


This article is for educational purposes only and does not constitute medical advice. Consult a qualified spine specialist before making any treatment decisions.
If you have been recommended for spinal fusion, you have already done the hard part: you found a spine surgeon willing to take your pain seriously. What often happens next is where the problem begins. You leave that appointment with a surgery date, a packet of pre-operative instructions, and one critical question left unasked: Does fusion actually fix what is causing my pain?
After over 30 years of performing spine surgery and developing the Deuk Laser Disc Repair®, I have evaluated thousands of patients who were scheduled for fusion when alternatives to spinal fusion surgery would have addressed their pain source directly. The most common reason this mismatch happens is straightforward: fusion is a structural solution, and most chronic back pain is not a structural problem. It is an inflammatory one.
Understanding that distinction is the most important thing you can do before agreeing to any spinal fusion surgery.
Why Fusion Does Not Fix the Most Common Cause of Back Pain
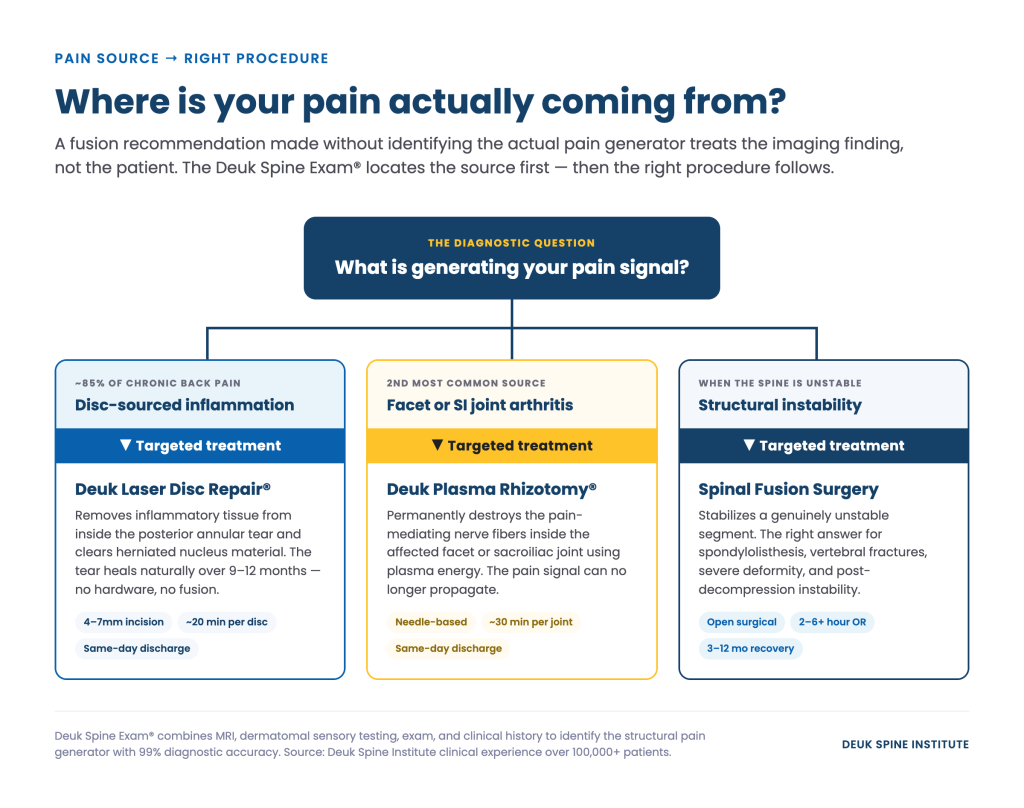
Based on clinical experience with over 100,000 patients, disc injuries account for approximately 85% of chronic back pain. The specific mechanism is this: when the outer wall of a disc (the annulus fibrosus) tears, nucleus pulposus material can herniate into that tear. The result is sustained inflammation within the posterior annular tear, which triggers neoinnervation, the growth of pain nerve fibers into the damaged tissue. That inflammation is what generates the pain signal.
Spinal fusion does not treat this. It eliminates motion at the affected vertebral segment by permanently joining two or more vertebrae into a single unit. Motion at that level is redistributed to the segments above and below. The posterior annular tear, along with its inflammation, remains entirely untreated.
For patients whose pain originates from disc-sourced inflammation, fusion stabilizes a joint that was not the problem. The annular tear continues to generate pain after surgery. This is one documented mechanism behind Failed Back Surgery Syndrome, a condition affecting a meaningful percentage of fusion patients who report ongoing pain after an anatomically successful procedure.
