

By Dr. Ara Deukmedjian
Board-Certified Neurosurgeon, Deuk Spine Institute
Medically reviewed on April 29, 2026
Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
Key Points
✓ Spinal fusion permanently locks vertebrae together with screws, rods, and cages and over 90% of fusion patients require additional surgery in their lifetime; due to Adjacent Segment Disease (ASD).
✓ Alternatives to spinal fusion preserve motion, avoid hardware, and treat the actual source of pain rather than eliminating movement at the painful disc level.
✓ The right alternative depends on the diagnosis: herniated disc, spinal stenosis, degenerative disc disease, spondylolisthesis, and scoliosis each have different options.
✓ Deuk Laser Disc Repair® treats the most common reasons fusion is recommended (disc herniation, annular tears, discogenic pain) through a 4mm to 7mm incision, with a 99% pain elimination rate and a 0.01% complication rate.
Why Patients Are Looking for Alternatives
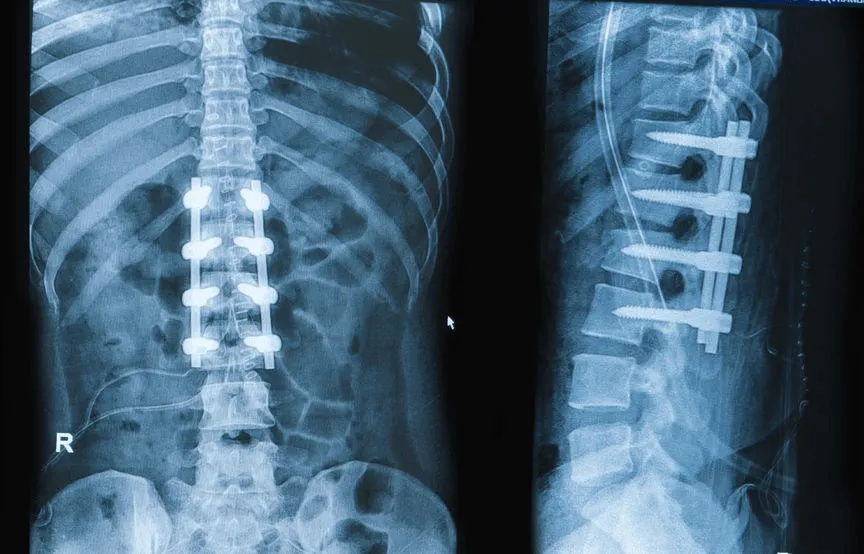
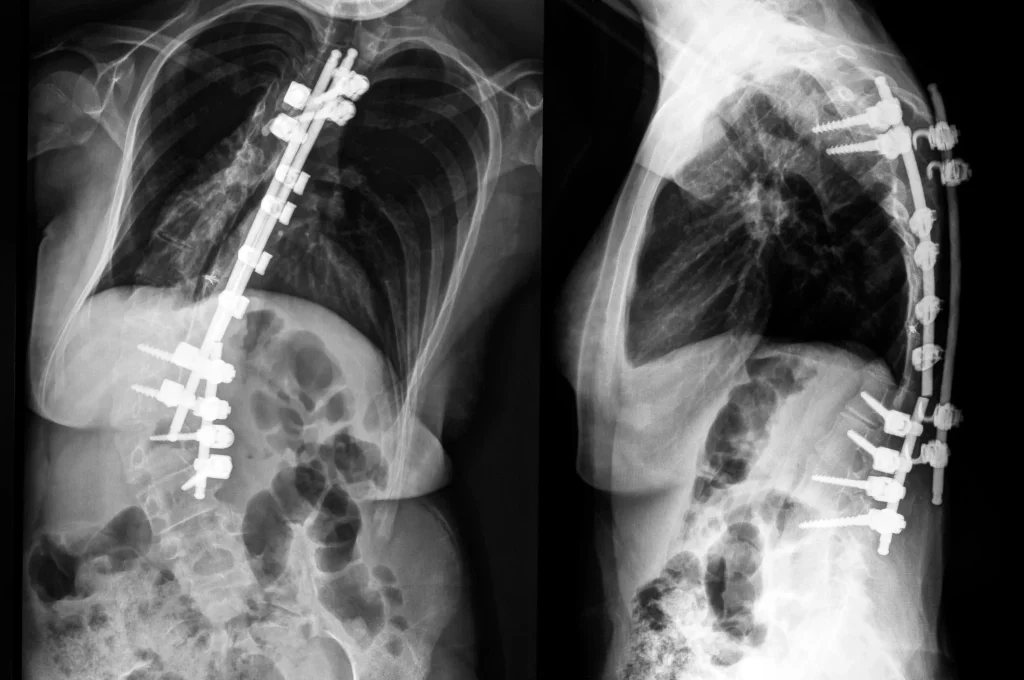
Spinal fusion is one of the most invasive procedures in modern spine surgery. It uses a 3 to 8 inch incision, removes muscle and bone, eliminates the disc, and bolts vertebrae together with metal hardware. Once the spine is fused, it never moves at that level again.
