

By Dr. Ara J. Deukmedjian
Board-Certified Neurosurgeon
Medically reviewed on May 14, 2026
Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
Key Points
✓ A 2025 Lown Institute analysis of Medicare claims found that U.S. hospitals performed more than 200,000 medically unnecessary back surgeries on older adults over a three-year period, costing taxpayers an estimated $1.9 billion. 1
✓ Complications of spinal fusion occur in up to 18% of patients and include infection, blood clots, stroke, pneumonia, heart and lung problems, and even death. 1
✓ The top 10% of physicians by spinal fusion overuse volume were responsible for 60% of all unnecessary fusion procedures, and the 3,454 physicians performing low-value back surgeries collectively received $64 million from device and drug companies. 2
✓ Florida ranks second in the nation for total volume of unnecessary spinal fusions (6,495 cases) and second for unnecessary vertebroplasties (8,302 cases), behind only California and Texas respectively. 1
✓ Adjacent segment disease (ASD), one of the most common long-term consequences of lumbar fusion, develops in roughly 18.6% of patients after posterior lumbar fusion and frequently leads to additional surgery. 3
✓ Deuk Laser Disc Repair® treats the actual pain generator through a 4mm to 7mm incision with no fusion, no hardware, no muscle cutting, and no bone removal, avoiding the surgical trauma that drives long-term failure after traditional fusion.
The Hidden Cost of Unnecessary Spinal Fusion in America

Chronic pain is one of the largest public health problems in the United States, and back pain sits at the top of that list. For more than 20 years I have watched patients walk into my clinic after years of suffering, after failed physical therapy, failed pain management injections, failed medications, and after being told that the only remaining option is a major open spinal fusion. Many of them never needed that surgery in the first place. The data on this is no longer anecdotal. It is published, peer-reviewed, and devastating.
In October 2025, the Lown Institute, an independent healthcare watchdog, released a national analysis of Medicare and Medicare Advantage claims covering 2020 to 2023. The headline finding: U.S. hospitals performed more than 200,000 unnecessary back surgeries on older adults across just three years and billed Medicare approximately $1.9 billion for those procedures. 1 Those numbers cover spinal fusion, laminectomy, and vertebroplasty cases that met the Institute’s strict criteria for low-value care, meaning the operations had little or no clinical benefit for the patients who received them.
This is not a story about a few bad actors. It is a structural problem in how American spine surgery is practiced, paid for, and marketed. And patients are paying the highest price, not in dollars. However, in disability, opioid dependence and living with chronic back pain for the rest of their lives if not properly treated.
What the Lown Institute Found About Spinal Fusion Overuse
The 2025 Lown report examined 2,547 hospitals for spinal fusion and laminectomy and 2,412 hospitals for vertebroplasty. 4 The findings shatter the assumption that surgical recommendations are uniformly driven by medical necessity.
The nationwide average overuse rate for spinal fusion and laminectomy was 13%. The overuse rate for vertebroplasty was 10%. But the averages hide an enormous variation between hospitals. At some institutions, fewer than 1% of spinal fusions met overuse criteria. At others, the rate exceeded 50%. Mount Nittany Medical Center in Pennsylvania logged the highest overuse rate in the country at 57.2%, meaning more than half of the spinal fusions performed there on Medicare patients had little or no expected clinical benefit. 1
The Lown researchers were not loose with their definitions. A spinal fusion was classified as overuse only when performed on a patient with low back pain who lacked any of the legitimate clinical indications, things like radicular symptoms, trauma, herniated disc, discitis, spondylosis, myelopathy, radiculopathy, radicular pain, or scoliosis. Stenosis with neural claudication and spondylolisthesis were specifically excluded from the overuse calculation, since those are accepted indications for fusion. Vertebroplasty was flagged as overuse for patients with osteoporotic spinal fractures, excluding those with bone cancer, myeloma, or hemangioma. 1
In other words, these were not edge cases. These were patients who, by any reasonable evidence-based standard, should not have been on an operating table.
