

If a surgeon has recommended lumbar laminectomy for your back pain, you are likely living with leg symptoms, heaviness with walking, or pain that has not responded to conservative care. The recommendation is common. Lumbar laminectomy is one of the most frequently performed spine operations in the United States, and for certain presentations, it provides genuine relief.
But “common” does not mean appropriate for every patient. Relief of leg symptoms is not the same as elimination of back pain. After over 30 years performing spine surgery, I have evaluated thousands of patients who had a laminectomy elsewhere and came to Deuk Spine Institute still suffering. Understanding what this surgery does, and what it leaves untreated, separates patients who recover fully from those who cycle through procedures without resolution.
What Is Lumbar Laminectomy and Who Is It Recommended For?
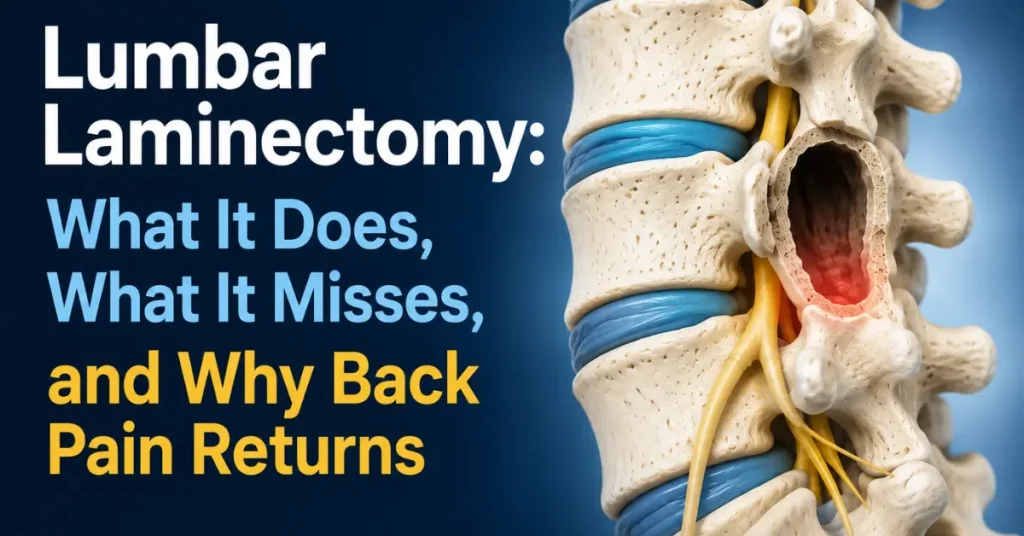
Lumbar laminectomy is a surgical procedure that removes a portion of the lamina, the flat bone forming the posterior arch of each vertebra. The lamina is part of the bony ring that surrounds and protects the spinal canal. When that canal narrows, a condition called lumbar spinal stenosis, neural structures inside become compressed.
Surgeons recommend lumbar laminectomy primarily for patients with:
- Lumbar spinal stenosis causing neurogenic claudication, the progressive leg heaviness, cramping, or weakness that worsens with walking and improves with rest or forward flexion
- Severe nerve compression producing weakness, numbness, or bowel and bladder dysfunction
- Failed conservative treatment including physical therapy, epidural steroid injections, and pain management over several months
- Imaging confirmation showing moderate to severe canal narrowing at one or more lumbar levels, most often L4-L5 or L3-L4
The logic is anatomical: if bone is compressing neural tissue, remove the bone and decompress the canal. For patients whose primary problem is mechanical compression of the spinal cord or nerve roots, this approach has merit.
Some patients are offered a smaller-scale version of this same idea, a laminotomy, which removes less bone but carries its own tradeoffs in recovery time and long-term spinal stability. Understanding how laminotomy and laminectomy actually differ matters before consenting to either one.
What Lumbar Laminectomy Actually Does to the Spine
To understand why lumbar laminectomy works for some symptoms but not others, you need a clear picture of what the surgery physically accomplishes.
