


Patients who receive a spinal fusion surgery recommendation often leave their surgeon’s office with more questions than answers. They understand the procedure is significant. They understand recovery takes time. What they often do not understand fully is what fusion permanently changes about their spine — and whether alternatives were ever considered.
Over 30 years of spine surgery practice, I have performed spinal fusion for patients who genuinely needed it. Instability, fracture, deformity — there are conditions where fusion is the medically appropriate answer. But I have also evaluated thousands of patients who arrived at Deuk Spine Institute already scheduled for fusion when a motion-preserving procedure could have resolved their pain without permanently eliminating movement at a spinal level. The difference matters enormously for long-term quality of life.
This guide covers spinal fusion honestly: what it is, why surgeons recommend it, what the procedure involves, what recovery actually looks like, and what patients should understand about long-term outcomes before consenting. If you have been recommended for fusion, this information belongs in your hands before you make a decision.
This article is for educational purposes only and does not constitute medical advice. Consult a qualified spine specialist before making any treatment decisions.
What Spinal Fusion Surgery Actually Does
Spinal fusion permanently joins two or more vertebrae into a single, immobile unit. The goal is to eliminate motion at a specific spinal segment — which, in cases of genuine structural instability, can reduce pain caused by abnormal movement at that level.
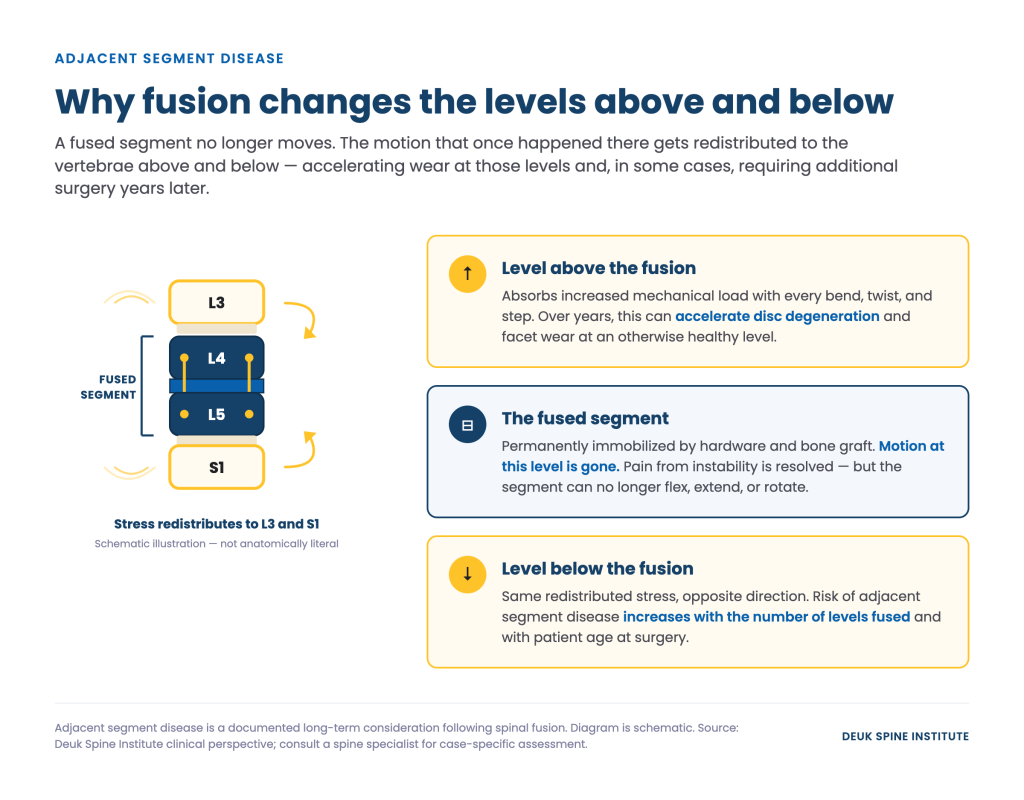
The procedure works by placing bone graft material between the target vertebrae and using implanted hardware to hold the segment fixed while the bone fuses over the following months. Once fusion is complete, that spinal level no longer moves. The motion that once occurred there is redistributed to the segments above and below.
