


By Dr. Ara Deukmedjian, MD
Board-Certified Neurosurgeon, Deuk Spine Institute
Medically reviewed on March 18, 2026
Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
Key Points
Before diving into the details, here is what you need to know about cervical spinal stenosis:
✓ Cervical spinal stenosis is a narrowing of the spinal canal in the neck: When the canal narrows, it compresses the spinal cord and nerve roots, producing a range of neurological symptoms that can progress if left untreated.
✓ It is primarily a degenerative, age-related condition: Bone spurs, herniated discs, thickened ligaments, and arthritic joint changes are the most common contributors.
✓ Symptoms can range from neck stiffness to paralysis: Depending on the severity of compression, symptoms may include radiating arm pain, numbness, weakness, balance problems, and in advanced cases, loss of bladder or bowel control.
✓ MRI is the gold standard for diagnosis: Imaging is essential to confirm the location and severity of compression and to guide treatment planning.
✓ Conservative treatment helps manage symptoms but does not fix the structural problem: Physical therapy, medications, and steroid injections can reduce pain temporarily, but they do not reverse the narrowing of the spinal canal.
✓ When surgery is needed, the approach matters enormously: Traditional cervical fusion (ACDF) eliminates motion at the fused level and carries a well-documented risk of adjacent segment disease, with reoperation rates of 6.57% and ASD incidence as high as 21% in five-year follow-up studies.
✓ Motion-preserving alternatives are available:Deuk Laser Disc Repair® treats disc-related cervical stenosis without fusion, without hardware, and without the motion loss and adjacent segment risk that come with traditional surgery.
✓ Early intervention leads to better outcomes: Research consistently shows that patients who receive timely treatment before significant neurological deterioration occurs recover more fully than those who delay.
✓ A second opinion from a specialist in minimally invasive spine surgery can change your outcome: Many patients are offered only fusion because it is what their surgeon knows. An independent evaluation may reveal superior options.

Cervical Spinal Stenosis: Symptoms, Causes, Diagnosis, and Treatment
Neck pain is one of the most common musculoskeletal complaints seen in medical practice, but when it is accompanied by symptoms traveling down the arm, such as numbness, tingling, weakness, or a loss of fine motor control, it frequently signals something more serious than a simple muscle strain. One of the most important conditions to evaluate in this clinical picture is cervical spinal stenosis.
Left unaddressed, cervical spinal stenosis can progress from a manageable source of discomfort into a condition causing permanent neurological damage, loss of coordination, and in the most severe cases, spinal cord dysfunction that is irreversible. Understanding what it is, how it develops, and what modern treatment options exist is essential for anyone experiencing these symptoms.
This guide covers the definition of cervical spinal stenosis, its causes and symptoms, how it is diagnosed, and the full spectrum of treatment options available today, including the most advanced minimally invasive surgical alternative.
What Is Cervical Spinal Stenosis?
