

By Dr. Ara J. Deukmedjian, MD
Board-Certified Neurosurgeon
Medically reviewed on June 10, 2026
Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
Key Points
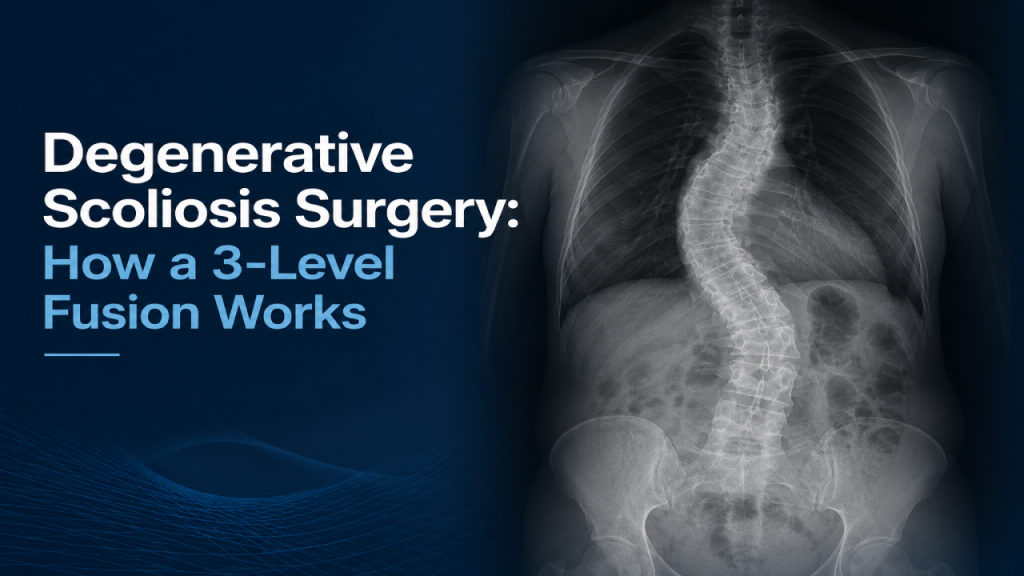
✓ The patient had adult degenerative (de novo) scoliosis across L2-3, L3-4, and L4-5 with spinal stenosis, lateral listhesis, and segmental instability driving worsening back and leg pain. Her L5-S1 level was normal and her bone was notably soft (osteoporotic). ¹
✓ The facet joints were enlarged, sclerotic, and rigid, so the curve could not be corrected with screws alone. Three-level posterior facet osteotomies were required to free the spine before it could be realigned.
✓ A wide decompression removed the hypertrophied facets and thickened ligamentum flavum to relieve stenosis. Fusing a patient without first clearing the stenosis would lock in permanent leg pain.
✓ Supine MRI can underestimate this kind of pathology, because stenosis and listhesis often worsen only when the spine is loaded standing. That is a key reason imaging findings and symptoms sometimes disagree. ²
✓ Transforaminal interbody cages packed with allograft and autograft bone restored disc height and derotated the spine, and bilateral L2 through L5 pedicle screw and rod fixation with cross links stabilized the correction in all planes. In soft bone, larger and longer screws and more fixation points improve hold. ³
✓ The performed fusion under neuromonitoring with notably low blood loss, the case ended with the deformity realigned into normal lordosis, the nerves decompressed, the patient stable, and same-day discharge expected.

Why This Patient Needed Surgery
Scoliosis comes in two broad forms. Idiopathic scoliosis develops earlier in life with no clear cause, while degenerative scoliosis (also called “de novo” scoliosis) develops later, when the discs and facet joints wear out asymmetrically and the spine slowly tilts and rotates off its normal axis. This patient had degenerative scoliosis with the apex of her curve pointing to the left, spanning L2-3, L3-4, and L4-5. Her L5-S1 level was healthy and left alone.

Three things made her a surgical candidate rather than someone who could keep managing symptoms conservatively. First, the curve was tied to segmental instability: one vertebra was sliding sideways relative to the next (a lateral listhesis), and the segment shifted and twisted as she loaded her spine. Second, that instability was producing spinal stenosis, the narrowing that pinched nerves and generated new, worsening leg symptoms. Third, her bone was soft (osteoporotic), which would shape every technical decision that followed. In adult degenerative scoliosis, surgery is generally reserved for exactly this picture: progressive deformity, instability, and nerve compression that conservative care no longer controls. ¹
A telling sign of how rigid her spine had become was the state of the facet joints, which are normally smooth, mobile joints. Hers were enlarged, sclerotic (hardened), and locked down with bone spurs. This is the body’s own attempt at a fix: when a joint moves abnormally, the body thickens the facet, the joint capsule, and the surrounding ligaments to try to splint it. The result is a self-made cage of overgrown bone and ligament that both pinches nerves and prevents the spine from being straightened.
Why the MRI Did Not Tell the Whole Story
One of the most useful teaching points in this case has nothing to do with the operating room. A standard MRI is taken with the patient lying down, hips and knees slightly flexed, a position that opens up the spinal canal and foramina and makes stenosis look milder than it is in real life. Symptoms, however, show up when a person stands, walks, and loads the spine, which is exactly when an unstable, scoliotic segment shifts, twists, and narrows around the nerves.
