


By Dr. Ara Deukmedjian
Board-Certified Neurosurgeon
Medically reviewed on May 13, 2026
Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
Key Points
✓ Yes, patients can absolutely get worse after spine surgery. Published research estimates that between 10% and 40% of traditional spine surgery patients develop Failed Back Surgery Syndrome (FBSS). 1
✓ FBSS is most commonly caused by inaccurate preoperative diagnosis, epidural fibrosis (scar tissue around the nerves), adjacent segment disease after fusion, recurrent disc herniation, and direct surgical nerve injury. 2
✓ Revision spine surgery has steeply declining odds of success: roughly 50% on the first surgery, 30% on the second, 15% on the third, and 5% on the fourth. 3
✓ As much as 58% of FBSS cases trace back to undiagnosed lateral stenosis of the lumbar spine. A structural problem the original surgery never addressed. 2
✓ Deuk Laser Disc Repair® treats the actual pain generator through a 4mm to 7mm incision with no muscle cutting, no bone removal, and no hardware. Eliminating the surgical trauma that causes FBSS in the first place.
Yes, Patients Get Worse After Spine Surgery, and It Has a Name
One of the most painful conversations in a spine clinic happens when a patient sits down, points to their scar, and says, “I’m worse than I was before.” They followed every instruction. They did the physical therapy. They took the medications. They consented to the surgery their doctor recommended. And now they hurt more, move less, and have lost faith in the system that put them there.
This is not rare. It is not “in their head.” It is a recognized medical condition called Failed Back Surgery Syndrome (FBSS), sometimes referred to as post-laminectomy syndrome or post-surgical spine syndrome. The International Association for the Study of Pain defines FBSS as lumbar spinal pain of unknown origin either persisting despite surgical intervention or appearing after surgical intervention for spinal pain originally in the same topographical location.4 9
Multiple large studies place the incidence of FBSS at 10% to 40% of all traditional spine surgeries. 1 2 For laminectomy specifically, national data place the rate between 10% and more than 40% of patients, and patients with post-laminectomy syndrome have a relative risk of requiring reoperation that is 6.14 times higher than those without postoperative back pain. Compared with other chronic conditions such as rheumatoid arthritis, FBSS produces lower quality of life and higher rates of disability and unemployment. 5 In other words, a failed spine surgery can be more disabling than the disease it was meant to treat.
What Failed Back Surgery Syndrome Actually Is

FBSS is not a single diagnosis. It is a syndrome. An umbrella term covering any situation where the patient continues to have chronic pain, develops new pain, or loses function after spine surgery. 7 Symptoms can include:
- Persistent or worsening low back pain in the same location as before surgery
- New back or leg pain that did not exist before the operation
- Radiating sciatica, burning, or numbness down the legs
- Foot drop or weakness, often from L5 nerve root injury or compression Reduced mobility, stiffness, and inability to return to work 7
- Dependence on opioid medications for daily function
- Depression, anxiety, and loss of independence tied to chronic pain
The pain can show up immediately after surgery, in the weeks of recovery, or years later as adjacent levels of the spine break down from carrying the load of a fused or destabilized segment. 7
Why Does Spine Surgery Fail? The Real Causes of FBSS

Spine surgery does not fail because patients did something wrong. It fails because of identifiable medical and surgical causes that often trace back to the decisions made before the patient ever entered the operating room.
1. Inaccurate Preoperative Diagnosis
This is the single largest driver of FBSS. Peer-reviewed research has shown that up to 58% of FBSS cases trace back to undiagnosed lateral stenosis of the lumbar spine.² A structural problem the original surgery never addressed. If the surgeon does not correctly identify which structure is generating the pain, the operation removes the wrong tissue and leaves the actual pain generator in place. The patient wakes up with a surgical wound and the original pain.
