

By Dr. Ara Deukmedjian, MD
Board-Certified Neurosurgeon, Deuk Spine Institute
Medically reviewed on April 1, 2026
Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
Key Points
Before diving into the details, here is what you need to know about bone spurs in the spine:
✓ Bone spurs are extremely common with age: According to UPMC, approximately 80% of men and 60% of women over age 50 have bone spurs, and by age 70 the figure rises to 95% across both sexes. Most are asymptomatic.
✓ They are a symptom of a deeper problem, not the problem itself: Bone spurs form because the spine is unstable or degenerating. Addressing the underlying disc degeneration or joint deterioration is the key to lasting relief.
✓ Spinal bone spurs are the most clinically significant: When osteophytes form in the cervical or lumbar spine, they can compress nerve roots and the spinal cord, producing pain, numbness, weakness, and in severe cases, loss of bladder and bowel function.
✓ Imaging is essential for accurate diagnosis: X-rays detect osteophyte formation, but MRI is required to assess nerve and spinal cord compression, and CT scan is used for detailed bony anatomy assessment before surgery.
✓ Conservative treatment manages symptoms but does not remove spurs: Physical therapy, medications, and epidural steroid injections provide meaningful relief but do not resolve the structural osteophyte causing compression.
✓ When surgery is necessary, minimally invasive options outperform open procedures: Deuk Laser Disc Repair® can remove disc-related osteophytes and bone spurs causing nerve compression without fusion, hardware, or extended recovery.
✓ The global burden of osteoarthritis, the leading driver of bone spurs, is increasing: A 2025 systematic review published in Osteoarthritis and Cartilage confirmed a notable rise in early-onset osteoarthritis driven by obesity and joint injuries, making bone spur formation an increasingly prevalent concern across younger age groups.
✓ Prevention is possible: Maintaining a healthy weight, exercising regularly, practicing good posture, and eating a diet rich in calcium and vitamin D all reduce the risk of developing symptomatic spinal bone spurs.
Bone Spurs (Osteophytes): Causes, Symptoms, and Treatment Options
Bone spurs, known medically as osteophytes, are calcified growths of additional bone that form along the edges of vertebrae, joints, and attachment points of ligaments and tendons. 1 In the spine, they are among the most common radiographic findings in adults over the age of 50, and they represent the body’s natural response to mechanical stress, joint deterioration, and structural instability. While many bone spurs never cause any symptoms, those that form in the cervical or lumbar spine can compress nerve roots or the spinal cord, producing pain, numbness, weakness, and other neurological symptoms that significantly affect quality of life.
Understanding what bone spurs are, why they form, how they cause pain, and what treatment options exist is essential for anyone experiencing spine-related symptoms that may have an osteophyte component.
What Are Bone Spurs?
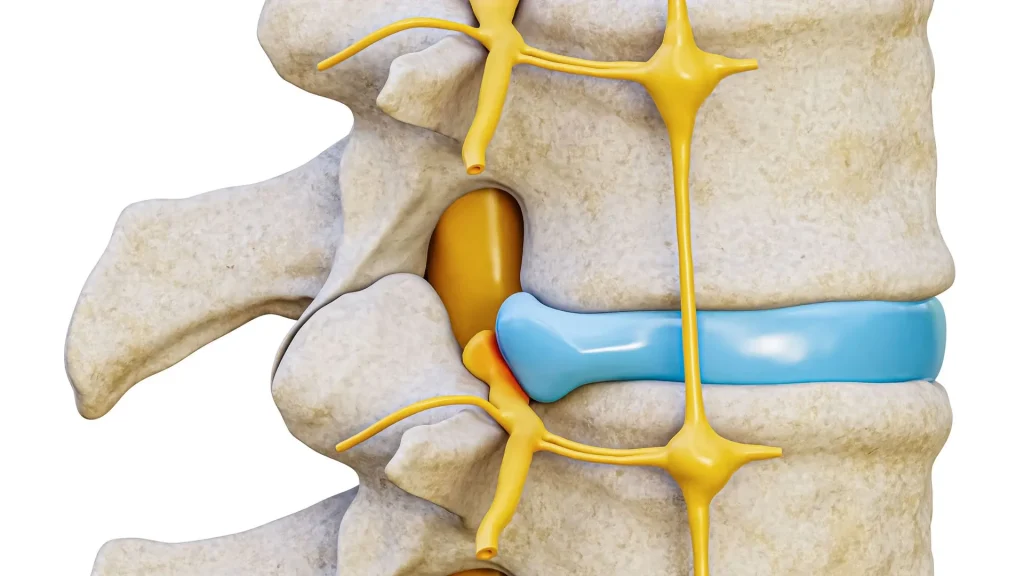
Bone spurs are smooth, hard outgrowths of calcified bone that develop on the ends of bones, typically near joints. Despite their name, they are not sharp spikes but rather rounded projections that develop gradually over months or years. They form wherever bone is under sustained mechanical stress, is damaged, or where adjacent soft tissues including cartilage, ligaments, and tendons become inflamed or injured.