That redistribution is not an incidental side effect. It is the biomechanical consequence of eliminating movement at one level — and it is the documented mechanism behind adjacent segment disease, one of the most significant long-term considerations for fusion patients. Understanding this from the outset shapes how patients should weigh fusion against motion-preserving alternatives.
When Spinal Fusion Is the Right Recommendation
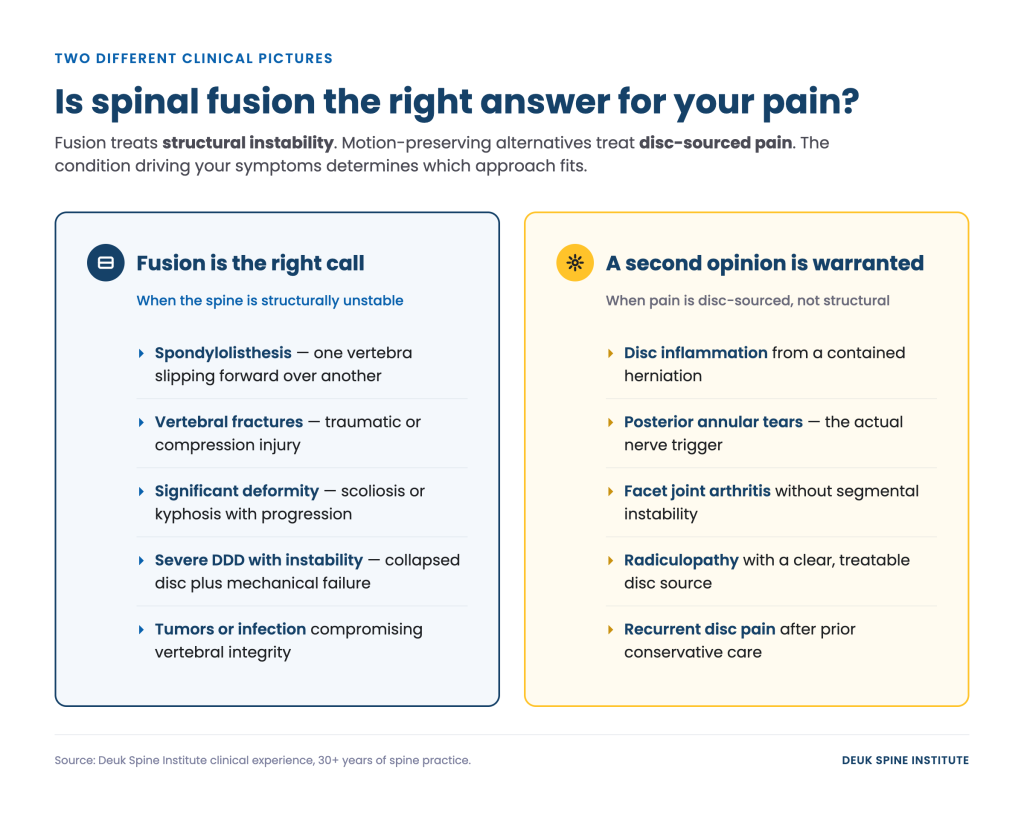
There are clinical conditions where spinal fusion is medically appropriate and, in some cases, necessary. These are not primarily conditions of disc-sourced inflammation. They are conditions involving structural failure at the vertebral level.
- Spondylolisthesis: When one vertebra slips forward over another, the resulting instability cannot be resolved without stabilizing the segment. Fusion restores structural alignment and eliminates the abnormal movement driving nerve compression or mechanical pain.
- Severe degenerative disc disease with structural instability: When a disc has collapsed significantly and the spinal segment is mechanically unstable — not simply painful — fusion may be appropriate to restore load-bearing function.