2. Epidural Fibrosis (Scar Tissue Around the Nerves)
Open spine surgery, including laminectomy, microdiscectomy, and fusion, requires cutting through muscle, removing bone, and manipulating the nerves. The body responds to that trauma by laying down dense scar tissue (epidural fibrosis) around the nerve roots. 6 This scar tissue tethers the nerves, restricts their natural movement, and produces a chronic burning, shooting pain that is often worse than the original symptoms. Epidural fibrosis is one of the most common causes of FBSS and one of the hardest to treat once it forms. 6
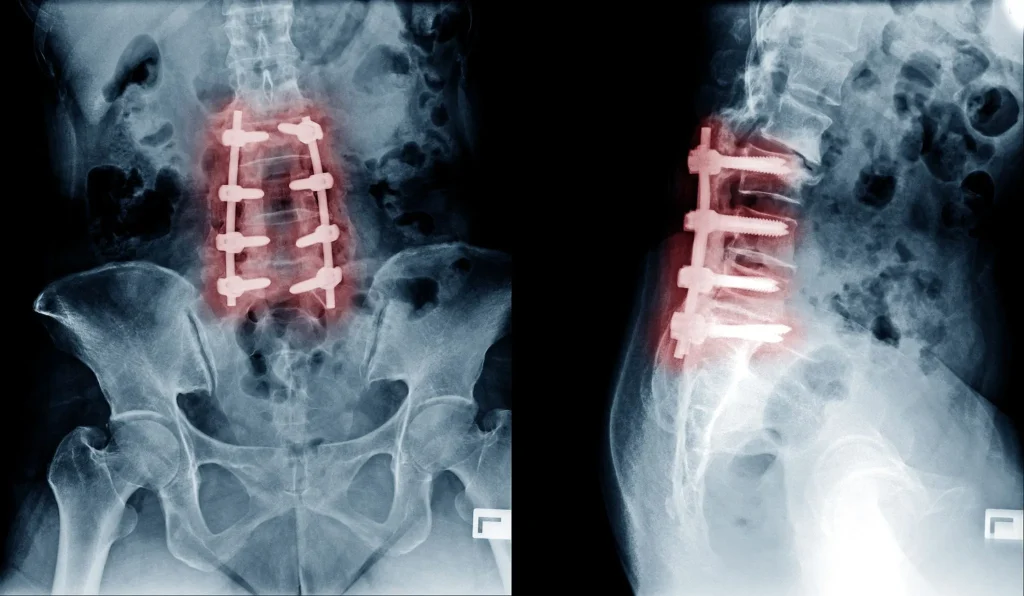
3. Adjacent Segment Disease (ASD)
When vertebrae are fused, the spinal segments above and below the fusion are forced to absorb extra motion and stress. Over time, those adjacent levels degenerate at an accelerated rate, producing new disc herniations, new stenosis, and new pain. 6 Adjacent segment disease is one of the most documented long-term consequences of lumbar fusion and a leading reason patients return to the operating room years after their original “successful” surgery.
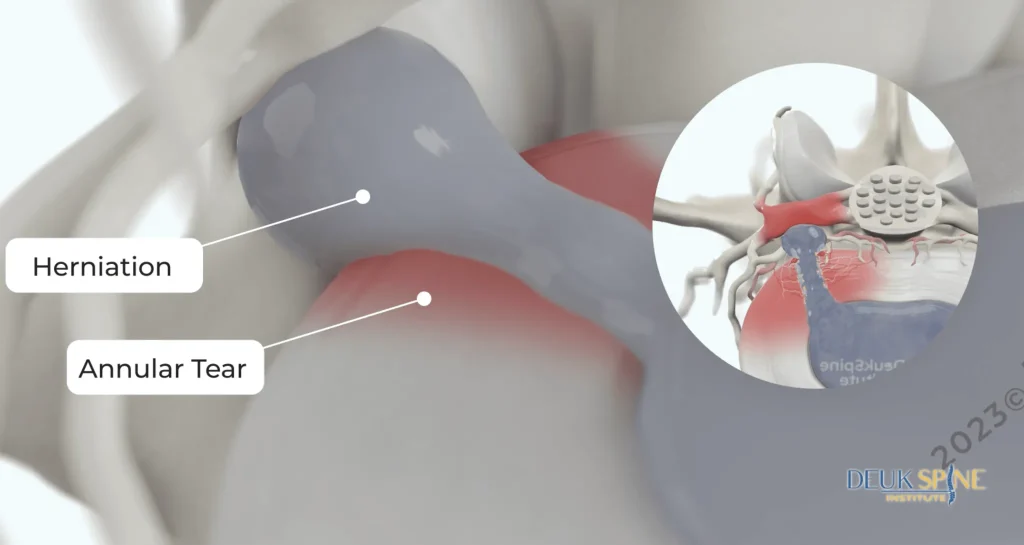
4. Recurrent Disc Herniation
After a traditional microdiscectomy, the disc itself is not repaired. A window is cut into the annulus and the herniated piece is removed, but the tear remains open. In a significant percentage of patients, the disc re-herniates through that same defect. Sometimes within weeks, sometimes years later. 7
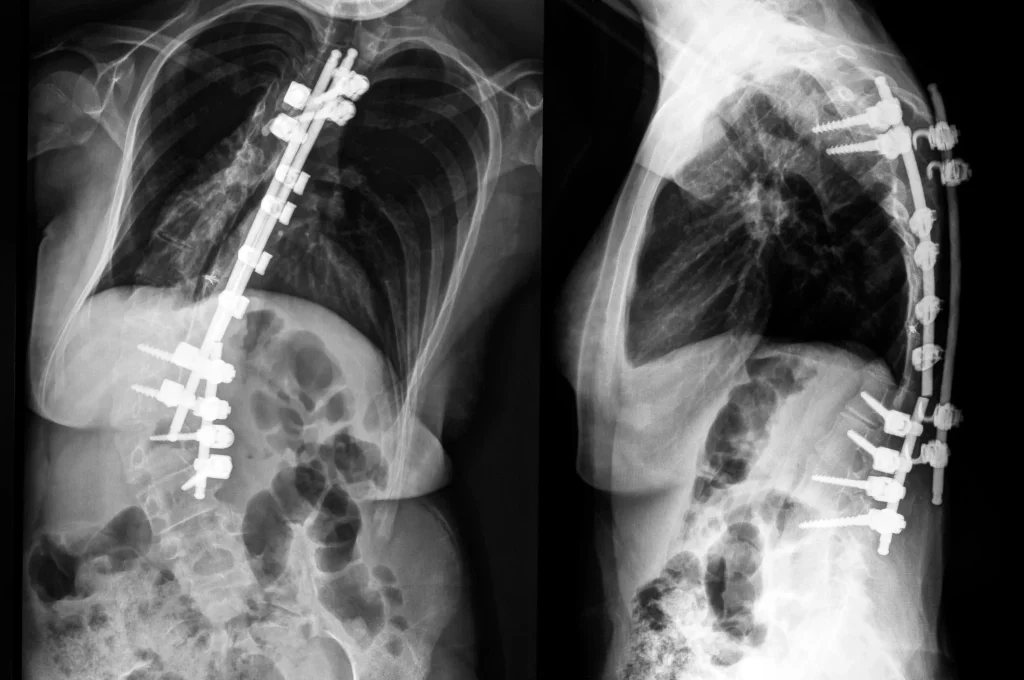
5. Hardware Failure
