


By Dr. Ara Deukmedjian, MD
Board-Certified Neurosurgeon, Deuk Spine Institute
Medically reviewed on January 27, 2026
Medical disclaimer:This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
If you’re a woman in your 40s, 50s, or 60s experiencing new or worsening back pain, you might wonder if menopause is playing a role. The answer is almost certainly yes. The hormonal shifts that occur during menopause don’t just cause hot flashes and mood changes; they fundamentally alter your spine health, affecting everything from your bones to your intervertebral discs to your risk of debilitating fractures.
Here’s what might surprise you: the connection between menopause and spine health goes far deeper than most people realize. While osteoporosis and bone loss are well-known consequences of declining estrogen, recent research reveals that menopausal hormone fluctuations are also associated with intervertebral disc degeneration, facet joint osteoarthritis, increased inflammation, and changes in how your body experiences and processes pain.1 Women can lose up to 20% of their bone mass in the first five to seven years after menopause, significantly heightening fracture risk and creating a cascade of spinal changes that can affect quality of life for decades.
This comprehensive guide will walk you through everything you need to know about how menopause affects your spine, from the underlying hormonal mechanisms to practical steps you can take to protect your spine health. Whether you’re approaching menopause, currently experiencing symptoms, or years past this transition, understanding these connections can help you make informed decisions about your care and take proactive steps to maintain a healthy, pain-free spine.
Understanding the Menopause-Spine Connection: What's Really Happening in Your Body
Menopause marks the end of a woman’s reproductive years, typically occurring around age 50, though it can happen earlier or later. The years leading up to menopause (perimenopause) and the years following (postmenopause) bring dramatic hormonal changes that ripple throughout the body, and your spine is particularly vulnerable to these shifts.
The Role of Estrogen in Bone and Spine Health
Estrogen is the key regulator of bone metabolism in both women and men. It performs several critical functions for bone health:
- Promotes production of osteoprotegerin, a protein that prevents excessive bone breakdown
- Enhances osteoblast (bone-building cell) survival and function through the Wnt signaling pathway
- Reduces production of pro-inflammatory cytokines (IL-1, IL-6, TNF-α) that accelerate bone resorption
- Maintains the balance between bone formation and bone resorption
- Preserves disc height and nutrient diffusion to intervertebral discs
When estrogen levels plummet during menopause, this protective effect vanishes. Research has consistently shown that estrogen deficiency accelerates bone resorption through a rise in pro-inflammatory cytokines and RANKL (receptor activator of nuclear factor kappa-B ligand), which promote osteoclastogenesis; the formation of cells that break down bone tissue.2 This imbalance between bone breakdown and bone formation is the fundamental mechanism behind postmenopausal osteoporosis.
A landmark study examining postmenopausal women found that those with undetectable serum estradiol concentrations (less than 5 pg/mL) had a relative risk of 2.5 for subsequent hip fracture and vertebral fracture compared to women with detectable estradiol levels.3 This association remained significant even after adjusting for age and weight, underscoring the direct protective effect of estrogen on bone integrity.