The result is a cascade of long-term consequences: adjacent segment disease, hardware failure, chronic pain, and the well-documented statistic that more than 90% of fusion patients eventually need additional spine surgery.¹ The full picture of what can go wrong after fusion, from hardware failure and infection to adjacent segment disease and chronic pain syndrome, is covered in detail for patients who want to understand the risks before making a decision about spinal fusion complications.
That is why “alternatives to spinal fusion” has become one of the most-searched phrases by patients facing a fusion recommendation.
The good news is that for the vast majority of patients don’t need to get a highly invasive spine surgery like fusion.
What Spinal Fusion Actually Does (And Why That Matters)
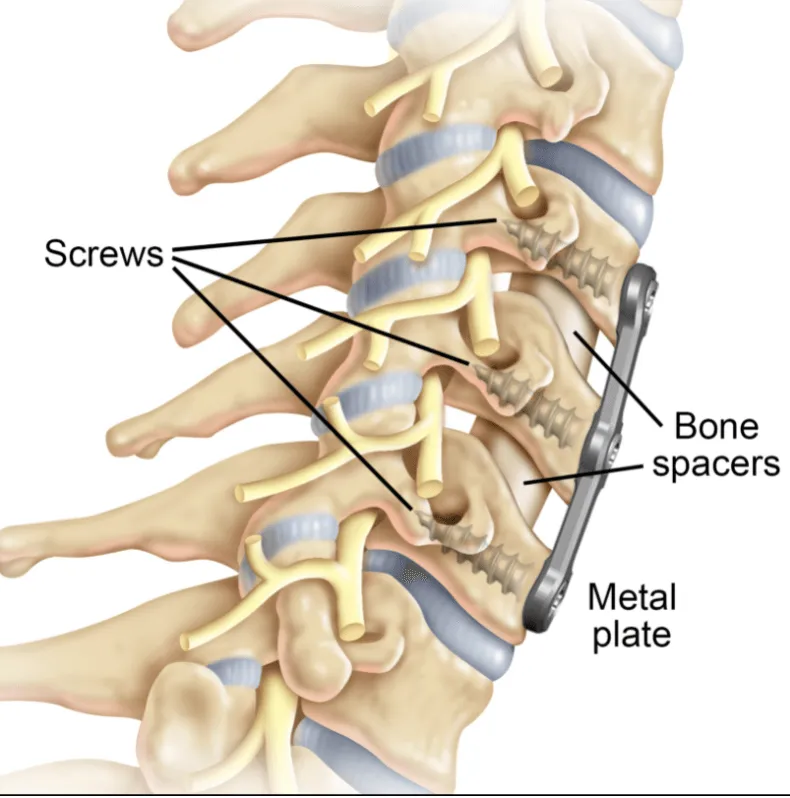
Fusion does not repair the painful disc. It removes the disc entirely, replaces it with a metal-plastic cage filled with bone graft, and locks the vertebrae above and below together with pedicle screws, rods, or plates.