Fusion relies on screws, rods, plates, and cages. These implants can loosen, migrate, fracture, or pull out of the bone. When that happens, patients develop new mechanical pain and often need revision surgery to remove or replace the hardware. 6
6. Iatrogenic Nerve Injury
Direct trauma to a nerve root during surgery from retraction, drilling, or manipulation can produce permanent neurologic deficits. Foot drop, persistent radicular pain, and chronic numbness are well-documented complications of traditional open spine procedures. 7
7. Pseudarthrosis (Failed Fusion)
In a fusion, the vertebrae are supposed to grow together into one solid bone over 6 to 12 months. When the bone graft fails to fuse, the construct is unstable, and the patient is left with hardware, motion at a level that was supposed to be locked, and pain.6
8. Wrong Procedure for the Pain Generator
A fusion cannot fix an inflamed annular tear. A laminectomy cannot fix a facet joint. A discectomy cannot fix instability. Recommending the wrong operation for the wrong pain source guarantees a poor outcome, and it is the single most preventable cause of FBSS. 2
The Brutal Math of Revision Surgery
Patients with FBSS are often told the answer is another surgery. The published data on revision spine surgery is sobering. A review article in the Asian Spine Journal documented the following declining success rates: 3

- First spine surgery: up to 50% success
- Second spine surgery: up to 30% success
- Third spine surgery: up to 15% success
- Fourth spine surgery: up to 5% success
Each repeat operation involves cutting through more scar tissue, removing more bone, and creating more fibrosis. The odds get worse with every attempt.