Florida and the Geography of Spine Surgery Overuse
If you live in Florida and you have been told you need a spinal fusion, the data should give you pause before you consent. The Lown analysis ranked Florida second nationally for the total volume of unnecessary spinal fusions (6,495 cases) and second for unnecessary vertebroplasties (8,302 cases). 1 California led on fusion volume; Texas led on vertebroplasty volume. Within Florida, the variation among hospitals was striking: Tallahassee Memorial Hospital had a spinal fusion overuse rate of 4.0%, while Cape Coral Hospital was at 33.3%. For vertebroplasty, AdventHealth Sebring had a 0.0% overuse rate, while Halifax Health Medical Center was at 43.2%. 1
What that variation tells you is that your zip code, and more specifically the surgeon you happen to see, has a much larger influence on whether you end up with major spine surgery than the actual pathology on your MRI. That is not how evidence-based medicine is supposed to work.
The Doctors Behind the Numbers

A subsequent Lown Institute breakdown of the same dataset pinpointed an uncomfortable truth: this overuse is not evenly distributed across the profession. The top 10% of physicians by spinal fusion overuse volume were responsible for 60% of the total overuse in the country. 4 Of approximately 6,000 doctors who performed any spinal fusions in the dataset, 4,000 had zero surgeries that met overuse criteria. The 71,000 unnecessary spinal fusions traced back to roughly 2,000 surgeons, with the top 600 accounting for the vast majority. 5
The Lown team also identified more than 30 outlier physicians who each performed at least 100 procedures meeting overuse criteria, with personal overuse rates of 50% or higher, meaning every other spinal fusion they did was likely unnecessary. Five of those outliers practiced in a single state, Alabama. 5 At one Pennsylvania hospital, a single physician was responsible for 92% of all overuse procedures, performing 308 of the 336 unnecessary spinal fusions and laminectomies at the institution. 6
This is the part of the story that explains everything else. A minority of surgeons, operating with high volume in a financially permissive environment, are driving the bulk of the harm.
Why Doctors Are Recommending Procedures Patients Do Not Need
The answer is uncomfortable, but it is not complicated: money, training inertia, and patient desperation.

Financial Incentives
Spinal fusion is one of the highest-reimbursed surgeries a hospital can perform. The implants alone, screws, rods, plates, and cages, generate enormous revenue for device manufacturers. A Conflixis analysis embedded in the Lown report found that the 3,454 physicians who performed unnecessary back surgeries collectively received $64 million in compensation from drug and medical device companies during the study period. 2 That is not a coincidence.
A 2025 peer-reviewed analysis published in the North American Spine Society Journal compared self-reported financial disclosures from spine surgeons participating in the 2023 NASS conference against the federal Open Payments database. The authors documented widespread discrepancies, with surgeons routinely failing to disclose industry relationships that the federal database had on record. 7 A separate 2024 analysis of NASS conference participants found that 151 spine surgeons received industry payments totaling $48.3 million in a single year, with royalties accounting for the largest share of dollars exchanged. 8
When a surgeon owns a royalty stake in a specific fusion implant, every fusion they perform is, in part, a personal product placement. That conflict is legal. It is also documented to influence clinical decision making.
Training Inertia
Spinal fusion has been the dominant surgical answer to back pain for decades, and most surgeons in practice today were trained during the era when it was the unquestioned standard of care. I was one of them. Early in my career I performed fusions because that was what I had been taught to do. The clinical evidence has shifted significantly since then, but the surgical economy is slow to follow. Hospitals still have fusion-heavy operating room schedules, device reps still walk the halls, and the patient in front of the surgeon is still being offered the procedure the surgeon was trained to perform, not necessarily the procedure the patient actually needs.
Patient Desperation
Chronic pain patients are uniquely vulnerable to overtreatment. They have already failed conservative care. They have lost sleep, lost work, and in many cases lost hope. When a surgeon offers a major operation that promises relief, patients often consent without exhausting the alternatives. The literature is unambiguous on what happens next: a 2025 Neurosurgical Review systematic review and meta-analysis comparing spinal fusion to nonoperative treatment for lumbar degenerative pathology synthesized the available evidence and found that the benefit of fusion over multidisciplinary nonsurgical care remains far from definitive in most patient populations. 9
The Real Outcomes of Spinal Fusion
The marketing brochure version of spinal fusion is that it eliminates pain by stopping motion at a damaged segment. The published outcome data is more sobering.