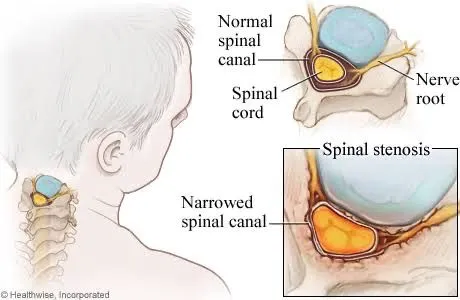
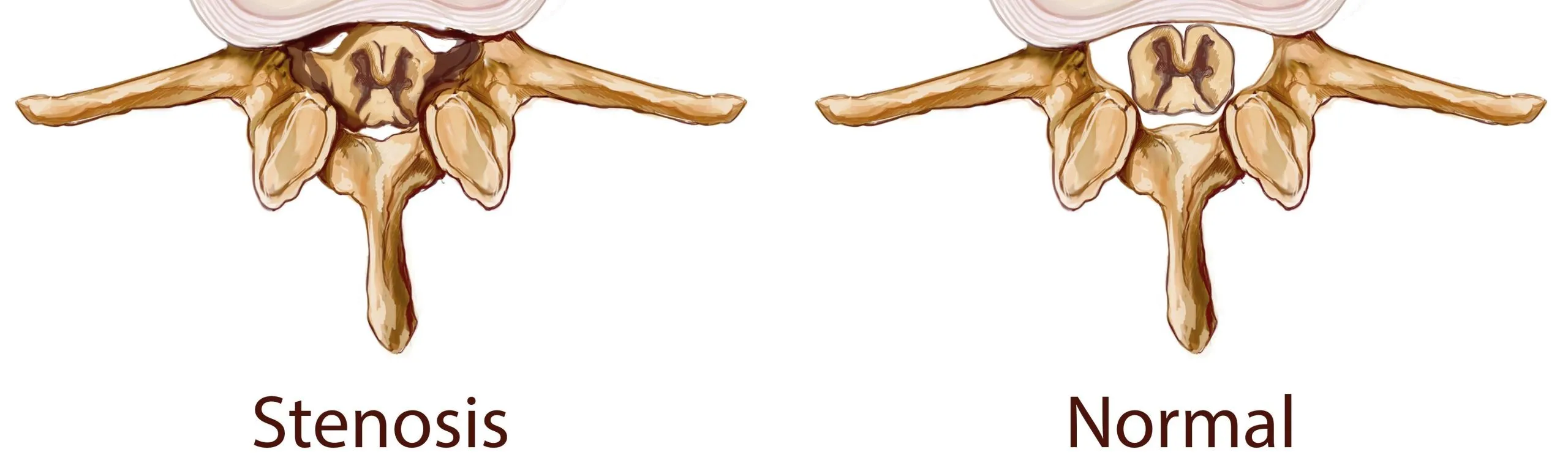
Cervical spinal stenosis (CSS) is the narrowing of the spinal canal within the cervical spine, the seven vertebrae that make up the neck. 1 The spinal canal is the bony tunnel formed by stacked vertebrae that protects the spinal cord and the nerve roots traveling from the brain to the rest of the body. When this canal narrows, whether gradually through degeneration or more acutely through injury or disc herniation, it compresses these delicate neural structures. The result is a spectrum of neurological symptoms that can significantly impair quality of life and, if untreated, cause irreversible damage.
CSS can affect the spinal cord itself (a condition called cervical myelopathy) or the individual nerve roots exiting the spinal canal (cervical radiculopathy), or both simultaneously. 2 The distinction matters clinically, as myelopathy represents a more serious and urgent form of the condition.
According to the most current data from StatPearls, the upper neck and lower back are the most commonly affected regions for spinal stenosis across all age groups, and the condition is strongly associated with the natural aging process. 3 Prevalence increases substantially after age 50, and with the aging of the global population, the number of patients affected is rising steadily.
Causes of Cervical Spinal Stenosis
CSS is primarily a degenerative condition, meaning it develops over time as the structures of the cervical spine gradually wear down. In most patients, multiple contributing factors are present simultaneously.
Age-Related Degeneration
The gradual breakdown of spinal structures is the most common underlying cause of CSS. Over decades of use, intervertebral discs lose height and fluid content, vertebral joints develop arthritic changes, and surrounding ligaments can thicken and calcify. These changes collectively reduce the space available within the spinal canal.
Bone Spurs (Osteophytes)
As the joints and disc spaces of the cervical spine degenerate, the body attempts to compensate by forming new bone at the margins of the vertebrae. These bony projections, called osteophytes or bone spurs, can directly encroach on the spinal canal or neural foramen, compressing the cord or nerve roots.
Bulging and Herniated Discs
The intervertebral discs that cushion each cervical vertebra can bulge outward or herniate when their outer wall (the annulus fibrosus) weakens or tears. This displaced disc material reduces the available space in the canal and can compress nerve roots or the cord directly. Disc-related compression is particularly important in younger patients with CSS.