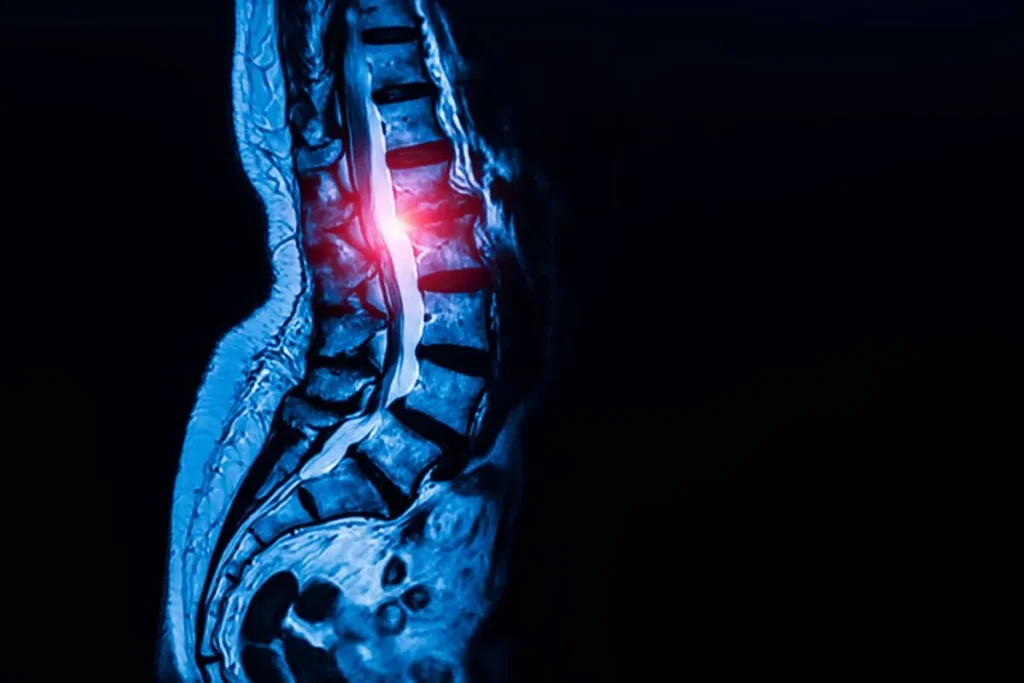
That distinction matters because the structures responsible for back and neck pain; the inflamed annular tear, the herniated nucleus pulposus, the irritated nerve root. Are not “fixed” by spine fusion surgery. They are bypassed. Once motion is eliminated, the body is forced to compensate at the levels above and below, accelerating degeneration there.²
A genuine alternative to fusion does the opposite: it treats the actual pain generator while preserving the disc, the bone, the muscles, and the natural motion of the spine.
DLDR® The Alternative to Spinal Fusion Surgery
There are six categories of alternatives to fusion that patients should understand before signing a consent form:
- Endoscopic laser disc repair (Deuk Laser Disc Repair®)
- Artificial disc replacement (cervical and lumbar arthroplasty)
- Endoscopic decompression for stenosis
- Plasma rhizotomy for facet-mediated pain (Deuk Plasma Rhizotomy®)
- Microdiscectomy (still invasive, but motion-preserving)
- Conservative care (physical therapy, medication, injections)
Each one targets a different pain generator. The right choice depends entirely on what is actually causing the pain. Which is why an accurate diagnosis from an MRI is more important than any specific procedure.
Alternatives to Spinal Fusion for Spinal Stenosis
Spinal stenosis is narrowing of the spinal canal, typically from a combination of disc bulging, ligament thickening, and bone spurs. Fusion is frequently recommended for stenosis even when the underlying cause is something far more treatable.
Better alternatives for stenosis include:
- Endoscopic decompression — uses a small portal to remove the specific tissue compressing the nerve, without destabilizing the spine. No fusion required because the bones, ligaments, and facet joints stay intact.
- Deuk Laser Disc Repair® — when the stenosis is driven by a bulging or herniated disc (which is common at L4-L5), removing the disc material alone often resolves the symptoms. There is no reason to fuse a spine when the disc is the problem.
- Interspinous spacers — small implants placed between vertebrae to open the canal in mild to moderate cases.
Fusion is rarely necessary for stenosis. The exceptions are cases of true segmental instability or severe deformity, which represent a small minority of stenosis patients.
Alternatives to Spinal Fusion for Degenerative Disc Disease
Degenerative disc disease (DDD) is the most over diagnosed reason for fusion. The term simply means a disc has dried out, lost height, and developed annular tears. Nearly every adult develops disc problems with age.
The pain in DDD comes from inflamed nerve endings inside the annular tear, not from the wear itself. That is exactly the problem laser disc repair is designed to treat:
- Deuk Laser Disc Repair® vaporizes the inflamed tissue inside the annular tear, removes any displaced disc material, and debrides damaged fibers so the tear can heal naturally. The disc is preserved, disc height is preserved, and motion is preserved.
- Artificial disc replacement is also a motion-preserving alternative for DDD, particularly in the cervical spine. Long-term studies show cervical disc arthroplasty produces equivalent or better pain relief than ACDF, with significantly lower rates of reoperation and adjacent segment disease.⁵
- Regenerative therapies (PRP, stem cell injections) are sometimes proposed but lack the consistent peer-reviewed outcomes of established surgical alternatives.
A diagnosis of “degenerative disc disease” almost never requires fusion. It requires identifying which disc is actually painful and treating that specific disc.