In the spine, osteophytes develop most commonly at two sites: the vertebral body margins, where they are called vertebral osteophytes or spondylophytes, and the facet joints, where they are called facet osteophytes. Both types can encroach on the space available for the spinal cord and exiting nerve roots. According to UPMC, by age 70, approximately 95% of both men and women have bone spurs somewhere in the body. 2 The vast majority of these are never symptomatic, but when bone spurs form within the spinal canal or neural foramen, the consequences can be significant.
Bone spurs themselves are not the root cause of the problem. They are the body’s attempt to compensate for structural instability or damage, essentially a bony scar. Treating bone spurs effectively means understanding and addressing what is driving their formation.
What Causes Bone Spurs in the Spine?
Spinal bone spurs develop as a downstream consequence of several interrelated processes, most of which involve degeneration of the discs and joints of the spine.
Osteoarthritis and Facet Joint Degeneration
Osteoarthritis is the most frequent underlying cause of spinal bone spurs. 3 In the back of the spine, each vertebra connects to those above and below through paired facet joints. These joints are lined with smooth cartilage that allows the surfaces to glide against each other during spinal movement. As osteoarthritis degrades this cartilage over time, the joint surfaces grind directly against each other. 4 The body responds by forming osteophytes at the joint margins in an attempt to redistribute load across the larger surface area created by the new bone. The result is that the facet joints enlarge, and the excess bone can protrude into the spinal canal or neural foramen.
A 2025 systematic review published in Osteoarthritis and Cartilage, covering epidemiological and therapeutic research from April 2024 to March 2025, confirmed that the global burden of osteoarthritis continues to rise, with a notable increase in early-onset OA driven by obesity and joint injuries. 5 This trend means spinal bone spurs are becoming a clinical concern for progressively younger populations.
Degenerative Disc Disease
Degenerative disc disease is the wear-related deterioration of the intervertebral discs, the shock-absorbing cushions between vertebrae. As discs lose hydration and height over time, the vertebrae above and below them move closer together, altering the biomechanics of the entire spinal segment. This generates increased stress on the facet joints, the vertebral endplates, and the surrounding ligaments. In response to this mechanical overload and resulting instability, the body produces osteophytes at the vertebral body margins. 6
A 2024 PMC review of lumbar disc degenerative disease confirmed that signs of disc degeneration, including osteophytes at the vertebral apophyses, are consistently associated with disc height loss and facet joint changes, and that these processes reinforce each other in a progressive degenerative cascade. 7 The most commonly affected lumbar levels are L3-L4 and L4-L5 through L5-S1, while in the cervical spine the C5-C6 level exhibits the earliest and most significant degeneration according to StatPearls. 8

How Enthesophytes Form: The Role of Ligament Instability
A specific subset of spinal bone spurs, known as enthesophytes, form at the attachments of ligaments to vertebral bone. As the intervertebral discs wear out and lose height, the ligaments that connect the vertebrae together become slack and lose their normal tensioning. The body attempts to compensate for this instability by thickening the ligaments and depositing new bone at their attachment points on the vertebra. The enthesis, the junction between the ligament and the bone, becomes inflamed from this process. Vertebral bone cells deposit new mineral at this inflamed junction, and the enthesis tissue calcifies into a bone spur.
A 2024 PMC study examining traction spurs in the lumbar spine documented that traction osteophytes form as a direct response to spinal instability, and that their presence on imaging has high specificity for identifying unstable segments in the lumbar spine. 9
Additional Contributing Factors
Several other factors can accelerate or contribute to spinal bone spur formation:
Age: The risk of developing bone spurs increases significantly with age as the cumulative effects of joint use and degeneration accumulate. Most patients with symptomatic spinal stenosis from bone spurs are in their 60s and 70s.