Thickened Ligaments
The ligamentum flavum, which runs along the back of the spinal canal, can hypertrophy and buckle into the canal with age. This is one of the most common contributors to posterior cord compression in degenerative CSS.
Facet Joint Arthritis
Osteoarthritis of the facet joints, the small paired joints at the back of each vertebra, causes bony enlargement and inflammation that can narrow the neural foramen and the central canal.

Congenital Narrowing
Some individuals are born with a naturally narrower cervical spinal canal than average. These patients may develop symptomatic stenosis earlier in life and often experience more rapid progression when degenerative changes do develop.
Symptoms of Cervical Spinal Stenosis
The symptoms of CSS depend on whether the nerve roots, the spinal cord, or both are being compressed.
Cervical Radiculopathy Symptoms (Nerve Root Compression)
- Radiating pain traveling from the neck into the shoulder, arm, or hand, often following a specific nerve distribution
- Tingling or “pins and needles” sensation in the arm or fingers
- Numbness in the arm, hand, or specific fingers
- Weakness in specific muscle groups of the arm or hand
- Worsening of symptoms with neck extension or rotation
Cervical Myelopathy Symptoms (Spinal Cord Compression)
- Chronic neck pain or stiffness that may be relatively mild even when cord compression is significant
- Loss of fine motor skills, such as difficulty buttoning a shirt, writing, or using utensils
- Weakness in the arms or legs that is not limited to a single nerve distribution
- Balance and coordination problems, including an unsteady or shuffling gait (ataxia)
- Diffuse numbness or tingling affecting the hands, arms, or legs
- In advanced cases, loss of bladder or bowel control
Myelopathy symptoms in particular should prompt urgent evaluation. Research consistently shows that patients with cervical myelopathy who receive timely surgical treatment recover more fully than those who delay, and that neurological deterioration from untreated myelopathy can become permanent.
What Happens If Cervical Spinal Stenosis Is Left Untreated?
Because CSS is a progressive condition, the risks of delaying evaluation and treatment are significant. As compression worsens over time:
- Neurological deficits increase: Weakness, numbness, and tingling in the arms and hands can become more severe and more permanent.
- Myelopathy progresses: Spinal cord dysfunction leads to worsening balance problems, gait instability, and difficulty walking.
- Permanent nerve damage accumulates: Prolonged compression of the spinal cord or nerve roots can cause irreversible loss of sensation, motor function, and muscle mass.
- Bladder and bowel dysfunction can develop: In the most advanced cases, significant cord compression can disrupt autonomic function.
A 2025 systematic review examining surgical timing for degenerative cervical myelopathy, published in EFORT Open Reviews, confirmed that earlier surgical intervention is consistently associated with better neurological outcomes, particularly in patients who have not yet reached severe functional impairment. 4 Waiting until symptoms are advanced significantly reduces the likelihood of full recovery.
Diagnosing Cervical Spinal Stenosis
An accurate diagnosis is the foundation of effective treatment. No two patients with CSS present identically, and treatment decisions depend entirely on the specific location, cause, and severity of compression identified through clinical evaluation and imaging.
Physical and Neurological Examination
The diagnostic process begins with a thorough physical and neurological examination. The physician assesses reflexes, sensation, muscle strength, balance, coordination, and gait to identify the pattern and extent of any neurological deficits. Specific provocative maneuvers, such as the Spurling test (neck extension and rotation toward the symptomatic side), can help confirm the presence of nerve root compression.
MRI: The Gold Standard
Magnetic resonance imaging (MRI) is the definitive diagnostic tool for cervical spinal stenosis. MRI provides high-resolution images of soft tissue structures, allowing clear visualization of disc herniations, thickened ligaments, the degree of cord compression, and whether cord signal changes (an indicator of myelopathy severity) are present. 5 For most patients, MRI is both necessary and sufficient to confirm the diagnosis and guide treatment.