A widely cited study in the European Spine Journal found that the minimal clinically important difference for back pain was achieved in only about 50% of patients after lumbar fusion. 10 That is the same statistical outcome as a coin flip, for a procedure that involves cutting bone, implanting hardware, and permanently locking spinal segments.
Beyond the immediate failure rate, fusion creates a cascade of downstream problems:

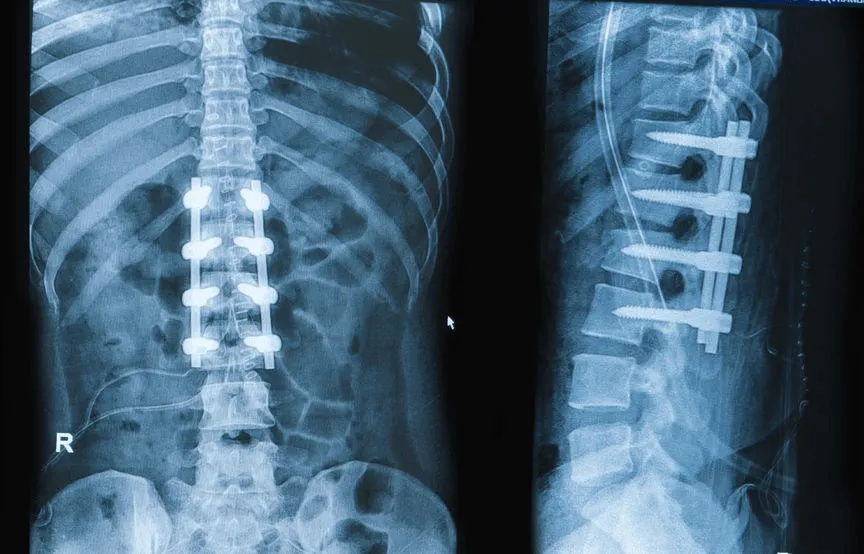
Adjacent segment disease. When two vertebrae are fused, the segments above and below are forced to absorb the motion the fused level no longer provides. Over years, those adjacent levels degenerate at an accelerated rate. A meta-analysis of 19 studies covering nearly 3,000 patients found an overall adjacent segment disease rate of 18.6% after posterior lumbar fusion. 3 A 2025 systematic review reported adjacent segment degeneration in 36% and clinically symptomatic adjacent segment disease in 11% of fusion patients within two to seven years of surgery. 11 Many of these patients return to the operating room for a second fusion, then a third.
Surgical complications. Complications of spinal fusion occur in up to 18% of patients, ranging from infection and blood clots to stroke, pneumonia, heart and lung problems, and death. 1
Opioid dependence and overdose death. When fusion fails to relieve pain, the prescription cascade that follows is dangerous in its own right. Published research on lumbar fusion outcomes has identified opioid overdose as a leading cause of death among patients who develop Failed Back Surgery Syndrome.
Hardware failure. Screws loosen, rods break, cages migrate. Each hardware problem typically requires another operation.
Pseudarthrosis. The bone graft fails to fuse in a meaningful percentage of cases, leaving the patient with hardware, motion at a level that was supposed to be locked, and pain.
The cumulative effect of all this is that the original $1.9 billion in unnecessary Medicare spending is only the beginning. Once you add the cost of revision fusions, spinal cord stimulators, long-term opioids, disability payments, and lost productivity, the real economic footprint of unnecessary spinal fusion in the United States is many multiples of that figure.