The Cascade of Spinal Changes During Menopause
The impact of estrogen deficiency on spine health extends beyond simple bone loss. Recent comprehensive research published in January 2026 highlights that menopausal hormone fluctuations are associated with multiple interconnected spinal changes:1
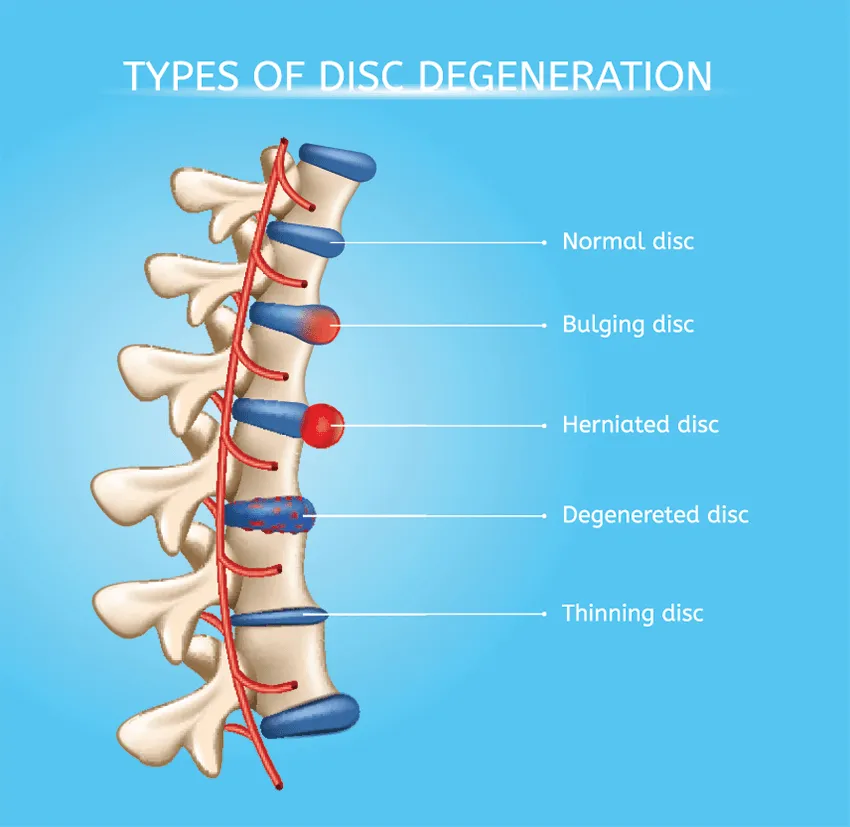
- Intervertebral disc degeneration: Estrogen receptors are present in disc tissue, and estrogen deficiency impairs nutrient diffusion to discs and accelerates degradation of the nucleus pulposus (the gel-like center of the disc)
- Facet joint osteoarthritis: The small joints between vertebrae show accelerated wear and tear
- Ligamentum flavum hypertrophy: Thickening of the ligaments in the spine that can contribute to spinal stenosis
- Sarcopenia: Loss of muscle mass and strength, reducing the spine’s natural support system
- Sympathetic innervation alterations: Changes in nerve function that can amplify pain perception
- Systemic inflammation: Increased inflammatory markers throughout the body that exacerbate pain
Research from multiple studies confirms that women, despite having fewer traditional risk factors for disc degeneration than men, actually experience more severe disc degeneration. This has been hypothesized to be due to estrogen deficiency-induced vertebral endplate degeneration and impaired nutrient diffusion to the discs. In fact, in a cohort study of over 1,500 women and 1,300 men, women had significantly higher MRI markers of intervertebral disc degeneration, and in postmenopausal women, the number of years since menopause was highly positively correlated with radiographic signs of lumbar disc degeneration.4
Osteoporosis: The Silent Threat to Your Spine
Osteoporosis is often called a “silent disease” because it typically doesn’t produce noticeable symptoms until it leads to fractures. By 2025, estimates suggest that osteoporosis will affect 500 million individuals worldwide, with postmenopausal women comprising the vast majority of cases.
Understanding Bone Mineral Density and Fracture Risk
Osteoporosis is defined by the World Health Organization as a bone mineral density (BMD) of -2.5 standard deviations or lower than the mean value for young adult women (T-score of ≤ -2.5 SD) on dual-energy X-ray absorptiometry (DEXA) scans of the lumbar spine, femoral neck, total proximal femur, or distal radius.5 The lower your T-score, the greater your fracture risk.
For postmenopausal women specifically:
- A T-score between -1.0 and -2.5 indicates osteopenia (low bone mass)
- A T-score of -2.5 or lower indicates osteoporosis
- Fragility fractures can occur even before reaching the osteoporosis threshold
Recent studies examining osteoporosis screening tools found that, among healthy postmenopausal women aged 50 to 64 years, the prevalence of osteoporosis at one or more anatomical sites (femoral neck, total hip, and/or lumbar spine) was 14.1%.6 This number increases dramatically with age, emphasizing the importance of early screening and intervention.