Spinal Fusion Alternatives for Disc-Sourced Pain
The appropriate alternative to fusion depends on what is actually generating the pain signal. That requires an accurate diagnosis before any surgical recommendation is made. The Deuk Spine Exam® combines MRI findings, physical examination, and clinical history to identify the structural source of pain with 99% diagnostic accuracy. Without that step, any surgical recommendation, including fusion, is premature.
For the two most common causes of chronic back pain, the motion-preserving approaches available at Deuk Spine Institute are as follows.
Deuk Laser Disc Repair® for Disc-Sourced Pain
The Deuk Laser Disc Repair® targets the posterior annular tear directly. The procedure removes inflammatory tissue from within the tear, performs debridement of the damaged area, and eliminates the herniated nucleus pulposus material contributing to inflammation. With the inflammatory source removed, the tear heals naturally over the following 9 to 12 months without cadaver bone, metal hardware, or plastic implants placed in the spine.
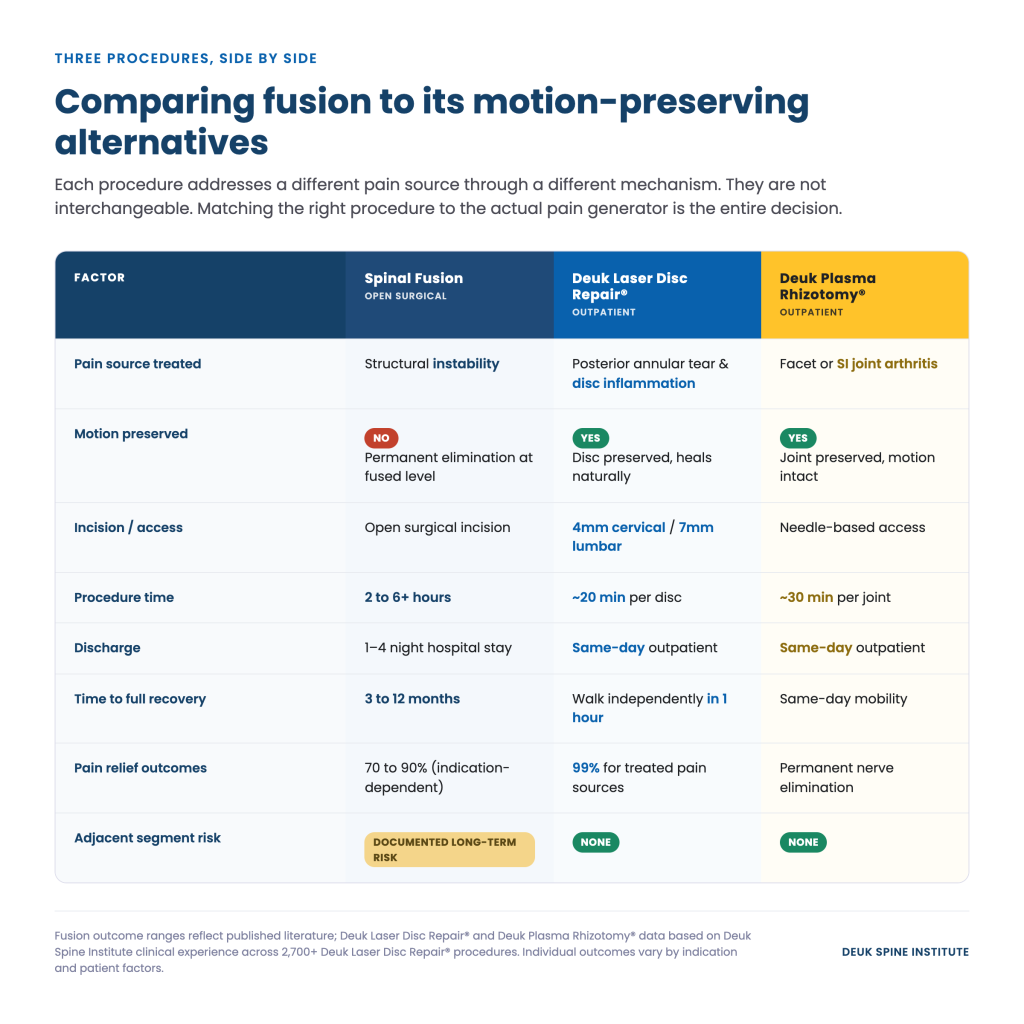
- Incision size: 4mm (cervical) or 7mm (lumbar), smaller than a dime
- Procedure duration: Approximately 20 minutes per disc level
- Discharge: Same-day outpatient, no hospital stay
- Mobility post-procedure: Patients walk independently within one hour
- Pain relief: Patients report an average of 99% pain relief for treated pain sources
- Complication rate: 0.01%
- Infection rate: 0%
- Procedures performed: Over 2,700 Deuk Laser Disc Repair® procedures through 2025
That outcome data reflects over 30 years of clinical practice focused exclusively on identifying and treating the structural source of pain rather than managing symptoms or eliminating motion at a healthy joint.