The surgeon accesses the posterior spine through an incision in the lower back, retracts the paraspinal muscles away from the vertebrae, and uses bone-cutting instruments to remove some or all of the lamina at the affected level. In a standard laminectomy, the entire lamina and spinous process are removed. Variations of the procedure remove smaller amounts of bone while still creating canal space.
What this creates is a wider spinal canal with more room for the nerves. The compression from the overgrown bone is removed. Leg symptoms caused by stenosis often improve markedly. For patients whose dominant complaint was neurogenic claudication, this can be a successful surgery.
What lumbar laminectomy does not do is equally important:
- It does not treat disc pathology. The intervertebral discs at the affected level remain exactly as they were before surgery.
- It does not address annular tears. If a posterior annular tear existed prior to surgery, that tear continues generating inflammation after laminectomy is complete.
- It does not remove the inflammatory pain signal. The chemical environment inside a painful disc does not change because bone was removed above it.
- It does not restore disc height. A degenerated disc remains degenerated.
- It does not stop neoinnervation. Small pain nerve fibers that have grown into damaged disc tissue do not retract after a laminectomy.
This matters enormously because the majority of patients presenting for lumbar laminectomy have coexisting disc pathology. Spinal stenosis and disc degeneration frequently occur at the same levels, in the same age group, for overlapping biomechanical reasons. Treating one while ignoring the other is why back pain so often persists or returns after this surgery.
The Pain Source Lumbar Laminectomy Cannot Reach
Through clinical practice spanning over 30 years and more than 2,700 Deuk Laser Disc Repair® procedures, I have identified 30 structurally distinct sources of chronic back pain. Disc injuries are the most prevalent, accounting for approximately 85% of chronic back pain cases. The most commonly affected levels are L4-L5, L5-S1, L3-L4, and L2-L3, in that order.
Disc pain originates from a specific mechanism. When the annulus fibrosus develops a tear in its posterior wall, the nucleus pulposus migrates into or through that tear. This herniation triggers ongoing inflammation within and around the posterior annular tear, an inflammation that does not resolve on its own the way acute soft tissue injuries do.
Over time, the body responds to this ongoing inflammation by growing new pain nerve fibers into the damaged tissue, a process called neoinnervation. This is why disc pain often becomes more severe over months and years rather than improving. The structural damage creates a self-sustaining inflammatory cycle.
Lumbar laminectomy is performed at the posterior arch of the vertebra. The disc sits anterior to the surgical field. The annular tear is not debrided. The herniated nucleus pulposus material in the tear is not addressed. The inflammatory environment that drives the ongoing pain signal is untouched by the procedure.
A patient who undergoes lumbar laminectomy for stenosis may walk better. Their leg cramping may resolve. But if a painful disc at L4-L5 was also generating their axial back pain, that back pain will remain once the recovery process is complete, because the surgery was never designed to address it.
- Lumbar spinal stenosis causing neurogenic claudication, the progressive leg heaviness, cramping, or weakness that worsens with walking and improves with rest or forward flexion
- Severe nerve compression producing weakness, numbness, or bowel and bladder dysfunction
- Failed conservative treatment including physical therapy, epidural steroid injections, and pain management over several months
- Imaging confirmation showing moderate to severe canal narrowing at one or more lumbar levels, most often L4-L5 or L3-L4
Failure Modes and Documented Risks of Lumbar Laminectomy
Lumbar laminectomy carries surgical risks that every patient should understand before consenting. The most common include:
- Spinal instability. The lamina contributes to the structural integrity of the posterior vertebral arch. Removing it, particularly at multiple levels or bilaterally, can destabilize the segment. This sometimes requires a follow-up fusion surgery, which carries its own risks and recovery demands.
- Adjacent segment degeneration. When biomechanical stress is redistributed after laminectomy, the disc levels above and below the operated segment may deteriorate at an accelerated rate.