Vertebral Fractures: A Major Health Concern
Of all osteoporotic fractures, vertebral compression fractures are among the most common and impactful. They occur when the weakened vertebrae in your spine collapse under normal stress or minimal trauma. Unlike hip fractures that typically result from falls, vertebral fractures can happen during everyday activities like:
- Lifting a grocery bag
- Sneezing or coughing forcefully
- Bending forward to tie your shoes
- Simply standing up from a seated position
Vertebral fractures have significant consequences:
- Acute or chronic back pain: Often the first noticeable sign
- Height loss: Progressive vertebral fractures result in a gradual reduction in height, sometimes several inches over time
- Kyphosis (Dowager’s Hump): The rounded-back appearance from curvature of the upper spine
- Decreased mobility: Spinal deformities reduce range of motion and impact overall mobility
- Respiratory issues: Severe kyphosis can compress the lungs, reducing breathing capacity
- Psychological impact: Body image changes and chronic pain significantly affect quality of life
Research examining vertebral fractures in Moroccan postmenopausal women found that 62.3% had vertebral fractures detected on imaging, with 17.6% having moderate to severe fractures. The best predictors of these fractures were the number of years since menopause and lumbar spine bone mineral density.7 This underscores that both time and bone density contribute to spinal health problems in postmenopausal women.
Beyond Osteoporosis: Other Spine-Related Changes During Menopause
While osteoporosis rightfully receives significant attention, the effects of menopause on spine health extend to multiple other structures and systems.
Intervertebral Disc Degeneration and Low Back Pain
The intervertebral discs, the cushions between your vertebrae, are particularly vulnerable to hormonal changes. Estrogen receptors have been identified in disc tissue, indicating that these structures respond directly to hormonal signals. Studies in animals have demonstrated that estrogen deficiency leads to:
- Reduced disc height
- Increased oxidative stress in disc cells
- Accelerated autophagy (cellular breakdown)
- Transformation of nucleus pulposus cells from notochord cells to chondrocyte-like cells (a degenerative change)
- Reduced endplate porosity, limiting nutrient delivery to discs
- Downregulation of key structural proteins like aggrecan and type II collagen
A 2023 review on the relationship between estrogen and bone health noted that estrogen deficiency was linked not only to rapid bone loss in the lumbar spine but also to significant intervertebral disc degeneration.8 One study showed that menopausal women had substantially lower disc height than premenopausal women and menopausal women receiving estrogen replacement therapy.
This disc degeneration can contribute significantly to low back pain (LBP), which affects millions of women. Interestingly, the mechanisms remain poorly understood, but evidence suggests that exercise and parathyroid hormone show promise as therapeutic options for menopause-related LBP, while hormone replacement therapy and bisphosphonates appear less promising for this specific issue.
Facet Joint Osteoarthritis and Spinal Stenosis
The facet joints, small joints located between and behind adjacent vertebrae, also show accelerated degeneration after menopause. These joints guide and limit the spine’s movement. When they degenerate, they can cause:
- Localized back pain that worsens with extension (bending backward)
- Stiffness, especially in the morning
- Reduced range of motion
- Potential contribution to spinal stenosis as bone spurs develop
Coupled with ligamentum flavum hypertrophy (thickening of the ligaments in the spinal canal), these changes can lead to spinal stenosis, a narrowing of the spinal canal that compresses nerves and causes leg pain, numbness, weakness, and difficulty walking. Postmenopausal women face an increased risk for this condition compared to men of similar ages.
Recognizing the Symptoms: When Should You Be Concerned?
The spine-related symptoms of menopause and osteoporosis can be subtle at first but progressively worsen without intervention. Here’s what to watch for:
Early Warning Signs
- New or worsening lower back pain, especially pain that develops without a clear injury
- Morning stiffness in the back that improves with movement
- Pain that worsens with specific activities: prolonged sitting, bending forward, lifting
- Gradual loss of height (more than 1.5 inches suggests possible vertebral fractures)
- Changes in posture, including forward stooping
- Decreased flexibility in the spine
More Serious Symptoms Requiring Immediate Evaluation
- Sudden, severe back pain (possible acute vertebral fracture)
- Back pain accompanied by leg weakness, numbness, or difficulty walking
- Loss of bladder or bowel control (medical emergency)
- Multiple fractures from minimal trauma
- Significant kyphosis development

The Importance of Proper Diagnosis: Beyond Just Looking at Images
One of the most critical aspects of addressing spine health in menopausal women is ensuring accurate diagnosis. This requires more than just imaging studies; it demands a comprehensive evaluation that correlates your symptoms with physical examination findings and imaging results.