Contrast that with spinal fusion recovery: three to twelve months of activity restriction, a formal physical therapy program beginning once imaging confirms early bone consolidation, and permanent loss of motion at the treated level. The procedures are not equivalent alternatives. They address different problems through fundamentally different mechanisms.
Deuk Plasma Rhizotomy® for Facet Joint Pain
Not all chronic back pain originates from disc injuries. The second most common source is facet joint arthritis, the small weight-bearing joints located behind each disc. When injury causes a tear in the facet joint capsule, chronic inflammation follows. Anti-inflammatory injections provide temporary relief, but they do not address the pain-generating nerves inside the joint.
The Deuk Plasma Rhizotomy® permanently destroys the pain-mediating nerve fibers inside the affected facet joint or sacroiliac joint using plasma energy. With those nerves eliminated, the pain signal cannot propagate. The procedure takes approximately 30 minutes per joint, is performed on an outpatient basis, and requires no fusion of any vertebral segment.
For patients whose pain source is facet-driven rather than disc-driven, this procedure eliminates the reason fusion was being considered without removing any of the motion that fusion would have permanently eliminated.
Fusion Still Has a Role in Specific Clinical Conditions
I want to be direct about something: I perform spinal fusion. There are clinical conditions where fusion is the medically appropriate answer, and in those cases, recommending fusion is the right call. The argument here is not against fusion as a procedure. It is against fusion as a default recommendation for patients whose pain source never required it.
The conditions where fusion addresses an actual structural problem include:
- High-grade spondylolisthesis: When vertebral slippage creates genuine instability that cannot resolve without structural stabilization
- Vertebral fractures: Traumatic or compression fractures that compromise spinal integrity and require surgical fixation
- Severe spinal deformity: Scoliosis or kyphosis with progressive curvature causing neurological deterioration
- Post-decompression instability: When decompression surgery has removed structural elements and the segment requires stabilization
- Tumors or infections: Pathological compromise of vertebral integrity requiring stabilization after treatment
In each of these cases, fusion resolves something that motion-preserving procedures cannot: a genuinely unstable vertebral segment. The clinical distinction that matters is whether structural instability is present. If it is, fusion addresses it. If it is not, and the pain originates from disc inflammation or facet arthritis, the rationale for fusion weakens considerably.
Why Patients Are Recommended for Fusion When Alternatives Exist
The answer is not that surgeons are acting in bad faith. It is that the diagnostic process often fails to distinguish between pain caused by structural instability and pain caused by disc inflammation. Without that distinction clearly established, fusion appears to address what imaging shows, which is disc degeneration, herniation, or joint changes, without confirming whether those findings are actually the source of the pain signal.
The Deuk Spine Exam® was developed specifically to close that diagnostic gap. Combining MRI findings with dermatomal sensory testing, physical examination, and detailed clinical history, it identifies the structural pain generator with 99% diagnostic accuracy before any surgical recommendation is made. That step determines whether a patient is a candidate for Deuk Laser Disc Repair®, Deuk Plasma Rhizotomy®, or, in appropriate cases, fusion.
Knowing which category your pain falls into before surgery is not optional information. It is the basis on which the surgical recommendation should be made.
Comparing Spinal Fusion Alternatives: What the Data Shows
How to Know Which Category You Fall Into
The question that drives this decision is not whether your MRI shows disc degeneration or herniation. At age 45 and older, nearly every adult has some degree of disc change visible on imaging. The question is whether those structural findings are generating the pain signal, and if so, through what mechanism.