Alternatives to Spinal Fusion for Spondylolisthesis
Spondylolisthesis is the forward slippage of one vertebra over another, most commonly at L4-L5 or L5-S1. Many surgeons recommend fusion for any degree of slippage. Only severe cases of slippage will require a spinal fusion.
Modern alternatives depend on the grade and stability of the slip:
- Low-grade, stable spondylolisthesis (Grade 1): the slip itself is rarely the pain source. The actual pain usually comes from a herniated or torn disc, or from arthritic facet joints, at the same level. Treating the disc with Deuk Laser Disc Repair® or the facets with Deuk Plasma Rhizotomy® often eliminates symptoms without ever touching the alignment.
- Moderate slips with mechanical instability: endoscopic decompression with motion-preserving stabilization can be appropriate without committing to a full fusion.
- High-grade slips (Grade 3 or higher): these are the rare cases where fusion may be required.
Most spondylolisthesis patients are Grade 1, and most do not need fusion. They need an accurate diagnosis of what is actually generating their pain.
Alternatives to Spinal Fusion for Scoliosis
Scoliosis surgery has historically meant long-segment fusion with rods and screws; sometimes 10 or more vertebrae welded together permanently. For adult degenerative scoliosis, that approach is increasingly being challenged.
Alternatives for adult scoliosis include:
- Targeted decompression: of the specific level causing pain, leaving the rest of the curve untouched. Many adults with scoliosis have pain from a single segment, not the curve itself.
- Deuk Laser Disc Repair®: when the pain generator is a specific symptomatic disc within the curve.
- Deuk Plasma Rhizotomy®: for facet pain, which is common in degenerative scoliosis.
- Bracing and physical therapy for adolescent idiopathic scoliosis under appropriate degree thresholds.
Multi-level fusion for scoliosis carries enormous risk: blood loss, hardware complications, proximal junctional kyphosis, and lengthy recovery. Patients should pursue every motion-preserving alternative first.
Alternatives to Spinal Fusion at L4-L5
L4-L5 is the most common level in the spine where fusion is recommended and the most common level where it is not actually necessary.
The pain at L4-L5 typically comes from:
- A herniated or bulging disc compressing the L5 nerve root
- An annular tear with discogenic low back pain
- Facet joint arthritis
- Foraminal stenosis from disc collapse
Each of these can be treated without fusion:
- Disc herniation or annular tear at L4-L5 — Deuk Laser Disc Repair® removes the herniated material and debrides the tear through a 4mm to 7mm incision. The disc is preserved.³
- Facet pain at L4-L5 — Deuk Plasma Rhizotomy® permanently denervates the medial branch nerve carrying pain signals from the facet joint.
- Foraminal stenosis at L4-L5 — endoscopic decompression opens the foramen without removing the lamina or facet joint.
Patients told they need an L4-L5 fusion should have their MRI reviewed by a surgeon who actually performs minimally invasive alternatives — not just a fusion specialist who will see every problem as a fusion candidate.
Alternatives to Spinal Fusion at L5-S1
L5-S1 is the bottom disc in the lumbar spine and the second most common fusion level. It carries the highest mechanical load in the back, which is why it tears, herniates, and degenerates frequently.
Alternatives at L5-S1 mirror those at L4-L5, with one important consideration: anterior approaches to L5-S1 fusion (ALIF) carry the highest complication rate of any spine surgery, including major vascular injury and retrograde ejaculation in male patients.⁶
For most patients with L5-S1 pain:
- Deuk Laser Disc Repair® treats herniated and torn L5-S1 discs without disturbing the abdominal vessels, the nerve roots, or the sacrum.
- Lumbar artificial disc replacement is FDA-approved for one- and two-level disease and preserves segmental motion at L5-S1.⁵
- Endoscopic foraminoplasty addresses S1 nerve root compression caused by foraminal narrowing.
If a surgeon recommends an L5-S1 fusion, ask why a motion-preserving option is not appropriate first. The answer should be specific and based on the MRI; not a general statement about how “fusion is the gold standard.”
Alternatives to Lumbar Fusion (All Levels)
Lumbar fusion in the United States costs $80,000 to $150,000, requires 3 to 5 days in the hospital, and involves a 6 to 12 month recovery with mandatory opioid prescriptions.¹ The alternatives are dramatically less invasive:
The decision between fusion and a motion-preserving alternative is not a cosmetic one. It is the difference between a permanent biomechanical change to the spine and a targeted repair of the actual injury.
How to Know Which Alternative Is Right for You
The right alternative is determined by what is actually generating your pain. That requires a careful review of your MRI by a surgeon who performs more than just fusion. Questions to ask:

- What specific structure on my MRI is causing my pain?