Vertebroplasty: The Other Side of the $2 Billion Problem
The 2025 Lown analysis devoted significant attention to vertebroplasty, the procedure where medical-grade cement is injected into a vertebra to stabilize an osteoporotic compression fracture. Multiple high-quality randomized trials have shown that vertebroplasty offers little to no benefit over a sham procedure for most patients with osteoporotic spinal fractures, yet the procedure continues to be performed at high volume across the country. 1
The Centers for Medicare and Medicaid Services included vertebroplasty on its list of 17 services targeted by the new Wasteful and Inappropriate Service Reduction (WISeR) Model, a prior authorization pilot launching in six states in 2026 that combines artificial intelligence with human clinical review to flag low-value procedures before they are paid for. 4 The inclusion of vertebroplasty in that pilot is a direct federal acknowledgment that overuse is real, measurable, and worth intercepting.
The Patient Selection Problem No One Talks About

There is another layer to the spine surgery overuse problem that the financial story alone does not capture. Patient selection for surgery has been studied for decades and the results are uncomfortable. A systematic review in The Spine Journal concluded that none of the diagnostic tests commonly used to select fusion candidates, including MRI, provocative discography, facet joint blocks, orthosis immobilization, and temporary external fixation, demonstrated clinically useful prognostic accuracy. 12 In plain language, the field cannot reliably predict which patients will benefit from a fusion based on the tools currently used to recommend it.
This matters because it means even surgeons acting in complete good faith are operating on patients who, on paper, look like fusion candidates but in practice will not benefit. Add in the financial incentives, the training inertia, and the desperation of the patient population, and the surgical overuse problem becomes almost inevitable.
What the Modern Evidence Says About Minimally Invasive Alternatives
The good news is that the surgical world has not stood still while fusion overuse has grown. Endoscopic and laser-based techniques targeting the actual pain generator have matured into well-studied alternatives to traditional open spine surgery.
A 2025 systematic review and meta-analysis published in the International Journal of Surgery compared minimally invasive endoscopic discectomy with conventional surgical techniques across multiple randomized trials and high-quality observational studies. The analysis concluded that endoscopic techniques produced comparable or superior outcomes to traditional open microdiscectomy with significantly less tissue trauma, shorter hospital stays, and faster return to function. 13 A 2025 Global Spine Journal meta-analysis comparing unilateral biportal endoscopic discectomy with microdiscectomy reached similar conclusions. 14
The clinical principle behind these findings is straightforward. Less surgical trauma means less of the scar tissue, instability, and adjacent segment stress that drives long-term failure after fusion. Targeting the actual pain generator, the herniated disc fragment, the inflamed facet, the pinched nerve, with a precise, motion-preserving procedure protects everything else the spine still does well.
A Different Approach: Targeting the Source of Pain Without Fusion

About 20 years ago, after years of performing traditional fusions and watching too many patients return worse than they came in, I developed Deuk Laser Disc Repair®, an endoscopic laser spine procedure designed around a single principle: treat the actual pain generator without destabilizing the spine.
The procedure is performed through a 4mm to 7mm incision. There is no muscle cutting, no bone removal, no hardware, and no fusion. A precision laser is used to remove the herniated disc material and decompress the inflamed annular tear that is generating the pain. Because nothing is fused and nothing is implanted, there is no adjacent segment disease, no pseudarthrosis, no hardware failure, no post-operative narcotics, and no months-long recovery.
For SI joint and facet joint pain, Deuk Plasma Rhizotomy® targets the small nerve branches generating the pain without disturbing the joint itself. These are the cases that most often get misdiagnosed as fusion candidates, because the standard imaging and exam workup misses the true source.
The point is not that minimally invasive procedures are universally appropriate. The point is that the question every patient deserves to have answered before consenting to a fusion is whether the actual pain generator on their MRI has been identified, and whether there is a less invasive procedure capable of addressing it.
Questions to Ask Before You Consent to Spinal Fusion
If a surgeon has recommended a spinal fusion, the answers to the following questions should be specific, documented, and consistent with current evidence. Vague answers are a warning sign.
- What specific structure on my MRI is generating my pain?
- How was that pain generator confirmed beyond imaging alone, through physical exam findings, diagnostic injections, or correlation with reported symptoms?
- Do I meet the published indications for fusion, such as instability, spondylolisthesis with neural claudication, deformity, or trauma?
- What is the least invasive procedure that can address my specific pathology?
- What is your personal complication rate, infection rate, and reoperation rate for the procedure you are recommending?