Too often, patients receive diagnoses based solely on MRI findings without proper clinical correlation. An MRI might show disc degeneration, a bulge, or osteoarthritic changes, but here’s the crucial point: these findings are extremely common in people without any pain. The presence of an abnormality on imaging doesn’t automatically mean it’s causing your symptoms.
A proper diagnostic approach requires three components working together:
- Detailed clinical history: When did symptoms start? What makes them better or worse? How have they progressed?
- Comprehensive physical examination: Neurological testing, range of motion assessment, palpation, provocative tests
- Appropriate imaging: MRI for soft tissue evaluation, DEXA scan for bone density, X-rays for alignment and structural assessment
Only when all three components align can your physician confidently identify the specific pain generators, the actual structures causing your symptoms. This is especially important for menopausal women who may have multiple overlapping conditions: osteoporosis with vertebral fractures, disc degeneration causing discogenic pain, facet joint arthritis, and spinal stenosis can all coexist. Each requires different treatment approaches.
The Value of a Second Opinion
Given the complexity of diagnosing spine-related issues in postmenopausal women, seeking a second opinion is often invaluable, especially if:
- You’ve been told you need surgery, but have questions about whether it’s truly necessary
- Conservative treatments haven’t provided adequate relief
- Your diagnosis seems unclear or doesn’t match your symptoms
- You want to explore all treatment options, including minimally invasive approaches
- Multiple physicians have given you conflicting recommendations
A thorough second opinion evaluation should include a review of all your imaging studies, a comprehensive physical examination, and a detailed discussion of your symptoms and their impact on your life. This process ensures you’re making truly informed decisions about your care rather than proceeding based on incomplete information.
Protecting Your Spine: Prevention and Treatment Strategies
The good news is that despite the significant challenges menopause poses to spine health, multiple evidence-based strategies can help protect your spine, maintain bone density, and manage symptoms effectively.
Exercise: The Most Powerful Tool
Exercise stands out as one of the most effective interventions for both preventing and managing spine changes associated with menopause. A 2025 scoping review found that exercise significantly improves bone mineral density and mental well-being in menopausal women.9 The key is choosing the right types of exercise:
- Weight-bearing exercises: Walking, jogging, dancing, stair climbing force bones to work against gravity, stimulating bone formation
- Resistance training: Using weights, resistance bands, or body weight builds both bone and muscle, providing dual benefits
- Balance exercises: Tai chi, yoga help prevent falls and subsequent fractures
- Core strengthening: Pilates and targeted abdominal and back exercises provide crucial spinal support
For maximum benefit, combine different types of exercise. Resistance training combined with impact exercises has been shown to produce better results than either alone. However, if you already have osteoporosis or vertebral fractures, work with a physical therapist to ensure exercises are safe and appropriate for your condition.