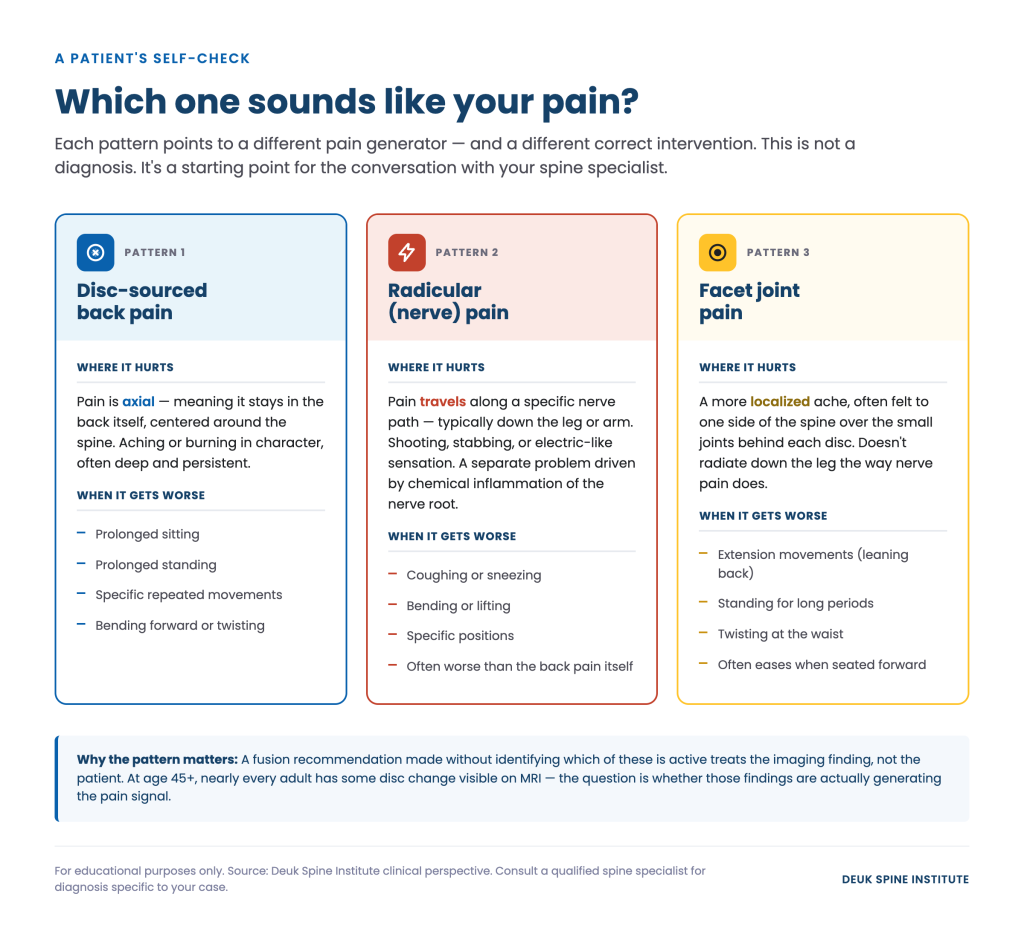
Disc-sourced pain typically presents as axial back pain, aching or burning in character, often worsened by prolonged sitting, standing, or specific movements. Radicular symptoms, the shooting, stabbing, or electric-like sensations that travel along a specific nerve path into the leg, are a separate problem driven by chemical inflammation of the nerve root, not by structural instability. Facet pain often presents as a more localized ache, frequently worse with extension movements.
Each pattern points toward a different pain generator and a different appropriate intervention. A fusion recommendation made without identifying which of these is active treats the imaging finding, not the patient.
If you have been recommended for spinal fusion and have not received a diagnostic evaluation that specifically identifies the structural source of your pain, a second opinion is warranted. Not because the original surgeon made a mistake, but because that information needs to be confirmed before a procedure that permanently changes your spine.
What Comes Next If You Want to Explore Alternatives to Spinal Fusion
The first step is identifying the actual pain source. A free MRI review is available at Deuk Spine Institute with no obligation. Our team will review your existing imaging and clinical history to determine whether your pain pattern is consistent with disc-sourced inflammation, facet joint arthritis, or a condition that genuinely requires fusion for structural stabilization.
If your pain originates from a disc injury, Deuk Laser Disc Repair® targets that source directly. If it originates from facet or sacroiliac joint arthritis, Deuk Plasma Rhizotomy® eliminates the pain-mediating nerves permanently. Both are outpatient procedures performed the same day, with no hospital admission and no permanent motion loss.
For a complete review of spinal fusion risks, including non-union, adjacent segment disease, hardware failure, and revision rates, see our article on spinal fusion complications. For an overview of what spinal fusion actually involves and when it is medically indicated, the spinal fusion guide covers that in detail.
A second opinion is not disloyalty to your surgeon. It is how patients gather the information they need before consenting to a procedure that permanently changes the structure of their spine.
Request a free MRI review or schedule a virtual consultation to find out whether a spinal fusion alternative applies to your case.
This article is for educational purposes only and does not constitute medical advice. Results from Deuk Laser Disc Repair® apply when the diagnosed pain source matches the treated pathology. Consult a qualified spine specialist to determine which treatment options are appropriate for your specific condition.
 in Lumbar MRI Imaging")