Patients with FBSS also face a documented risk that is often left out of the conversation. One peer-reviewed analysis found that opioid overdose was the most common cause of death following lumbar fusion surgery. 7 When pain persists after surgery, the prescription cascade that follows can become more dangerous than the original condition.
This is why the goal at Deuk Spine Institute is not to do “better” failed back surgery. The goal is to avoid causing FBSS in the first place. And when a patient already has it, to treat the actual pain generator with the least invasive procedure possible.
Who Is Most at Risk of FBSS?

Research has consistently identified the patient populations most likely to develop Failed Back Surgery Syndrome. A 2022 analysis using a national insurance database found the highest rates of FBSS occurred in: 8
- The elderly, particularly the 70–74 age group
- Patients receiving their procedure in an inpatient setting rather than outpatient
- Patients undergoing multi-level surgery rather than single-level procedures
- Patients with decompression and posterior lumbar fusion procedures
Additional preoperative risk factors documented in the literature include inadequate diagnostic workup, smoking (which impairs bone healing and increases pseudarthrosis rates), and untreated psychological comorbidity such as depression and anxiety. 2 10
If you fall into any of these categories and a surgeon has recommended a large open operation, a second opinion is not optional. It is essential.
How FBSS Is Diagnosed
Show Image
Diagnosing the cause of FBSS is more important than diagnosing FBSS itself, because the syndrome is just a description. The cause is what determines treatment. 2 A proper workup includes:
- Detailed history of the original pain, the original surgery, what changed, and what triggers symptoms now
- Physical examination to localize pain, identify weakness, test reflexes, and check for instability
- Updated MRI to look for recurrent herniation, scar tissue, adjacent segment disease, foraminal stenosis, and pseudarthrosis
- CT scan when hardware needs to be evaluated or fusion status confirmed
- Diagnostic injections to confirm which specific structure is generating pain
At Deuk Spine Institute, we use the Deuk Spine Exam®, which combines detailed clinical evaluation with imaging review to identify the true pain generator. Without that step, any treatment plan is a guess.
Treatment Options for Failed Back Surgery Syndrome
Treatment depends entirely on the cause. There is no single procedure that “fixes” FBSS as a category. Conservative management is generally recommended before any invasive technique in patients without indications for emergency surgery, and the options fall broadly into four tiers. 6
Conservative and Pain Management
- Physical therapy aimed at core stabilization and gentle mobilization
- NSAIDs and non-opioid medications
- Targeted epidural steroid injections
- Medial branch blocks and radiofrequency ablation for facet pain
- Spinal cord stimulation (SCS) for neuropathic pain that has not responded to other measures
These approaches manage symptoms but do not repair the structural problem causing them. 7 They have a role, but they are not a cure when there is an identifiable, treatable pain generator.
Targeted Minimally Invasive Procedures
When the cause of FBSS is a specific structural problem (a recurrent disc herniation, an untreated annular tear, foraminal stenosis, or facet-mediated pain) a precise, motion-preserving procedure can address it without repeating the trauma of the original operation:
- Deuk Laser Disc Repair® for residual or recurrent disc pathology, performed through a 4mm to 7mm incision with no hardware and no bone removal.
- Deuk Plasma Rhizotomy® for facet joint and SI joint pain, which is a frequent and under-recognized source of pain after lumbar fusion.
- Endoscopic decompression for foraminal stenosis at the original level or at an adjacent segment that has degenerated.