Get a free virtual consultation with Dr. Deuk. Submit your MRI to pinpoint the cause of your back pain and explore minimally invasive treatment options.

CT Scan
Computed tomography (CT) scanning is particularly useful for visualizing bony structures, making it the preferred tool for identifying bone spurs and ossification of the posterior longitudinal ligament (OPLL). 6 CT is often used when MRI is contraindicated, for example in patients with certain metallic implants or pacemakers, and is frequently combined with myelography (contrast injection into the spinal fluid) in complex diagnostic situations.
Electrodiagnostic Studies
Electromyography (EMG) and nerve conduction studies (NCS) can help differentiate cervical radiculopathy from peripheral nerve entrapment syndromes such as carpal tunnel syndrome, and can quantify the degree of nerve injury. These studies are often ordered when the clinical picture is ambiguous or when multiple potential diagnoses exist.
Non-Surgical Treatment for Cervical Spinal Stenosis
For patients with mild to moderate symptoms who do not have significant or progressive neurological deficits, conservative management is typically the appropriate first step. It is important for patients to understand clearly what conservative treatment can and cannot achieve.
Conservative treatments manage pain and may slow the functional impact of CSS. They do not reverse the structural narrowing of the canal.
Physical Therapy
A specialized physical therapy program focused on the cervical spine can improve posture, strengthen the muscles that support the neck, improve flexibility, and reduce the mechanical load on compressed neural structures. Aquatic therapy is often particularly well-tolerated in patients with severe symptoms. Physical therapy is one of the most important components of conservative management and should be tailored specifically to the cervical spine.

Medications
Non-steroidal anti-inflammatory drugs (NSAIDs) reduce inflammation and can provide meaningful pain relief. Nerve-specific medications such as gabapentinoids (gabapentin, pregabalin) may help manage radiating neuropathic pain. Muscle relaxants are used short-term for associated cervical muscle spasm. Oral corticosteroids may be used briefly for severe flares.

Epidural Steroid Injections
Epidural steroid injections (ESIs) deliver corticosteroids directly to the epidural space near the compressed nerve root. They can provide temporary but significant reduction in inflammation and pain. ESIs are useful for short-term symptom management and for allowing patients to engage more effectively in physical therapy. Their effects are temporary and do not address the underlying structural narrowing.

Activity Modification
Avoiding activities and positions that worsen symptoms, particularly sustained neck extension, can reduce the intensity of symptoms during periods of flare. Ergonomic adjustments to workstations and sleep positioning are often helpful.
When conservative treatment fails to provide adequate relief, when symptoms are severe or worsening, or when neurological deficits are progressing, surgical decompression becomes necessary and appropriate.
Surgical Treatment for Cervical Spinal Stenosis
The goal of surgery for CSS is decompression: creating sufficient space for the compressed spinal cord and nerve roots to relieve pressure, stop neurological deterioration, and allow recovery. 7 The surgical approach and specific technique chosen depend on the location and cause of the compression, the number of levels involved, and the patient’s anatomy and overall health.