- Epidural fibrosis. Scar tissue forming in the surgical field can compress nerves, producing pain similar to or worse than the original stenosis.
- Infection. Any open spine surgery involves exposure of deep tissue and bone, with associated infection risk.
- Dural tear and cerebrospinal fluid leak. The dura, the membrane surrounding the spinal cord, can be damaged during bone removal, requiring repair and extended recovery.
- Persistent or returning pain. If the underlying disc pathology is not addressed, back pain does not resolve. This outcome is sufficiently common that it has a clinical name: Failed Back Surgery Syndrome.
Failed Back Surgery Syndrome is not a fringe outcome. It describes patients who had spine surgery, experienced inadequate relief or recurrence, and continue to suffer. Many of these patients end up on long-term opioid regimens, repeat injections, or additional surgeries. The root cause in a large proportion of cases is that the original surgery treated a structural finding on imaging rather than the specific pain generator driving the patient’s symptoms.
Understanding why that mismatch happens so often comes down to what laminectomy physically can and cannot reach — and why the anatomy it targets is rarely the source of the pain.
Deuk Laser Disc Repair® Targets What Lumbar Laminectomy Ignores
Deuk Laser Disc Repair® treats the structural source of disc-driven back pain: the posterior annular tear with its associated inflammation and herniated nucleus pulposus material. It is the only surgical procedure in the world that directly addresses this anatomy. In over 2,700 procedures, patients report an average of 99% pain relief for treated pain sources, with a complication rate of 0.01% and an infection rate of 0%.
The procedure uses a 7mm incision to access the disc from a lateral approach. No bone is drilled, no lamina is removed. The surgeon removes the herniated nuclear material from the posterior annular tear, debrides the inflamed tissue, and eliminates the pain signal at its source. The tear heals naturally over the following months without bone grafts or hardware.
Each procedure takes approximately 20 minutes per disc level. Patients are ambulatory within hours and discharged the same day, with no hospital admission and no weeks of recovery that come with open posterior spine surgery.