A 2024 systematic review in the European Spine Journal found that full-endoscopic discectomy produced outcomes comparable to or better than traditional open microdiscectomy with significantly less tissue trauma. 10 The clinical principle is straightforward: less surgical trauma means less of the fibrosis and instability that drives FBSS.
Revision Surgery (When Truly Required)
Revision fusion or hardware removal is sometimes necessary for pseudarthrosis, broken hardware, or true mechanical instability. But the bar should be high. The declining success rate of repeat surgery is not a marketing slogan. It is published data, and patients deserve to know it before they consent. 3
How to Avoid FBSS in the First Place
The best treatment for Failed Back Surgery Syndrome is not having it. Avoiding the initial development of FBSS may, in fact, be the most effective way of reducing the condition’s burden on patients. 7 Before consenting to spine surgery, every patient should be able to answer the following:
- What specific structure on my MRI is generating my pain?
- How was that pain generator confirmed: physical exam, imaging correlation, diagnostic injection?
- What is the least invasive procedure that can treat that specific structure?
- What is the surgeon’s documented complication rate, infection rate, and reoperation rate?
- What are the motion-preserving alternatives to the procedure being recommended?
- What happens if I do nothing for 6 more months?
If a surgeon cannot answer these questions with specifics, the recommended procedure is not ready to be performed. Hardware cannot be unscrewed. Fused vertebrae cannot be unfused. The removed bone does not grow back. The first surgery is the one most likely to succeed, 3 which is also why it is the one most worth getting right.
The Deuk Spine Approach to Patients With FBSS
A meaningful portion of the patients who come to Deuk Spine Institute have already had at least one spine surgery somewhere else. They arrive frustrated, in pain, and skeptical that anything will help. Our approach is simple:
- Re-image and re-diagnose. We do not assume the original diagnosis was correct. The MRI is reviewed in detail, and the pain generator is identified using the Deuk Spine Exam®.
- Identify what is treatable. Some FBSS is from scar tissue and central sensitization, which requires pain management. Much of it, however, comes from a specific structure that can still be repaired. A residual disc herniation, an untreated facet, an adjacent segment.
- Choose the least invasive option that addresses the real problem. When the source is a disc or facet, theDeuk Laser Disc Repair® or Deuk Plasma Rhizotomy® can treat it without repeating the trauma that caused the original failure.
- Be honest about what cannot be undone. Fused segments stay fused. Removed bone stays gone. We are direct about what is and is not fixable, because patients who have already failed once deserve straight answers.
When to Seek Medical Attention
| Level of Care | Symptoms |
|---|---|
| See a Specialist Spine specialist evaluation Schedule a consultation |
|
| Emergency Go to the ER immediately Possible cauda equina syndrome. A surgical emergency that cannot wait |
|
The Bottom Line
Yes, patients can absolutely get worse after spine surgery, and a large body of peer-reviewed medical literature confirms it. 1 2 6 Failed Back Surgery Syndrome is not a rare event, not a character flaw, and not something patients should be asked to “just live with.” It is most often the predictable downstream consequence of either the wrong diagnosis or the wrong procedure performed on the right diagnosis. 2
The good news is that for most patients, the original injury is still treatable. Often by a much less invasive procedure than the one that failed them. A precise diagnosis, an honest conversation about alternatives, and a procedure that targets the actual pain generator rather than the whole spinal segment is what separates lasting relief from another failed surgery.
If you or a loved one is living with pain after a previous spine surgery, submit your MRI for a free virtual consultation. Dr. Deukmedjian will personally review your imaging and explain what is causing your pain and whether a minimally invasive option can finally fix it.
Frequently Asked Questions
Has anyone actually gotten worse after spine surgery?
Yes. Studies estimate that between 10% and 40% of patients undergoing traditional spine surgery develop Failed Back Surgery Syndrome, meaning their pain persists or worsens after the operation. 1 2 This is not a rare complication. It is one of the most common reasons patients seek second-opinion spine consultations.
What is Failed Back Surgery Syndrome?