Traditional Anterior Cervical Discectomy and Fusion (ACDF)
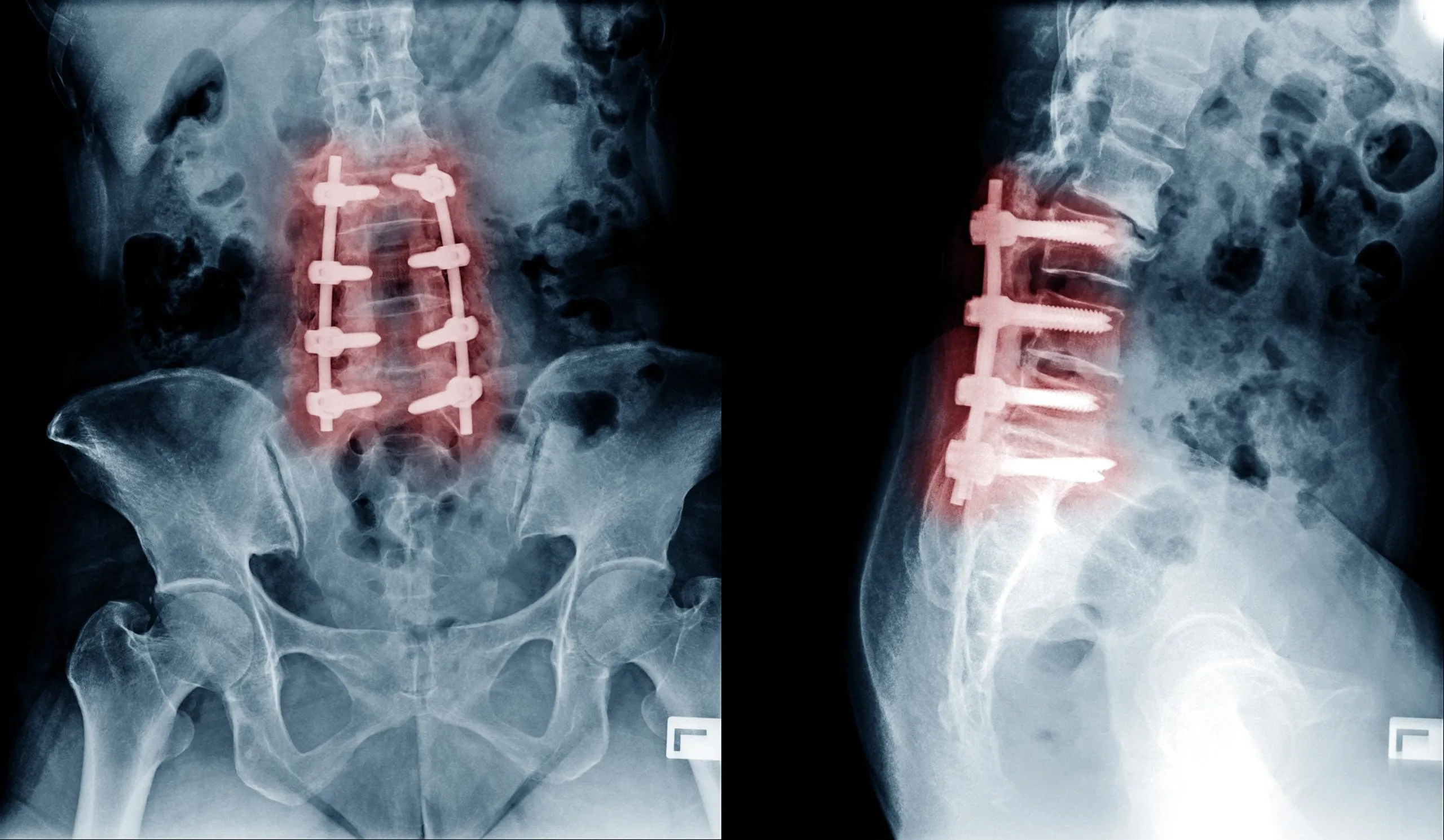
ACDF is the most commonly performed cervical spine surgery in the United States, with more than 130,000 procedures performed annually. The surgeon approaches the spine through the front of the neck, removes the herniated disc or bone spurs causing compression, and permanently fuses the adjacent vertebrae using a bone graft and metal plate.
ACDF can effectively relieve arm pain and neurological symptoms for appropriately selected patients. However, it permanently eliminates motion at the fused level, and this loss of motion transfers increased mechanical stress to the adjacent spinal segments.
The long-term consequences of this stress transfer are well-documented. A 2025 PMC review of risk factors and treatment strategies for adjacent segment disease (ASD) confirmed that cervical fusion consistently alters spinal biomechanics, increasing intradiscal pressure and range of motion at adjacent levels and accelerating degeneration there. 8 Published ASD rates following ACDF range from 6.57% requiring reoperation to 21% in five-year follow-up studies depending on how ASD is defined and the population studied. Younger patients who undergo cervical fusion face decades of elevated adjacent segment stress, making this risk particularly meaningful for anyone under 50 who receives this procedure.