The clinical difference comes down to diagnosis. Lumbar laminectomy treats canal narrowing visible on MRI without always confirming that the canal narrowing is actually causing the patient’s pain. Deuk Spine Exam® combines MRI findings with physical examination and detailed pain history to identify the specific pain generator with 99% diagnostic accuracy. When a disc is the confirmed pain source, Deuk Laser Disc Repair® treats that exact disc. The result is targeted relief rather than structural modification that may or may not correspond to the patient’s symptoms.
Lumbar Laminectomy vs. Deuk Laser Disc Repair®
| Comparison | Lumbar Laminectomy | Deuk Laser Disc Repair® |
|---|---|---|
| Surgical target | Posterior lamina bone | Posterior annular tear and disc inflammation |
| Addresses disc pain | No | Yes, directly |
| Bone removal | Yes, lamina removed | No bone drilling or removal |
| Incision size | Multiple centimeters, posterior midline | 7mm lateral lumbar incision |
| Hospital stay | Typically 1-3 days inpatient | Same-day outpatient discharge |
| Motion preservation | May require fusion for stability | Full spinal motion preserved |
| Complication rate | Infection, dural tear, instability, fibrosis | 0.01% complication rate, 0% infection rate |
| Treats axial back pain | No | Yes, when disc is confirmed pain source |
| Procedure duration | 1-3+ hours | Approximately 20 minutes per disc |
| Recovery timeline | Weeks to months | Ambulatory within hours, same-day discharge |
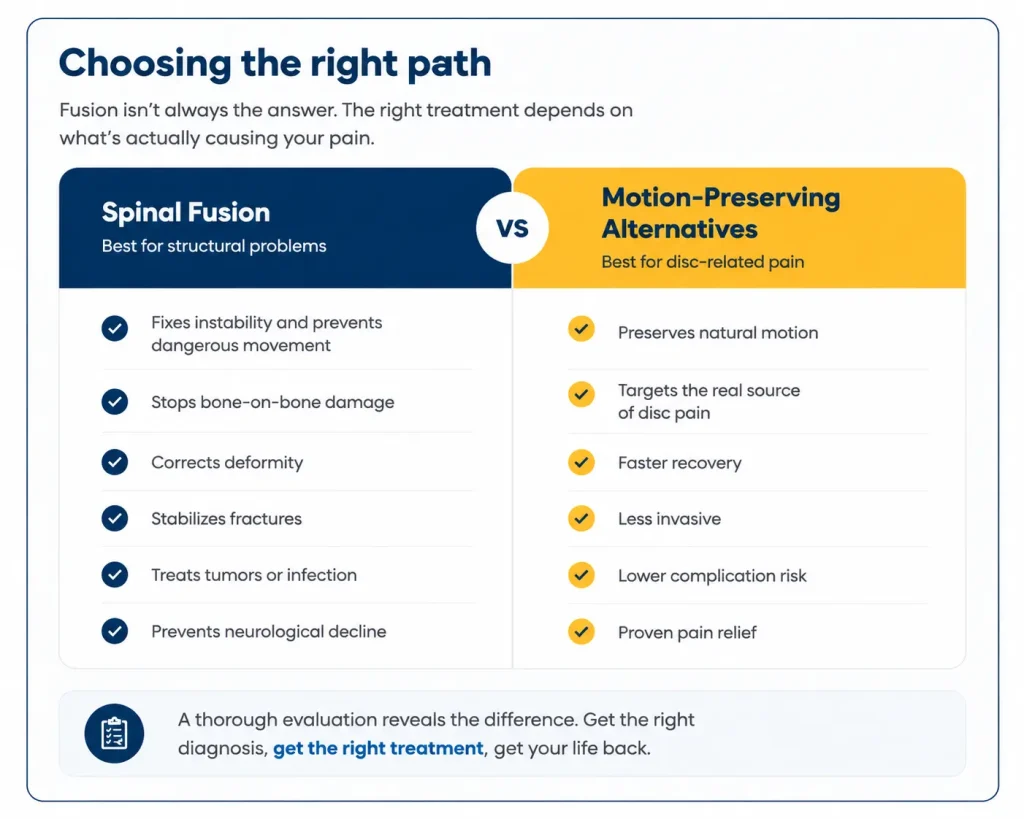
When Laminectomy Is Appropriate and When It Is Not
This is not an argument that lumbar laminectomy should never be performed. For a patient whose primary complaint is neurogenic claudication, with imaging-confirmed severe stenosis and minimal axial back pain, laminectomy may be the right intervention. Decompressing a severely compressed cauda equina or nerve root producing progressive leg weakness is appropriate and sometimes urgent.
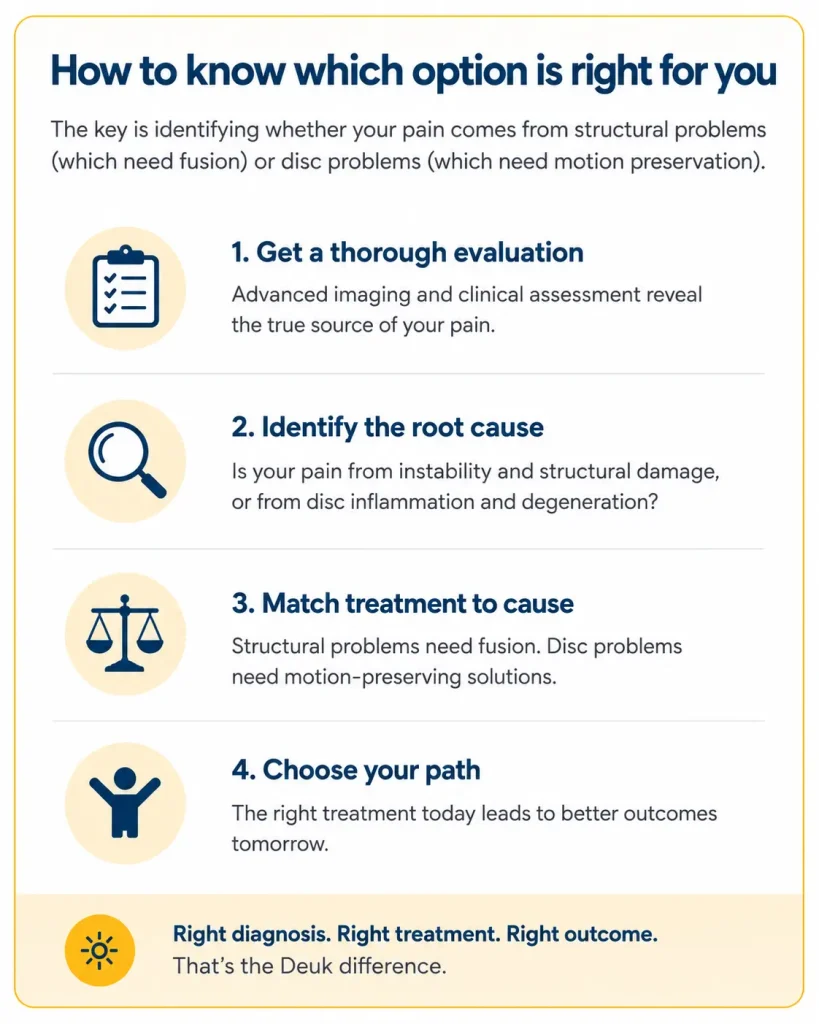
The concern is with the much larger population of patients who have both stenosis and disc pathology, or whose primary complaint is axial back pain, and who are offered laminectomy as the answer to both. For those patients, the stenosis finding on MRI becomes the surgical target while the disc, which may be the dominant pain driver, is left untreated.
A thorough diagnostic process separates these two groups. The Deuk Spine Exam® uses MRI findings, dermatomal sensory testing, and detailed symptom history to confirm which structure is generating the pain before any surgical recommendation is made. This is how patients get lasting relief rather than partial results that fade.