The International Association for the Study of Pain defines FBSS as lumbar spinal pain of unknown origin either persisting despite surgical intervention or appearing after surgical intervention for spinal pain in the same topographical location. 4 It is not a single condition but an umbrella term covering many causes.
What are the most common causes of FBSS?
The leading causes are inaccurate preoperative diagnosis (especially missed lateral stenosis, which accounts for as much as 58% of cases), epidural fibrosis from open surgical trauma, adjacent segment disease after fusion, recurrent disc herniation, hardware failure, pseudarthrosis (failed fusion), and direct nerve injury during surgery. 2 6 7
Can FBSS be fixed?
Often, yes, but it depends on the cause. Structural problems like a recurrent disc herniation, an untreated facet joint, or an adjacent segment disc can frequently be treated with targeted minimally invasive procedures. Diffuse pain from scar tissue and central sensitization is harder to reverse and is usually managed rather than cured. 6
Is more surgery the answer to a failed surgery?
Usually not. Each successive revision surgery has lower odds of success. Roughly 50%, 30%, 15%, and 5% for the first, second, third, and fourth operations respectively. 3 More invasive surgery on an already-traumatized spine compounds the problem. A precise minimally invasive procedure targeting the true pain generator is almost always preferable to another large open operation.
How long after spine surgery does FBSS show up?
It varies. Some patients wake up from surgery already worse. Others develop new pain in the weeks of recovery as nerve irritation and scar formation evolve. Adjacent segment disease often appears years after a fusion as the levels above and below break down under the added stress. 8
Can Deuk Laser Disc Repair® help patients with FBSS?
In many cases, yes. When the cause of ongoing pain is a residual or recurrent disc problem, Deuk Laser Disc Repair® can treat the disc through a 4mm to 7mm incision without removing bone, cutting muscle, or implanting hardware. Candidacy depends on the specific findings on MRI and what the original surgery did.
How do I find out if I have Failed Back Surgery Syndrome?
The first step is having an updated MRI reviewed by a spine surgeon experienced in motion-preserving and endoscopic procedures. Not only by the surgeon who performed the original operation. Submit your MRI for a free virtual consultation with Dr. Deukmedjian to find out what is generating your pain and which options remain.
Sources
- Risk factors analysis and risk prediction model for failed back surgery syndrome: A prospective cohort study. PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1175558/
- Baber Z, Erdek MA. Failed back surgery syndrome: current perspectives. Journal of Pain Research. https://pmc.ncbi.nlm.nih.gov/articles/PMC5106227/
- Daniell JR, Osti OL. Failed Back Surgery Syndrome: A Review Article. Asian Spine Journal. 2018;12(2):372-37. https://pubmed.ncbi.nlm.nih.gov/2713421/
- Orhurhu VJ, Chu R, Gill J. Failed Back Surgery Syndrome. StatPearls Publishing, National Library of Medicine. https://www.ncbi.nlm.nih.gov/books/NBK53777/
- Ampat G, George JS, Clynch AL, Sims JMG. Spinal fusion surgery: the need to follow the ‘BRAN’ toolkit. Journal of Surgical Case Reports. 2022. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4186/
- Orhurhu VJ, Chu R, Gill J. Failed Back Surgery Syndrome. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK53777/
- Failed Back Surgery Syndrome (FBSS): What It Is and How to Avoid Pain after Surgery. Spine-Health. https://www.spine-health.com/treatment/back-surgery/failed-back-surgery-syndrome-fbss-what-it-and-how-avoid-pain-after-surgery
- The incidence of failed back surgery syndrome varies between clinical setting and procedure type. Clinical Neurology and Neurosurgery. 2022. https://pubmed.ncbi.nlm.nih.gov/35810607/
- Prevalence of Chronic Pain After Spinal Surgery: A Systematic Review and Meta-Analysis. PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10423077/
- Full-endoscopic versus microscopic lumbar discectomy for lumbar disc herniation: a systematic review and meta-analysis. European Spine Journal. 2024. https://pubmed.ncbi.nlm.nih.gov/4151230/