That mismatch is well documented: supine MRI has meaningful false negative rates for stenosis and can miss the listhesis that only appears under load, which is why imaging findings and a patient’s symptoms sometimes disagree. ² For a patient like this one, the surgeon expected to find more narrowing in the operating room than the supine images suggested, and did.
Step One: Releasing the Spine With Facet Osteotomies
With soft bone, the tempting shortcut, placing screws and simply torquing the curve straight, is the wrong move, because the screws would loosen or pull out, or the pedicles would fracture. The durable solution is to remove the abnormal facet joints first so the spine can rotate freely, then realign it.
That removal is a posterior facet osteotomy, performed at all three levels. Using a high-speed drill and an osteotome, the rigid, overgrown joints are cut and lifted out. Because the joints were so scarred and hypertrophied, freeing each one took deliberate, controlled force. An important technical detail: it is not enough to remove the upper facet. The tip of the superior articular process below it has to come out too, since it would otherwise dig into the nerve’s exit tunnel and physically block realignment when the spine is derotated. Each osteotomy does double duty, eliminating a fixed point that resists correction while simultaneously opening the lateral recess and foramen where nerves were being squeezed.
Clearing the Nerves: Decompression
Running alongside the bone work is the decompression. The ligamentum flavum, a normally thin ligament inside the canal, was two to three times thicker than it should be, part of that same stabilizing overgrowth, and it was pinching nerves. Removing it, along with the hypertrophied facets, reopens the lateral recess and foramen.
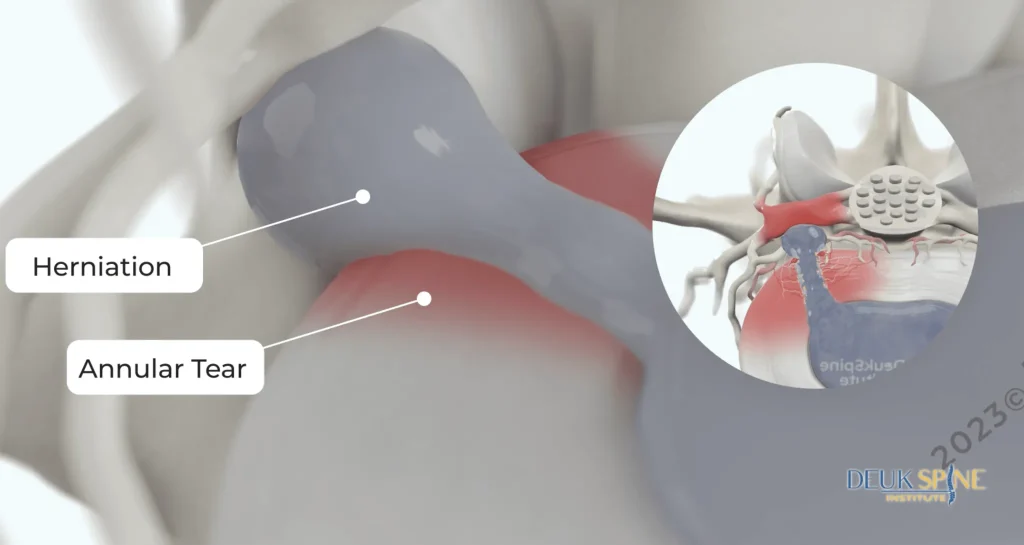
The guiding principle here is simple and consequential: never fuse a patient over residual stenosis. Once a segment is fused, any narrowing left behind is locked in, and the leg pain it causes becomes permanent. The decompression also has to anticipate the correction itself. As the curve is straightened, the concave side of the curve closes down, so a foramen that looks fine before correction can pinch a nerve afterward. For that reason the decompression is intentionally wide, especially on the side that will tighten, to avoid trading one nerve problem for another.
Rebuilding the Disc Spaces: Interbody Fusion
With the facets gone, the vertebrae could finally move, and that mobility is what makes correction possible. The discs were removed and the spaces rebuilt through a transforaminal approach, working through Kambin’s triangle, the small safe corridor between the exiting and traversing nerve roots. In a spine rotated by scoliosis, that corridor is even tighter than usual, and the epidural veins tethering the nerve roots had to be coagulated and released before the roots could be safely moved aside.
Each cleaned disc space was then filled with an interbody cage packed with bone graft. Two graft types were used together: allograft (donor bone) and autograft (the patient’s own bone). The patient’s cancellous bone is prized because it carries all three properties of an ideal fusion graft. It is osteoconductive (a scaffold), osteoinductive (it signals bone formation), and osteogenic (it contains living stem cells), while many grafts offer only one or two. As the cages restored disc height, they also derotated and realigned the spine, taking advantage of ligamentotaxis: because the ligaments stay attached to the bone, distracting the space pulls the vertebrae back toward their natural alignment. The spine was deliberately set into lordosis (its normal inward curve), which is the posture that gives the best long-term result.