- Do you have any financial relationships with the manufacturer of the implants you plan to use, and are those relationships disclosed in the federal Open Payments database?
- What happens to me if I do nothing for six more months while exhausting nonsurgical care?
A surgeon who cannot or will not answer these questions in detail is not the surgeon you want operating on your spine. Hardware cannot be unscrewed. Fused vertebrae cannot be unfused. Removed bones do not grow back. The first surgery is the one most likely to help. It is also the one most worth getting right.
When to Seek Medical Attention
| Level of Care | Symptoms |
| See a Specialist Spine specialist evaluation. Schedule a consultation. | Persistent or worsening back or neck pain. Pain radiating into the arms or legs. Numbness, tingling, or weakness in the extremities. A recommendation for spinal fusion you want a second opinion on. |
| Emergency Go to the ER immediately. Possible cauda equina syndrome, a surgical emergency that cannot wait. | Sudden loss of bladder or bowel control. Saddle anesthesia, meaning numbness in the groin or inner thighs. Rapidly progressive weakness in both legs. |
The Bottom Line
The $1.9 billion in unnecessary Medicare spending documented by the Lown Institute is not an abstraction. 1 It is more than 200,000 real people, most of them older adults, who were put through major operations that the published evidence says they did not need. Many of them are now living with worse pain, worse function, and worse quality of life than they had before surgery. Some are dependent on opioids. Some have died from complications.
This is fixable. The medical literature on adjacent segment disease, surgical complication rates, conflict of interest, and minimally invasive alternatives is not hidden. It is in PubMed, in the European Spine Journal, in Neurosurgical Review, in the North American Spine Society Journal, and in the Lown Institute’s public dataset. Patients and policymakers have access to the same evidence the profession does, and the WISeR pilot at CMS shows the federal payer is finally beginning to act on it.
If you have been recommended for spinal fusion, especially in a state where overuse rates are high, get a second opinion from a surgeon who is not financially connected to the implant manufacturer. Ask the questions above. Upload your MRI for a free virtual consultation with Dr. Ara Deukmedjian, M.D., founder of Deuk Spine Institute and creator of the Deuk Laser Disc Repair® procedure. We will tell you what is generating your pain and whether a precise, motion-preserving option can address it without the lifelong trade-offs of fusion.

Frequently Asked Questions
How many spinal fusions in the United States are medically unnecessary?
A 2025 Lown Institute analysis of three years of Medicare and Medicare Advantage claims (2020 to 2023) found that U.S. hospitals performed more than 200,000 unnecessary back surgeries on older adults, including spinal fusions, laminectomies, and vertebroplasties, at an estimated cost of $1.9 billion. 1 The nationwide overuse rate for spinal fusion and laminectomy was 13%, with individual hospitals ranging from under 1% to over 57%.
Why do some surgeons recommend spinal fusion when the evidence does not support it?
Three factors converge to drive overuse. First, financial incentives: spinal fusion is highly reimbursed, and the surgeons performing low-value back surgeries collectively received $64 million from device and drug companies during the Lown study period. 2 Second, training inertia: most surgeons in practice were trained when fusion was the standard answer to back pain. Third, patient desperation, which makes it easier to consent to major surgery without exhausting alternatives. The Lown data also show that 60% of overuse is concentrated in just the top 10% of physicians by volume. 4
What is adjacent segment disease, and how often does it happen after fusion?
Adjacent segment disease (ASD) is degeneration of the spinal segments above and below a fusion, caused by the extra mechanical stress those segments must absorb when the fused level no longer moves. A meta-analysis of 19 studies covering 2,896 patients found a 18.6% rate of ASD after posterior lumbar fusion, 3 and a 2025 systematic review reported a 36% rate of adjacent segment degeneration and an 11% rate of clinically symptomatic ASD within two to seven years of surgery. 11 ASD frequently leads to additional surgery.
Are there alternatives to spinal fusion that actually work?
