

Your surgeon just told you that you need a laminectomy or maybe a laminotomy, and now you’re staring at two words that sound almost identical, trying to figure out what’s actually going to happen to your spine. That confusion is common, and it matters, because these two procedures are not the same operation, and neither one may actually solve the pain that sent you looking for answers in the first place.
Most patients arrive at this decision after months, sometimes years, of physical therapy, injections, and medication that never quite got rid of the pain. By the time a surgeon mentions laminectomy or laminotomy, you’ve usually already done everything else you were told to try. You deserve a clear answer about what these procedures actually do, and an honest look at whether either one, or a motion-preserving alternative like Deuk Laser Disc Repair®, will address the problem you’re actually dealing with.
I’ve spent over 30 years as a board certified neurosurgeon treating patients with exactly this confusion. I know this because it comes up in nearly every consultation with a patient who was referred for spinal stenosis or a herniated disc. So let’s clear up the laminotomy vs laminectomy question directly, and then let’s talk about something most surgeons won’t bring up. Removing bone from your spine might relieve one type of pain while leaving the real source of your suffering completely untouched.

No cost · No obligation
Live Pain Free
Upload your MRI for a free expert review by Dr. Ara Deukmedjian, M.D. — board-certified neurosurgeon. Ten minutes can change your life.
What Is a Laminectomy?
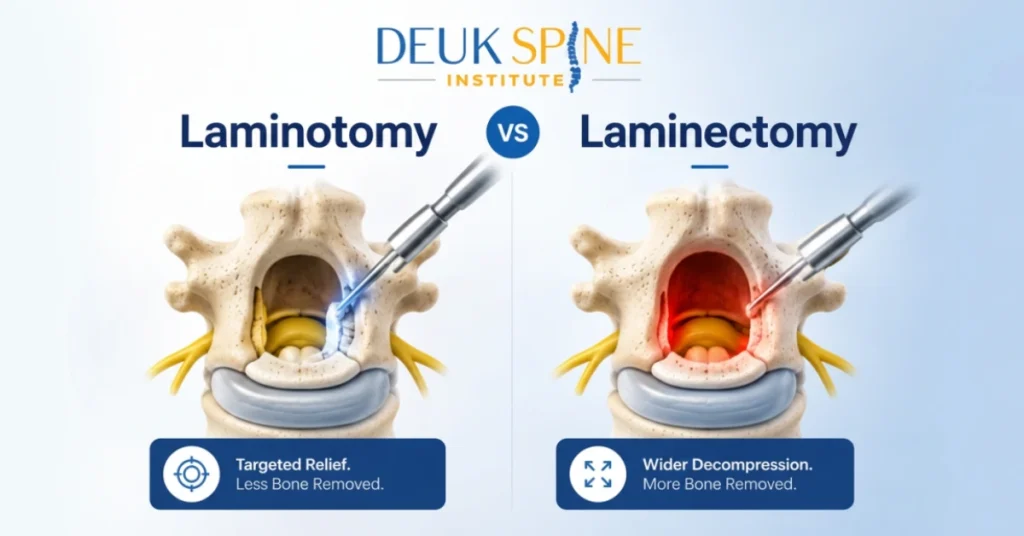
The lamina is the bony arch on the back of each vertebra. It forms part of the protective ring around your spinal cord and nerves. A laminectomy removes that bony arch, either partially or completely, at one or more spinal levels.
Surgeons perform this procedure most often for spinal stenosis, a narrowing of the spinal canal that squeezes the nerves running through it. By removing the lamina, the surgeon opens up space and takes pressure off the compressed nerves.
A traditional laminectomy is an open surgery. The surgeon makes a larger incision, moves muscle tissue aside, and removes bone directly. Recovery typically means a hospital stay of one to three days, followed by weeks or months of restricted activity while the muscles and remaining bone structure heal.
What Is a Laminotomy?