- Vertebral fractures: Traumatic or compression fractures that compromise spinal integrity may require fusion to stabilize the spine and protect the spinal cord.
- Spinal deformity: Scoliosis or kyphosis with significant curvature can cause progressive neurological damage. Fusion corrects alignment and halts further progression.
- Tumors or infections affecting vertebral integrity: Structural compromise from pathological causes sometimes requires surgical stabilization following treatment.
The clinical distinction that matters most: fusion addresses structural instability. For patients whose pain originates from disc inflammation, posterior annular tears, or facet joint arthritis without accompanying instability, the rationale for fusion weakens considerably. That is precisely where motion-preserving alternatives deserve serious evaluation.
Types of Spinal Fusion Surgery
There are several approaches to spinal fusion, each named for the surgical corridor used to reach the spine. The appropriate approach depends on the level being fused, the patient’s anatomy, and the surgeon’s training.
- ACDF (Anterior Cervical Discectomy and Fusion): The most common fusion procedure for the cervical spine. The surgeon approaches from the front of the neck, removes the damaged disc, and fuses the adjacent vertebrae using a bone graft and plate. Used for herniated cervical discs, cervical radiculopathy, and cervical myelopathy when conservative treatment has failed.
- ALIF (Anterior Lumbar Interbody Fusion): Performed through the abdomen to access the lumbar spine from the front. Allows placement of a large interbody cage without disrupting the back muscles. Typically used at L4-L5 and L5-S1.
- PLIF (Posterior Lumbar Interbody Fusion): Performed through the back. The surgeon retracts the paraspinal muscles, removes portions of the facet joint for access, and places bone graft or cages between the vertebral bodies from behind.
- TLIF (Transforaminal Lumbar Interbody Fusion): A variation of PLIF performed at an angle through the neural foramen, requiring less retraction of neural structures. Currently the most commonly performed lumbar fusion approach.
Minimally invasive versions of PLIF and TLIF have been developed to reduce muscle damage, though the fundamental fusion — and its long-term consequences — remains the same regardless of the approach used.
What the Procedure Involves
Regardless of approach, spinal fusion surgery shares common components: anesthesia, surgical access to the spine, decompression of any compressed neural structures, placement of bone graft material, and implantation of hardware to stabilize the segment during healing.
Bone graft is required because fusion depends on new bone growing across the treated segment. Surgeons use one of three primary graft options:
- Autograft: Bone harvested from the patient’s own body, typically the iliac crest (hip). Considered the gold standard for fusion rates, but adds a second surgical site and a separate source of post-operative pain.
- Allograft: Bone from a donor (cadaver) processed and sterilized for implantation. Avoids the donor site pain of autograft but has somewhat lower fusion rates in some studies.
- Bone graft substitutes and biologics: Synthetic materials or growth factors (such as BMP) used to stimulate bone formation. Used increasingly in complex cases, with ongoing research into long-term performance.
Surgical duration ranges from approximately two hours for a single-level cervical fusion to six or more hours for multi-level lumbar cases. Most patients require a hospital stay of one to two nights for single-level procedures, with multi-level fusions extending to three or four nights. This stands in contrast to motion-preserving procedures like Deuk Laser Disc Repair®, which are performed on an outpatient basis with same-day discharge.
What Recovery From Spinal Fusion Actually Looks Like

Spinal fusion recovery is measured in months, not weeks. The bone graft must biologically incorporate and grow across the treated segment — a process that cannot be accelerated by activity or willpower. Understanding the realistic timeline before surgery prevents the frustration that many fusion patients experience during a recovery that feels longer and harder than they anticipated.
- Months 1–3: Significant activity restrictions. Patients are typically instructed to avoid bending, lifting, or twisting. Driving is restricted. Most patients cannot return to desk work for several weeks and physical labor for considerably longer. Pain from the surgical site, and from the graft harvest site in autograft cases, is common during this period.
- Months 3–6: Formal physical therapy typically begins once the fusion shows early radiographic evidence of incorporation. Therapy focuses on rebuilding strength in the muscles surrounding the fused segment — muscles that may have been damaged during the surgical approach.