Yes, for most patients with disc-related pain. A 2025 systematic review and meta-analysis published in the International Journal of Surgery found that minimally invasive endoscopic discectomy produced comparable or superior outcomes to traditional open microdiscectomy with significantly less tissue trauma and faster recovery. 13 Deuk Laser Disc Repair® treats the actual pain generator through a 4mm to 7mm incision with no fusion, no hardware, no muscle cutting, and no bone removal, eliminating the surgical trauma that drives adjacent segment disease and other long-term complications of fusion.
How can I tell if my spinal fusion recommendation is appropriate or unnecessary?
A legitimate fusion recommendation should be backed by a specific structural diagnosis on imaging that correlates with your physical exam, a clear indication from the published literature (such as instability, spondylolisthesis with neural claudication, deformity, or trauma), and a documented failure of appropriate nonsurgical care. If your surgeon cannot specify exactly what structure is generating your pain or whether less invasive alternatives have been considered, or if you fall into the Lown Institute’s overuse category (low back pain without radicular symptoms, trauma, herniated disc, discitis, spondylosis, myelopathy, radiculopathy, or scoliosis), a second opinion from a surgeon without financial ties to a specific implant manufacturer is essential.
Sources
- Lown Institute. PRESS RELEASE: Older adults get unnecessary back surgeries at an alarming rate. October 2025. https://lowninstitute.org/press-release-older-adults-get-unnecessary-back-surgeries-at-an-alarming-rate/
- Jaklevic MC. Worthless back surgeries are a nagging pain for U.S. health care. Association of Health Care Journalists. November 2024. https://healthjournalism.org/blog/2024/11/worthless-back-surgeries-are-a-nagging-pain-for-u-s-health-care/
- Wang T, Ding W. Risk factors for adjacent segment degeneration after posterior lumbar fusion surgery in treatment for degenerative lumbar disorders: a meta-analysis. https://pmc.ncbi.nlm.nih.gov/articles/PMC7713357/
- Muoio D. Medicare spent $1.9B on unnecessary back surgeries over 3 years, report finds. Fierce Healthcare. October 2025. https://www.fiercehealthcare.com/providers/medicare-spent-19b-unnecessary-back-surgeries-over-3-years-report-finds
- Lown Institute. Physicians who perform the most unnecessary back surgeries: what we know. October 2025. https://lowninstitute.org/physicians-who-perform-the-most-unnecessary-back-surgeries-what-we-know/
- Lown Institute. PRESS RELEASE: Unnecessary back surgeries cost Medicare up to $600 million annually. https://lowninstitute.org/press-release-unnecessary-back-surgeries-cost-medicare-up-to-600-million-annually/
- Vallee EK, Alben MG, Chipman DE, et al. Spine surgeon conflict of interest disclosure discrepancies between a national conference and the open payments database. North American Spine Society Journal. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11999366/
- Lucasti C, Vallee EK, Scott MM, et al. Differences in Financial Conflicts of Interest Among Participants in a National Spine Conference. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11418697/
- Moghib K, Altalab G, Jader A, et al. Comparison between spinal fusion vs. nonoperative treatment for lumbar degenerative pathology: a systematic review and meta-analysis. Neurosurgical Review. 2025. https://link.springer.com/article/10.1007/s10143-025-03671-2
- Minimal clinically important difference after lumbar fusion for low back pain. PubMed. https://pubmed.ncbi.nlm.nih.gov/37486861/
- Impact of iatrogenic alterations on adjacent segment degeneration after lumbar fusion surgery: a systematic review. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12039085/
- Willems P. Spinal fusion for chronic low back pain: systematic review on the accuracy of tests for patient selection. The Spine Journal. https://pubmed.ncbi.nlm.nih.gov/23127364/
- Comparative effectiveness of minimally invasive endoscopic discectomy versus conventional surgical techniques for lumbar disc herniation: a systematic review and meta-analysis. International Journal of Surgery. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12577904/
- Waseem MH, ul Abideen Z, Ahsan M, et al. Comparing Unilateral Biportal Endoscopic Discectomy Versus Microdiscectomy for Lumbar Disc Herniation: A Systematic Review and Meta-Analysis. Global Spine Journal. 2025. https://journals.sagepub.com/doi/10.1177/21925682251412289