A laminotomy is a smaller, more targeted version of the same basic idea. Instead of removing the entire lamina, the surgeon removes only a portion of it, just enough to create a window that relieves pressure on the specific nerve or disc causing the problem.
This procedure is common when a herniated disc fragment needs to be removed (a discectomy) or when a smaller section of bone is pinching a single nerve root. Because less bone comes out, laminotomy generally involves a smaller incision and a faster initial recovery than a full laminectomy.
Laminotomy vs Laminectomy, the Real Differences
Patients often ask me to boil this down into plain terms, so here’s how I explain it during consultations.
| Factor | Laminectomy | Laminotomy |
|---|---|---|
| Amount of bone removed | Entire lamina at the affected level | Only a portion, leaving more natural bone intact |
| Typical use case | Broader spinal stenosis affecting multiple levels or the central canal | A single, localized problem such as a disc fragment pressing on one nerve root |
| Incision and approach | Larger open incision | Smaller opening, though still typically an open bone removal procedure |
| Recovery expectations | Hospital stay, longer road back to normal activity | Shorter recovery, but still measured in weeks |
| Spinal stability afterward | Higher risk of instability, sometimes requiring a later fusion | Lower risk of instability due to less bone removed |
Both procedures share one thing in common that patients rarely hear until after they’ve already scheduled surgery. They decompress a nerve. They do not repair a disc, and they do not eliminate the underlying source of chronic back pain.
Why Neither Procedure May Be Your Best Option
Here’s the distinction I wish more patients understood before they consent to either surgery. Nerve compression, the kind a laminectomy or laminotomy is designed to relieve, causes leg symptoms. A burning, shooting, electric sensation that travels down a specific nerve path. Numbness or weakness in a particular pattern. That’s radicular pain, and it’s driven largely by inflammation and pressure on the nerve itself.
Axial back pain, the deep, localized ache that stays in your back, is a different problem entirely. In my clinical experience treating patients across three decades, the majority of chronic back pain traces back to inflammation inside a torn disc or an irritated facet joint, not to a nerve being pinched.
So if your main complaint is leg pain from a compressed nerve, a laminectomy or laminotomy may genuinely help. But if you also have chronic back pain, and most patients referred for these procedures do, removing bone to decompress a nerve won’t touch that back pain at all. You may wake up from surgery with less leg pain and the exact same back pain you walked in with.
There’s also the bone removal itself to consider. Your lamina and facet joints provide structural support for your spine. Taking away that bone, especially in a full laminectomy, changes the mechanics of the segment. Some patients develop new instability months or years later, sometimes requiring a second surgery, often a fusion, to stabilize what the first operation left unsupported. I go into more depth on this trade-off in my breakdown of what a lumbar laminectomy does and doesn’t fix.
I’ve reviewed thousands of MRIs from patients considering these procedures, and a pattern shows up again and again. The imaging clearly shows nerve compression, which explains the leg pain. But the same scan often shows a degenerated, torn disc or arthritic facet joint sitting right next to that compressed nerve, the actual source of the back pain the patient has been living with for years. A laminectomy or laminotomy will open space around the nerve. It will not touch the torn disc or the arthritic joint sitting a few millimeters away.
What Actually Causes Most Chronic Back Pain
Through years of clinical practice and diagnostic refinement, I’ve identified that the disc itself is usually the true source of chronic axial back pain, specifically a tear in the back wall of the disc called the posterior annular tear. When the soft nucleus pulposus material pushes into that tear, it triggers ongoing inflammation. Over time, small pain fibers grow into the damaged tissue, and the pain becomes chronic.
Facet joints can develop a nearly identical problem. An injury to the joint capsule causes a tear, inflammation sets in, and the pain becomes chronic in the same way. I cover how these different pain generators show up and get diagnosed in my guide to the four main types of chronic back pain. For a general overview of what a standard laminectomy involves from a purely surgical standpoint, Cleveland Clinic’s patient resource is a solid reference.