Laminectomy and Laminoplasty
Laminectomy removes the lamina from one or more cervical vertebrae to decompress the spinal cord from behind. Laminoplasty expands the spinal canal by creating a hinge in the lamina rather than removing it entirely, preserving more posterior stability. Both approaches are typically used for multi-level cord compression and for patients in whom anterior surgery is not feasible. Because posterior bone removal can create instability, laminectomy is frequently combined with instrumented fusion.
The Superior Alternative: Deuk Laser Disc Repair

For patients whose cervical stenosis is caused by disc-related compression, including herniated discs, bulging discs, bone spurs arising from the disc level, and annular tears, Deuk Laser Disc Repair (DLDR) offers a definitively superior approach to traditional fusion.
What it is: DLDR is a minimally invasive, motion-preserving procedure performed through an incision no larger than a pencil eraser (4 to 7 mm). Using a high-definition endoscopic camera and a precision FDA-approved Holmium:YAG laser, the surgeon removes the specific disc tissue, bone spurs, and thickened tissue causing the canal narrowing, without fusing the vertebrae, cutting major muscle groups, or implanting any hardware.
How it works: Using live fluoroscopic imaging, a small tube is guided into the symptomatic disc. The endoscopic camera is inserted to visualize the area precisely. The laser then removes only the 5 to 10% of damaged disc tissue causing herniation and inflammation, and treats the annular tear that is the source of discogenic pain, leaving healthy disc structure completely intact.
Key advantages over ACDF:
- No fusion: The cervical spine retains its full natural range of motion permanently. There is no adjacent segment disease risk because no fusion is performed.
- No hardware: No screws, plates, or cages means no hardware complications, no hardware failure, and no need for future hardware removal surgery.
- No muscle cutting: The approach does not disrupt the major muscle groups of the neck, resulting in dramatically less postoperative pain and faster recovery.
- Outpatient procedure: No hospital stay is required. Most patients walk out of the surgical center within one hour.
- Rapid recovery: Most patients return to daily activities within two to three days and to desk work within a week. This contrasts sharply with the three to six month recovery typical of ACDF.
- No opioids required: Patients do not need narcotic pain medication after DLDR, unlike most traditional cervical spine procedures.
- Proven results: Over 20 years and more than 2,000 procedures, DLDR has achieved a 99.6% success rate in eliminating pain with zero complications on record.
What DLDR treats:
- Disc-related cervical spinal stenosis
- Herniated and bulging cervical discs
- Annular tears
- Bone spur-related nerve compression
- Cervical radiculopathy (pinched nerves in the neck)
- Degenerative disc disease
- Chronic neck and arm pain
The appropriate surgical approach, whether DLDR or another technique, is always determined after a thorough review of diagnostic imaging, clinical examination, and an honest assessment of all available options. At Deuk Spine Institute, patients receive a free MRI review so that Dr. Deukmedjian can assess candidacy and provide a genuine, evidence-based recommendation.
Why a Second Opinion on Cervical Spinal Stenosis Treatment Can Change Your Outcome
One of the most important steps any patient with cervical spinal stenosis can take before committing to surgery is to obtain a second opinion from a surgeon trained in both traditional fusion techniques and minimally invasive, motion-preserving alternatives.
Many patients with disc-related cervical stenosis are offered only ACDF because it is the procedure their surgeon performs most frequently, not necessarily because it is the best option for their specific anatomy and diagnosis. As documented in the research on ASD, fusion carries meaningful long-term risks that compound over time, especially for younger patients. A surgeon whose practice includes advanced endoscopic and laser techniques can evaluate whether a motion-preserving approach addresses your specific compression pattern.