- Months 6–12: The fusion is considered complete when imaging confirms solid bone bridging across the treated level. For some patients, particularly smokers, diabetics, or those with osteoporosis, this timeline extends further. During this entire period, the hardware holds the segment in place while awaiting bone consolidation.
By comparison, patients who undergo Deuk Laser Disc Repair® walk independently within one hour of their procedure and are discharged the same day. Recovery timelines are not equivalent, and patients deserve to understand that difference before choosing between options.
Long-Term Considerations After Spinal Fusion
Spinal fusion produces real outcomes for patients with the right clinical indications. Published success rates for lumbar fusion range from approximately 70 to 90 percent, depending on the indication, patient selection, and how “success” is defined. Those are meaningful results for appropriately selected patients.
They are also not universal — and they come with documented long-term considerations that patients should understand before surgery.
Adjacent segment disease: The vertebral segments above and below a fusion absorb increased mechanical stress over time. This accelerated loading can cause degeneration at adjacent levels, sometimes requiring additional surgery years after the original procedure. The risk increases with the number of levels fused and with patient age at the time of surgery.
Non-union and pseudarthrosis: Fusion fails to achieve solid bone consolidation in approximately 5 to 10 percent of cases. When this occurs, the hardware may fail under repeated stress loads, causing persistent pain and, in some cases, requiring revision surgery. Smoking, obesity, osteoporosis, and multi-level constructs all increase non-union risk.
Hardware complications: Screws, rods, and cages are permanently implanted in most fusion patients. Hardware can loosen, migrate, or break over time — particularly in patients who return to high-demand physical activity. Revision surgery to address hardware complications carries additional risk compared to the original procedure.
Permanent motion loss: The fused segment does not move. For most activities of daily living, this loss is tolerable. For patients who depend on full spinal mobility — athletes, manual laborers, younger patients — the long-term functional impact of permanent motion restriction at one or more levels is worth weighing carefully.
Fusion Is the Right Answer for Some Patients
I want to be direct about this: spinal fusion is an appropriate and sometimes necessary procedure. For patients with documented structural instability — spondylolisthesis, fracture, deformity — fusion provides something that no motion-preserving procedure can: structural stabilization. In those cases, I recommend fusion because it is the right recommendation.
The problem is not fusion itself. The problem is when fusion is recommended for patients whose pain originates from disc inflammation, posterior annular tears, or facet joint arthritis — conditions that do not involve structural instability and where the source of pain can be directly treated without eliminating spinal motion.
For patients in that second category, a motion-preserving option like Deuk Laser Disc Repair® targets the actual source of pain — the inflammation within the posterior annular tear — rather than immobilizing the segment. The procedure takes approximately 20 minutes per disc, is performed on an outpatient basis, and patients are discharged the same day. In our clinical experience with over 2,700 Deuk Laser Disc Repair® procedures, patients report an average of 99% pain relief for treated pain sources, with a complication rate of 0.01% and a 0% infection rate.
Knowing which category you fall into starts with an accurate diagnosis. The Deuk Spine Exam® combines MRI findings, physical examination, and clinical history to identify the structural source of your pain with 99% diagnostic accuracy — before any surgical recommendation is made.
If you have been recommended for spinal fusion and want to understand whether a motion-preserving alternative applies to your case, a free MRI review is available with no obligation. A second opinion is not disloyalty to your surgeon. It is how patients make informed decisions about procedures that permanently change their spine.
For patients seeking a deeper look at the risks associated with fusion surgery — non-union, adjacent segment disease, revision rates, hardware failure — the next article in this series covers spinal fusion complications in detail. For patients already exploring what comes next, our guide to alternatives to spinal fusion is a useful starting point.
This article is for educational purposes only and does not constitute medical advice. Results from Deuk Laser Disc Repair® apply when the diagnosed pain source matches the treated pathology. Consult a qualified spine specialist to determine which treatment options are appropriate for your specific condition.