Obesity: Excess body weight places sustained additional compressive loading on the intervertebral discs and facet joints, accelerating the degenerative processes that lead to osteophyte formation. The 2025 Osteoarthritis and Cartilage systematic review specifically identified obesity as a key driver of early-onset OA.
Occupational and physical demands: Workers in physically demanding roles involving heavy lifting, repetitive bending, or prolonged vibration exposure, including construction workers, warehouse staff, and truck drivers, develop spinal degeneration and associated bone spurs at earlier ages than sedentary individuals.

Poor posture: Sustained poor posture alters the distribution of mechanical forces through the spinal segments, creating areas of concentrated stress that accelerate local degeneration and osteophyte formation.
Spinal deformity: Structural conditions including scoliosis, kyphosis, and spondylolisthesis alter load distribution through the spine, accelerating degeneration and bone spur formation at specific levels.
Genetics: Genetic predisposition plays a role in both disc health and joint cartilage maintenance, meaning some individuals are at elevated risk regardless of lifestyle or occupation.
Who Is at Risk of Developing Spinal Bone Spurs?
Spinal bone spurs are primarily a consequence of aging, meaning that risk increases with every decade of life. They are a near-universal imaging finding in people over age 70. Beyond age, individuals with the following characteristics are at elevated risk:
- Personal or family history of osteoarthritis
- Obesity or overweight
- History of spinal injury or repetitive spinal loading at work
- Sedentary lifestyle combined with metabolic health issues
- Scoliosis, kyphosis, or other structural spinal conditions
- History of chronic poor posture
It is important to note that imaging evidence of bone spurs does not always correlate with symptoms. Many people with extensive osteophyte formation on X-ray or MRI have no pain or neurological symptoms whatsoever. The clinical significance depends on whether the osteophytes are impinging on neural structures.
How Bone Spurs Cause Pain
Bone spurs themselves do not generate pain directly. Pain arises when osteophytes encroach on adjacent structures in three main ways. 10
Nerve Root Compression (Radiculopathy)
The neural foramen are the openings on each side of the spine through which nerve roots exit the spinal canal and travel to the arms and legs. Bone spurs that form at the vertebral margins or facet joints can narrow these openings, compressing the exiting nerve root. This compression produces radiculopathy: radiating pain, tingling, numbness, and weakness following the distribution of the affected nerve. In the cervical spine this manifests as symptoms traveling into the shoulder, arm, and hand. In the lumbar spine it produces low back pain and sciatica radiating into the buttock, leg, and foot.
Research from 2024 confirmed that nerve irritation from spinal bone spurs involves both mechanical compression and a chemical inflammatory component, as the inflammatory mediators released during osteophyte formation can sensitize nearby nerves even without direct physical pressure.
Spinal Cord Compression (Myelopathy)
Bone spurs that grow into the spinal canal itself can compress the spinal cord, producing cervical or thoracic myelopathy. Unlike radiculopathy, which typically affects one limb following a specific nerve pattern, myelopathy produces more diffuse symptoms including bilateral arm or leg weakness, loss of fine motor control, balance and coordination difficulties, and in advanced cases, loss of bladder or bowel function. Cervical myelopathy from osteophyte-driven stenosis is one of the most common causes of spinal cord dysfunction in adults over 55 and requires prompt evaluation to prevent permanent neurological injury.
Facet Joint Inflammation
Osteophytes within the facet joints cause the joint surfaces to grind against each other during spinal movement, producing friction, synovial inflammation, and local pain. Facet-mediated pain is typically axial, meaning it is felt primarily in the back or neck itself rather than radiating into the extremities, and it worsens with extension and rotation of the spine.

Symptoms of Spinal Bone Spurs
Symptoms vary substantially depending on the location of the osteophytes and which structures they are compressing.