Locking In the Correction: Screws, Rods, and Cross Links
Only after the spine was realigned did the instrumentation go in. Pedicle screws were placed bilaterally at L2, L3, L4, and L5, eight screws in total, entering at the base of the superior facet where it meets the transverse process and angling from lateral to medial into the vertebral body, with fluoroscopy confirming position. Every pilot hole was “sounded” with a ball-tipped probe to confirm it had not broken through the pedicle wall, and the placed screws were electrically stimulated to confirm none were sitting against a nerve.
Soft bone changed the screw strategy. Bigger, longer screws grip better, and biomechanical data backs this up: larger diameter, longer pedicle screws increase pullout strength, with osteoporotic bone being the central challenge to fixation. ³ Weak bone also argues for more points of fixation rather than fewer, so a long, well-anchored construct is less likely to loosen or fail.
The rods were contoured to the corrected shape, bent gradually across several points rather than sharply in one spot (a sharp single bend would weaken the metal and invite fatigue failure), and locked to the screw heads with set screws. A final, often-skipped step was adding cross links between the rods. Screws and rods alone create a tension band that controls flexion and extension but do little to stop rotation. Cross links restore rotational control, so the fused segment is stabilized in all planes.
What Each Stage of the Operation Accomplished
Finishing the Case: Pain Control and Infection Prevention
Before closing, the paraspinal muscles were injected with Exparel (a long-acting local anesthetic) to control pain and reduce reliance on narcotics, and intrawound vancomycin powder was placed to lower the risk of deep wound infection, a common practice supported by retrospective evidence, though high-quality prospective data remain limited. ⁴ A drain was placed and the wound closed. Throughout a long, multilevel open operation, blood loss stayed remarkably low, reflecting careful hemostasis, blood pressure control, and positioning. By the end of the broadcast the deformity had been realigned into a normal lordosis, the nerves were decompressed, the patient was stable, and she was expected to go home within a couple of hours.
What You Should Do
This operation is a powerful tool for a specific problem: a genuinely unstable, progressive deformity with nerve compression. It is also a large procedure, and it is not the answer for most back or neck pain. The same symptoms, such as leg pain, a “pinched nerve,” or a bad disc, are far more often driven by conditions that do not require removing the facets, eliminating motion, or fusing the spine. The fact that a fusion can be done well does not mean it is the right operation for a given patient.
If a spinal fusion has been recommended to you, two questions are worth asking before consenting. First, is my problem a true structural deformity or instability that requires fusion, or a disc or nerve problem that a less invasive, motion-preserving option could treat? Second, has my imaging been evaluated with my symptoms and my loaded, standing spine in mind, not just a single supine MRI? A second opinion on those questions is not a delay in care. It is the most reasonable step before committing to a permanent change to your spine.

Frequently Asked Questions
What is degenerative scoliosis?
Degenerative (de novo) scoliosis is a sideways curvature of the spine that develops later in life as the discs and facet joints wear out unevenly, causing the spine to tilt and rotate. Unlike idiopathic scoliosis, which appears earlier without a clear cause, degenerative scoliosis is driven by age-related degeneration and is often accompanied by spinal stenosis and instability. ¹
Does degenerative scoliosis always require surgery?
No. Most patients are managed conservatively first. Surgery is generally reserved for progressive deformity, instability, and nerve compression with symptoms that conservative care no longer controls. The decision depends on the curve, the symptoms, and the patient’s overall health, not the X-ray alone. ¹
Why are the facet joints removed during scoliosis correction?
When the facet joints become enlarged, hardened, and locked down, they physically prevent the spine from being realigned. Removing them with osteotomies frees the vertebrae to rotate back toward normal alignment and, at the same time, helps decompress the pinched nerves nearby.
Can an MRI miss spinal stenosis?
Yes. A standard MRI is taken lying down, which opens the spinal canal and can make stenosis look milder than it is. Stenosis and slippage often worsen only when the spine is loaded standing, so supine imaging can underestimate the problem. That is one reason imaging and symptoms sometimes disagree. ²
Is spinal fusion the only option for back or leg pain?
No. Fusion is one tool, best suited to true deformity and instability. Many causes of back and leg pain can be treated with less invasive, motion-preserving options. If fusion has been recommended, it is reasonable to ask whether a smaller procedure could address your specific diagnosis.
How is the spine actually straightened in this surgery?
Through a combination of steps: removing the rigid facet joints, clearing the discs, inserting interbody cages that restore height and derotate the segment, and then holding the correction with pedicle screws, rods, and cross links. Because the ligaments stay attached to the bone, distracting the disc spaces also helps pull the vertebrae back into alignment.
Sources
- Cho KJ, et al. Adult degenerative scoliosis: decompression vs. decompression with fusion. J Neurosurg Spine. 2018;29(3):259-266.
- Upright positional MRI of the lumbar spine. Clin Radiol. 2008.
- Screw diameter and length in pedicle screw fixation of osteoporotic bone: a finite element analysis. Asian Spine J. 2021.
- Ghobrial GM, et al. Intrawound vancomycin powder and infection after spinal surgery: a systematic review. Neurosurg Focus. 2019;46(1):E18.
 in Lumbar MRI Imaging")