If you have been recommended for lumbar laminectomy and your primary complaint is back pain rather than leg symptoms, confirm that the proposed surgery targets the actual source of your pain. You can learn more about laminectomy alternatives and what those options treat that bone removal alone does not.
Patients preparing for a conversation about their L4-L5 or L5-S1 levels specifically will find additional clinical detail in our article on L4-L5 disc pathology and treatment options and in the overview of the Deuk Laser Disc Repair® procedure. For patients evaluating the risks of fusion as a potential follow-up to laminectomy, our article on spinal fusion complications covers what the evidence shows.
The Right Question Before Any Lumbar Spine Surgery
The question every patient should ask before consenting to lumbar laminectomy is whether this surgery treats the structure actually generating the pain.
Back pain and leg symptoms are different problems with different sources. Canal narrowing on MRI is not automatically the cause of back pain. Removing the bone relieves compression but leaves disc inflammation untreated, and disc inflammation drives back pain in approximately 85% of chronic cases. A surgery that does not address 85% of the problem will not produce complete relief.
At Deuk Spine Institute, we offer free MRI reviews so patients can understand what their imaging actually shows, which structures may be pain generators, and whether the proposed treatment matches the diagnosis. Patients travel from across the country and internationally for this evaluation because getting the diagnosis right is what makes treatment work.
If you are living with chronic lumbar back pain and have been recommended for laminectomy, request your free MRI review with the Deuk Spine Exam® before moving forward. Understanding your pain source is the first step toward eliminating it.
This content is provided for educational purposes only. It does not constitute medical advice, diagnosis, or a recommendation for any specific treatment. Individual results vary. Outcomes with Deuk Laser Disc Repair® apply to patients whose confirmed pain source matches the treated pathology. Consult a qualified spine specialist to determine what treatment is appropriate for your condition.