Cervical Spine (Neck) Bone Spur Symptoms
- Neck pain or stiffness that worsens with certain movements
- Numbness, tingling, or a pins-and-needles sensation in one or both arms
- Radiating pain from the neck into the shoulder, arm, or hand (cervical radiculopathy)
- Weakness in the upper arms or hands, affecting grip strength or fine motor skills
- In more severe cases: bilateral arm or leg symptoms, gait problems, or loss of bladder control indicating myelopathy
- Rarely: difficulty swallowing (dysphagia) if cervical osteophytes grow large enough to impinge on the esophagus
Lumbar Spine (Lower Back) Bone Spur Symptoms
- Dull, aching lower back pain that worsens with prolonged standing or walking
- Radiating pain into the buttock, thigh, leg, or foot (sciatica)
- Loss of sensation or tingling in the buttocks, thighs, or legs
- Weakness in one or both legs, making activities like climbing stairs more difficult
- Neurogenic claudication: leg pain and weakness that develops with walking and relieves with sitting or forward flexion, a hallmark of lumbar spinal stenosis from bone spurs
Diagnosing Spinal Bone Spurs
Accurately diagnosing bone spurs and their clinical impact requires a combination of clinical evaluation and advanced imaging.
Physical and Neurological Examination
A comprehensive examination evaluates the range of motion of the affected spinal region, reflex responses, motor strength in the extremities, sensation, and balance. Provocative maneuvers such as the Spurling test for cervical radiculopathy and the straight leg raise for lumbar radiculopathy help identify nerve root involvement. The pattern of neurological deficits identified on examination guides the selection of imaging studies. 11
X-Ray
X-rays are the most accessible initial imaging tool for bone spur evaluation. They clearly show osteophyte formation at vertebral margins, disc space narrowing, and facet joint hypertrophy. X-rays are used as the first step to assess the extent of bony degeneration and determine whether more detailed imaging is needed.

MRI: The Gold Standard
MRI provides the most complete picture of spinal bone spur impact. It visualizes not only the osteophytes themselves but also the degree of neural foramen narrowing, the extent of spinal cord or nerve root compression, and the condition of the surrounding discs, ligaments, and soft tissues. MRI is essential for surgical planning and for correlating imaging findings with the patient’s specific symptoms.
CT Scan
CT scanning provides superior detail for bony anatomy compared to MRI and is particularly useful for characterizing the size, shape, and precise location of bone spurs before surgery. CT myelography, which involves injecting contrast into the spinal fluid, provides even more detailed visualization of nerve root and cord compression in complex cases.
Non-Surgical Treatment for Bone Spurs
For the majority of patients with mild to moderate symptoms from spinal bone spurs, conservative management provides meaningful relief. It is important to understand clearly that conservative treatment manages symptoms but does not physically remove or reduce osteophytes. 12
Medications
Over-the-counter non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen reduce both pain and the inflammation associated with nerve compression and facet joint irritation. For more severe pain, prescription nerve medications including gabapentinoids can address neuropathic components of bone spur-related radiculopathy. Short courses of oral corticosteroids may provide additional relief during acute flares. Long-term use of any medication should be supervised by a physician given the potential for side effects.

Physical Therapy
A structured physical therapy program is one of the most effective conservative interventions for symptomatic spinal bone spurs. Therapy focuses on strengthening the muscles that support the spine, reducing the mechanical load on degenerating joints, improving flexibility and range of motion, and correcting posture that exacerbates symptoms. A 2025 review in Current Treatment Options in Rheumatology confirmed that physical therapy and orthosis immobilization improve pain and stiffness associated with spinal ligament calcification and enthesophyte formation. 13

Epidural Steroid Injections
Epidural steroid injections deliver anti-inflammatory corticosteroids directly to the area of nerve compression adjacent to the bone spur. They can provide temporary but significant reductions in radicular pain, allowing patients to participate more effectively in physical therapy. Their effects are not permanent and do not address the structural osteophyte, but they are a valuable component of multimodal conservative care.
Activity Modification
Avoiding activities that consistently aggravate bone spur symptoms, and incorporating ergonomic improvements into daily activities, can reduce the frequency and severity of flares. Walking aids, ergonomic workstations, and supportive sleeping positions are all practical tools for symptom management.
Surgical Treatment for Bone Spurs
When conservative management fails to provide adequate relief, when neurological deficits are progressing, or when spinal cord compression from osteophytes requires urgent decompression, surgery becomes necessary. The goal of surgery is decompression: physically removing the bone spur and any associated disc material that is compressing the nerve root or spinal cord.
The approach chosen matters significantly for both outcomes and recovery.
Deuk Laser Disc Repair®: Advanced Treatment for Disc-Related Bone Spurs
For bone spurs that are associated with or arise from disc-level degeneration, including anterior osteophytes, posterior disc-osteophyte complexes, and foraminal bone spurs compressing nerve roots, Deuk Laser Disc Repair® (DLDR) offers the most advanced minimally invasive treatment available. 14 The procedure treats both the damaged disc tissue driving osteophyte formation and the compressive osteophyte itself, without fusion, without hardware, and without the structural disruption of open surgery.
