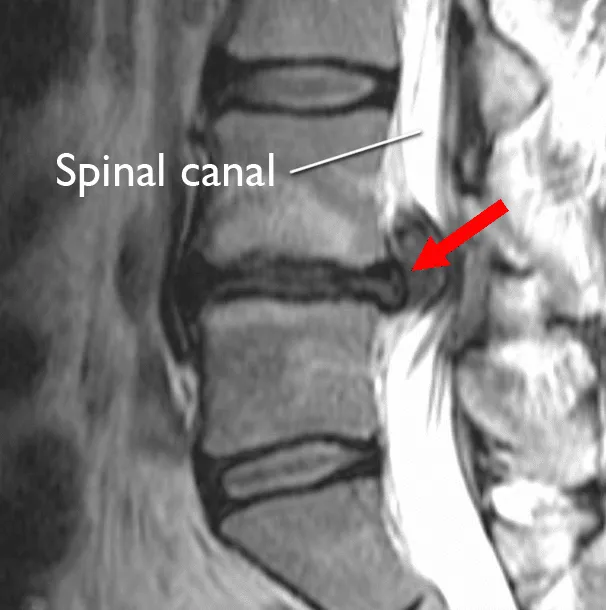
Image: MRI of a herniated disc in the lower back.
Non-Surgical Treatments
- Epidural steroid injections (ESIs): The MRI is absolutely vital for ESIs. The image allows the physician to identify the exact nerve root being compressed (e.g., the right L5 nerve root) and the safest approach for delivering the anti-inflammatory medication directly to the inflamed area under X-ray guidance (fluoroscopy).
- Physical therapy (PT): The MRI helps guide the physical therapist, indicating which movements (e.g., specific spinal flexion or extension) should be avoided or emphasized to prevent further irritation of the injured disc.
- Spinal decompression therapy: This non-invasive treatment is most effective for certain types of bulging discs and contained protrusions, as it gently creates negative pressure within the disc space to promote retraction.
Criteria for Surgical Intervention
For most patients, non-surgical treatment resolves symptoms. Surgery is reserved for cases where:
- Non-operative care fails: Persistent, debilitating pain lasts for 6 weeks or more despite consistent, appropriate conservative treatment.
- Progressive neurological deficits: The patient experiences worsening weakness (e.g., foot drop) or loss of bowel/bladder function (Cauda Equina Syndrome—an emergency).
Herniated and Bulging Disc Treatment
Learn how Dr. Deukmedjian cures herniated and bulging discs at the Deuk Spine Institute.

Bulging and Herniated Disc Surgical Options
Minimally invasive microdiscectomy: This surgery is common for symptomatic herniated discs (protrusions or extrusions). It involves a small incision to remove only the part of the disc compressing the nerve. The surgeon relies entirely on the MRI to confirm the affected level and the side of the compression before planning the procedure, ensuring precision and high success rates.
Deuk Laser Disc Repair®: A Minimally Invasive Alternative
Traditional surgeries for herniated and bulging discs, such as standard microdiscectomy, involve removing the disc fragment causing compression. However, advanced options like Deuk Laser Disc Repair® (DLDR) and Deuk Plasma Rhizotomy® (DPR) offer a highly precise, minimally invasive alternative.
The procedure is designed to treat both bulging and herniated discs by:
- Precision targeting: Utilizing the MRI findings to guide the surgery, the surgeon precisely accesses the disc through a small incision.
- Removing damaged tissue: A state-of-the-art laser is used to vaporize the painful disc material—the bulge or herniation—without damaging the surrounding bone, nerves, or healthy disc tissue.
- Sealing the annulus: Unlike traditional procedures that may leave the tear open, this technique focuses on repairing and sealing the annular tear, which is often the source of chronic pain and prevents the nucleus pulposus from leaking again.
Make Your First Pain-Free Move
If you’re seeking relief from lumbar pain, have been recommended for a TLIF spinal fusion, or are still dealing with chronic neck pain after a failed fusion surgery, we can help improve your quality of life and enable you to live pain-free.
Upload your latest MRI for a free review and a personal consultation with myself. Ara Deukmedjian, M.D., founder of Deuk Spine Institute and creator of the Deuk Laser Disc Repair® procedure.
Frequently Asked Questions
-
Is a broad-based disc bulge the same as a herniated disc?
No. A broad-based disc bulge is distinct from a herniated disc. A bulge means the outer disc wall is weakened and stretched but still intact, extending broadly around the disc’s circumference. A herniated disc involves a definite tear or rupture in the outer wall, allowing the inner material to displace focally into the spinal canal. While both can cause symptoms, the herniation is generally considered more anatomically severe.
-
Does an annular tear always indicate a herniated disc?
Not necessarily. An annular tear (or annular fissure) is a tear in the outer disc wall (annulus fibrosus). It is visible on an MRI and can cause localized back pain, sometimes noted as a “High-Intensity Zone” (HIZ). A herniated disc occurs only if that tear is large enough to allow the inner disc material to push out (protrusion) or leak out (extrusion). A tear can exist without an accompanying mass that compresses a nerve.
-
Why is the L5-S1 disc a common area for a disc herniation?
The L5-S1 disc, located at the very bottom of the lumbar spine where the spine connects to the sacrum, is the most frequently affected level for several reasons. It carries the highest load of the body’s weight and is subject to the most shear force during bending, twisting, and lifting. This mechanical stress makes it highly susceptible to degenerative changes, disc flattening, and subsequent herniation.