At Deuk Spine Institute, we offer a free virtual consultation and MRI review. Dr. Deukmedjian will personally review your imaging and provide an honest, independent assessment of whether Deuk Laser Disc Repair or another approach best fits your condition.
Sources
- https://my.clevelandclinic.org/health/diseases/17499-spinal-stenosis
- https://my.clevelandclinic.org/health/diseases/22564-radiculopathy
- https://pubmed.ncbi.nlm.nih.gov/28723018/
- https://eor.bioscientifica.com/view/journals/eor/10/6/EOR-2025-0070.xml
- https://www.mayoclinic.org/tests-procedures/mri/about/pac-20384768
- https://www.mayoclinic.org/tests-procedures/ct-scan/about/pac-20393675
- https://my.clevelandclinic.org/health/treatments/10874-spinal-decompression-therapy
- https://pmc.ncbi.nlm.nih.gov/articles/PMC11605282/
Frequently Asked Questions
-
What is the difference between cervical spinal stenosis and a cervical herniated disc?
Both conditions can produce similar symptoms including neck pain, radiating arm pain, numbness, and weakness, but they are distinct diagnoses. Cervical spinal stenosis is the narrowing of the spinal canal itself, typically caused by age-related changes including bone spurs, thickened ligaments, and degenerative disc changes. It often affects multiple levels and can compress the spinal cord (myelopathy) in addition to individual nerve roots. A cervical herniated disc is a single event in which the inner material of one disc pushes through a tear in the outer wall and directly compresses a nerve root or the cord. Herniated discs can be sudden or gradual and typically cause radicular pain following a specific nerve path. In practice, these conditions frequently occur together, as disc herniations are one of the most common causes of canal narrowing in cervical stenosis.
-
Can cervical spinal stenosis be treated without surgery?
Yes, mild cases of cervical spinal stenosis without significant or progressive neurological deficits are typically managed initially with conservative care including physical therapy, anti-inflammatory medications, and epidural steroid injections. These treatments can meaningfully reduce pain and improve function. However, conservative treatment does not correct the structural narrowing of the canal. If symptoms are severe, worsening, or accompanied by neurological deficits such as progressive weakness, coordination problems, or myelopathy, surgical decompression is necessary to relieve pressure, prevent permanent nerve damage, and allow neurological recovery. A 2025 review confirmed that earlier surgical intervention in degenerative cervical myelopathy consistently produces better neurological outcomes than delayed treatment.
-
Is traditional cervical fusion (ACDF) the only surgical option for cervical spinal stenosis?
No. While ACDF is the most commonly performed cervical spine surgery in the United States, it is not the only option and is not always the best option. For patients with disc-related cervical stenosis, Deuk Laser Disc Repair offers a minimally invasive, motion-preserving alternative that treats the structural cause of compression without fusing the spine. ACDF permanently eliminates motion at the fused level and transfers biomechanical stress to adjacent segments, with published ASD rates requiring reoperation of approximately 6.57% and ASD incidence as high as 21% in five-year follow-up. Deuk Laser Disc Repair carries none of these long-term structural risks because it does not involve fusion or hardware. The appropriate procedure depends on the specific anatomy and cause of compression, which is why evaluation by a surgeon trained in both approaches is essential.
-
What happens if cervical spinal stenosis is left untreated?
Because cervical spinal stenosis is a progressive condition, leaving it untreated carries a significant risk of worsening neurological damage. Potential consequences include increasing weakness and numbness in the arms and hands, deterioration of fine motor skills, progressive gait instability and balance problems, and in severe cases loss of bladder or bowel control. Prolonged pressure on the spinal cord can cause permanent injury that does not fully recover even with delayed surgery. Research on degenerative cervical myelopathy consistently shows that the severity of neurological deficits at the time of surgery is one of the most important predictors of how fully a patient recovers. For this reason, timely evaluation and treatment are strongly recommended when symptoms suggest significant or progressive cord or nerve root compression.