- Why is fusion being recommended over a motion-preserving alternative?
- What is the surgeon’s experience with endoscopic and laser alternatives?
- What are the documented complication and reoperation rates for each option?
- Is there peer-reviewed outcome data for the recommended procedure?
If your surgeon cannot answer these questions specifically, get a second opinion before consenting to fusion. Hardware cannot be undone.
Submit your MRI for a free virtual consultation with Dr. Deukmedjian. He will review your imaging and explain whether you are a candidate for a minimally invasive alternative to spinal fusion.
When Spinal Fusion May Still Be Necessary
When a fusion may be necessary
- Unstable spinal fractures
- High-grade spondylolisthesis (Grade 3 or higher)
- Severe spinal deformity requiring correction
- Tumor or infection requiring extensive bone removal
- Failed prior surgeries with documented mechanical instability
These cases represent a small fraction of the fusions actually performed in the United States each year. The overwhelming majority of fusions are recommended for conditions: disc herniation, mild stenosis, degenerative disc disease, low-grade spondylolisthesis are far less invasive alternatives.
Frequently Asked Questions
What are the alternatives to spinal fusion surgery?
The main alternatives include endoscopic laser disc repair, artificial disc replacement, endoscopic decompression, plasma rhizotomy for facet pain, microdiscectomy, and non-surgical conservative care. The right alternative depends on the specific pain generator identified on MRI.
What are the alternatives to spinal fusion for spinal stenosis?
Endoscopic decompression, Deuk Laser Disc Repair® when the stenosis is driven by a disc, and interspinous spacers in mild cases. Fusion is rarely necessary for stenosis unless there is true segmental instability.
What are the alternatives to spinal fusion for degenerative disc disease?
Deuk Laser Disc Repair® is the most direct alternative because it treats the inflamed annular tear that causes discogenic pain. Artificial disc replacement is another motion-preserving option, particularly in the cervical spine.
What are the alternatives to spinal fusion for spondylolisthesis?
For Grade 1 (low-grade) slips, the pain usually comes from a herniated disc or arthritic facets at the same level — both treatable without fusion. Endoscopic decompression and motion-preserving stabilization can address moderate slips. Only high-grade slips typically require fusion.
What are the alternatives to spinal fusion for scoliosis?
Targeted decompression of the painful segment, Deuk Laser Disc Repair® for symptomatic discs within the curve, and Deuk Plasma Rhizotomy® for facet pain. Multi-level fusion should be reserved for severe progressive deformity.
What are the alternatives to spinal fusion at L4-L5?
For herniated or torn discs at L4-L5, Deuk Laser Disc Repair® removes the painful tissue without fusion. For facet pain, Deuk Plasma Rhizotomy® provides permanent relief. Endoscopic decompression addresses foraminal stenosis at this level.
What is the alternative to spinal fusion at L5-S1?
Deuk Laser Disc Repair®, lumbar artificial disc replacement, and endoscopic foraminoplasty are all motion-preserving options for L5-S1. These avoid the high complication rate of anterior lumbar fusion (ALIF) at the lumbosacral junction.
What are the alternatives to lumbar fusion?
The leading minimally invasive alternative is Deuk Laser Disc Repair®, which uses a 4mm to 7mm incision, requires no hardware, is performed outpatient under light sedation, and has a 99% pain elimination rate with a 0.01% complication rate across more than 2,700 procedures.⁴
Is laser spine surgery a real alternative to fusion?
Yes — when performed as true endoscopic laser disc repair, with the laser actually entering the disc through a small portal. Many clinics advertise “laser spine surgery” but only use a laser for the skin incision. Patients should ask whether the laser actually treats the disc itself.
Sources
- A systematic review of treatment guidelines for lumbar disc herniation. Neurospine. 2025;22(2):389-402.
- Adjacent segment disease after lumbar fusion: incidence, risk factors, and management. European Spine Journal. 2024.
- Full-endoscopic versus microscopic lumbar discectomy for lumbar disc herniation: a systematic review and meta-analysis. European Spine Journal. 2024.
- Deukmedjian AR, et al. Deuk Laser Disc Repair® for cervical disc disease: a prospective clinical study.
- Investigational Research: Timeline, Trials, and Future Directions of Spinal Disc Arthroplasty. NCBI.
- Up to 10-year surveillance comparison of survivability in single-level cervical disc replacement versus anterior cervical discectomy and fusion. Journal of Neurosurgery: Spine.