Neither a laminectomy nor a laminotomy addresses this tear or the inflammation inside it. They’re designed to make room for a nerve, not to treat a damaged disc or joint. That’s an important distinction, and it’s one reason so many patients tell me they had “successful” decompression surgery and still hurt.
A Motion-Preserving Alternative Worth Understanding
I developed Deuk Laser Disc Repair® specifically to treat the disc injury at its source rather than simply decompressing a nerve around it. The procedure removes the inflamed tissue from the annular tear and performs a debridement, allowing the tear to heal naturally over time, without cadaver bone, metal hardware, or plastic implants. There’s no bone drilling involved, which means the spine’s natural stability stays intact.
For facet joint pain, Deuk Plasma Rhizotomy® works on the same principle, addressing the nerves responsible for transmitting pain from the damaged joint capsule in a 30 minute outpatient procedure.
I’ve performed over 2,700 Deuk Laser Disc Repair® procedures, and patients report an average of 99% pain relief for the disc sources we treat, with a complication rate of 0.01%. Most patients walk within an hour of finishing surgery and go home the same day, a stark contrast to the hospital stay and extended recovery that often follows a traditional laminectomy.
None of this means laminectomy or laminotomy is never appropriate. When a large central disc herniation or severe stenosis is putting a nerve at genuine risk, decompression can be necessary and even urgent. But if your pain is primarily coming from the disc or facet joint itself, treating that source directly, rather than just making room around it, gives you a real chance at ending the pain instead of just moving it. You can compare how each surgical and non-surgical option stacks up on our spine treatment options page.
Questions Patients Ask Me About Laminotomy vs Laminectomy
Which procedure has a faster recovery?
Laminotomy typically has a shorter recovery than a full laminectomy because less bone is removed and the surgical footprint is smaller. Even so, patients usually need several weeks before returning to normal activity.
Will a laminectomy fix my back pain?
A laminectomy is built to relieve pressure on a compressed nerve, which mainly affects leg symptoms. If your back pain comes from a disc or facet joint issue rather than nerve compression, a laminectomy alone likely won’t resolve it.
Do I need a fusion after a laminectomy?
Not always. It depends on how much bone is removed and how many levels are involved. Removing larger amounts of bone, particularly at multiple levels, increases the chance that a fusion will eventually be recommended to restore stability.
Is there a way to treat a herniated disc without removing bone?
Yes. Deuk Laser Disc Repair® treats the annular tear and inflammation directly, without drilling or removing the surrounding bone, which helps preserve the spine’s natural stability.
How do I know if my pain is coming from a nerve, a disc, or a joint?
The pattern of symptoms is the biggest clue. Leg pain that follows a specific path, along with numbness or weakness in a defined area, usually points to nerve compression. A deep, localized ache that stays in the back, especially one that worsens with sitting or bending, more often points to a disc or facet joint problem. An MRI combined with a careful physical exam and pain history, what I use in the Deuk Spine Exam®, gives a 99% accurate answer rather than a guess.
Get a Second Opinion Before You Commit to Surgery
If you’ve been told a laminectomy or laminotomy is your only path forward, it’s worth understanding exactly what that surgery will and won’t fix before you schedule it. Ask your surgeon directly whether your primary complaint is leg pain, back pain, or both, and whether the proposed procedure is designed to address the specific source of each. If the answer only covers the nerve compression, you still deserve a plan for the pain in your back.
I offer a free MRI review so you can find out whether your pain is coming from nerve compression, a disc injury, a facet joint, or some combination, and what your actual treatment options look like. There’s no obligation, just clarity about what’s really happening in your spine and the most direct path toward ending your pain rather than just managing it. You’ve already spent enough time trying treatments that didn’t get to the source. Let’s find out what will.
Diagnosis. Answers. Relief.
Submit your MRI for a free expert review by Dr. Ara Deukmedjian, M.D. —
board-certified neurosurgeon. No obligation. Real answers.