How it works: DLDR is performed through a 4 to 7 mm incision using a high-definition endoscopic camera and a precision Holmium:YAG laser. The laser removes the damaged disc tissue, bone spur material, and inflamed annular tissue causing nerve compression, while leaving healthy structures intact. Bones, muscles, and stabilizing joints are not disrupted.
Key advantages:
- No fusion: The spine maintains its natural motion permanently, with no risk of adjacent segment disease
- No hardware: No screws, rods, or cages
- Outpatient procedure: No hospital stay, walk out within one hour
- Rapid recovery: Return to daily activities in two to three days, desk work within a week
- No opioids: No narcotic pain medication required after the procedure
- Proven results: 99.6% success rate across more than 2,000 procedures with zero complications over 20 years
Traditional Surgical Options
For more extensive or complex spinal bone spur presentations, traditional surgical approaches may be required.
Laminectomy: Removes the lamina to decompress the spinal cord and nerve roots. Frequently combined with fusion due to the instability created by bone removal. Recovery takes 2 to 6 months.
Foraminotomy: Widens the neural foramen to relieve nerve root compression. May be performed as a standalone procedure or in combination with discectomy. Less structurally disruptive than laminectomy when performed in isolation.
Spinal fusion (ACDF or TLIF): Appropriate when bone spur formation is associated with significant spinal instability that requires structural correction. Permanently eliminates motion at the fused level and carries a well-documented risk of adjacent segment disease at neighboring levels. Recovery takes 6 to 12 months.
Preventing Bone Spurs
While bone spurs caused by the natural aging process cannot always be prevented entirely, there are meaningful steps that reduce the risk and slow the progression of the underlying conditions that cause them.
- Maintain a healthy weight: Reducing excess body weight decreases the mechanical load on spinal discs and facet joints, directly slowing degenerative processes.
- Exercise regularly: Weight-bearing exercise strengthens the muscles that support the spine, reduces joint stress, and improves disc nutrition through movement-driven fluid exchange.
- Practice good posture: Correct posture when sitting, standing, and lifting distributes spinal load evenly across all segments rather than concentrating stress at specific levels.
- Adopt a bone-healthy diet: Adequate calcium and vitamin D intake supports bone density and reduces the risk of the osteoporotic changes that accelerate spinal degeneration.
- Use proper lifting mechanics: Lifting with the legs, keeping objects close to the body, and avoiding spinal flexion under load prevents the acute disc injuries that initiate the degenerative cascade leading to osteophytes.
- Consider physical therapy proactively: Learning correct body mechanics and maintaining a strong posterior chain can significantly delay the onset of symptomatic degenerative changes.
Frequently Asked Questions
-
Q1: Are bone spurs always painful?
A1: No. The majority of spinal bone spurs never cause any symptoms. While approximately 80% of people over 50 and 95% of people over 70 have bone spurs, most learn about them incidentally during imaging done for another reason. Pain and neurological symptoms only develop when osteophytes grow into the spinal canal or neural foramen and compress a nerve root or the spinal cord.
-
Q2: Can bone spurs in the spine be removed without surgery?
A2: No. Once formed, bone spurs are structural calcified growths that can only be physically removed through surgical intervention. Conservative treatments including medications, physical therapy, and epidural steroid injections can significantly reduce the pain and inflammation caused by bone spurs, but they do not dissolve or reduce the osteophyte itself.
-
Q3: What is the connection between bone spurs and herniated discs?
A3: Bone spurs and herniated discs frequently coexist because both are products of the same underlying degenerative process. As an intervertebral disc degenerates, it loses height and structural integrity, leading simultaneously to disc bulging or herniation and to vertebral instability that triggers bone spur formation at the adjacent vertebral margins.
-
Q4: When should I see a doctor about possible bone spurs?
A4: You should seek evaluation from a spine specialist if you experience persistent neck or back pain lasting more than four to six weeks that does not improve with rest, if you develop radiating pain, numbness, or tingling into the arms or legs, if you notice progressive weakness, if you have balance problems, or if you experience any loss of bladder or bowel control, which is a medical emergency requiring immediate evaluation.