Nutrition: Building Blocks for Bone Health
Adequate nutrition plays a fundamental role in maintaining bone health during and after menopause:
- Calcium: 1,200 mg daily for women over 50 (from diet and supplements combined). Best sources include dairy products, leafy greens, and fortified foods
- Vitamin D: 800-1,000 IU daily to enhance calcium absorption. Many women are deficient and may need higher doses
- Protein: Adequate protein intake (1.0-1.2 g/kg body weight) supports both bone and muscle health
- Anti-inflammatory foods: Omega-3 fatty acids, colorful fruits and vegetables help reduce systemic inflammation
- Limit: Excessive caffeine, alcohol, and sodium, which can interfere with calcium absorption or increase calcium loss
Other Lifestyle Factors
- Smoking cessation: Smoking accelerates bone loss and impairs healing
- Weight management: Maintain a healthy body weight; being underweight increases fracture risk
- Fall prevention: Remove tripping hazards at home, ensure adequate lighting, and address vision problems
- Proper body mechanics: Learn safe lifting techniques and ergonomic principles
Medical Treatments for Osteoporosis
When lifestyle modifications alone aren’t sufficient to maintain bone health, several FDA-approved medications can help prevent bone loss and reduce fracture risk. Recent research published in February 2025 highlights evolving strategies for osteoporosis management in postmenopausal women:10
Antiresorptive Medications
These medications slow bone breakdown:
- Bisphosphonates (alendronate, risedronate, ibandronate, zoledronate): First-line treatment for most women, reducing vertebral fractures by up to 50%
- Denosumab: A twice-yearly injection that has shown sustained increases in BMD over up to 10 years with reduced fracture rates
- Selective Estrogen Receptor Modulators (SERMs): Raloxifene reduces vertebral fracture risk while avoiding some risks of hormone therapy
Anabolic Medications
These medications stimulate new bone formation:
- Teriparatide and abaloparatide: Daily injections that stimulate osteoblasts, reserved for women at very high fracture risk
- Romosozumab: The newest FDA-approved medication with both anabolic and antiresorptive effects, administered monthly for 12 months
Hormone Replacement Therapy (HRT)
Hormone replacement therapy remains controversial but can be effective for appropriate candidates. HRT has been shown to reduce hip and all fractures in large clinical trials, though current guidelines recommend it primarily for women with significant menopausal symptoms who also need fracture prevention, rather than for fracture prevention alone due to other health risks.
However, a comprehensive review noted that while hormone replacement therapy and bisphosphonates show efficacy for osteoporosis, evidence for their effectiveness in treating menopause-related low back pain from disc degeneration is less promising. Exercise and parathyroid hormone show more promise for addressing low back pain specifically.1
Emerging Therapies
Research is actively exploring innovative approaches to treating osteoporosis:
- Vibration therapy: The Osteoboost device delivers focused vibrations to the lumbar spine and hips, showing promising results in preserving bone density in postmenopausal women
- Gene therapy targeting GPR133: Recent 2025 research identified the GPR133 receptor as crucial to bone density, opening new treatment possibilities
- Repurposing osteoporosis drugs for disc degeneration: Studies are investigating whether treatments like bisphosphonates and sclerostin inhibitors could prevent or slow disc degeneration
What To Do If You're Experiencing Spine Problems Related to Menopause
If you’re dealing with back pain, suspected osteoporosis, or other spine-related symptoms during or after menopause, taking action early provides the best outcomes.
Steps to Take
- Get screened: If you’re postmenopausal and haven’t had a DEXA scan, schedule one. Early detection of low bone density allows for intervention before fractures occur
- Document your symptoms: Keep a journal of your pain, noting what makes it better or worse, its location and intensity, and how it affects your daily activities
- Seek comprehensive evaluation: Find a spine specialist who will take the time to correlate your symptoms with examination findings and imaging results
- Start conservative treatment appropriately: Physical therapy, exercise programs, and lifestyle modifications should typically be attempted before considering more invasive interventions
- Consider a second opinion: If recommendations don’t feel right or you want to explore all options, seek additional expert input
When Conservative Treatment Isn't Enough
Most spine problems related to menopause improve with comprehensive conservative care. However, certain situations warrant consideration of more advanced interventions:
- Vertebral compression fractures causing severe pain that doesn’t improve with conservative treatment
- Progressive neurological symptoms (weakness, numbness) from nerve compression
- Severe disc herniation with radicular symptoms (sciatica) that limits function despite appropriate treatment
- Spinal stenosis causing significant walking difficulty and leg symptoms
- Quality of life severely impacted despite comprehensive conservative care
In these situations, minimally invasive surgical options may provide relief. For instance, vertebral compression fractures can often be treated with vertebroplasty or kyphoplasty; procedures that stabilize the fracture and reduce pain. For disc herniations or stenosis, advanced endoscopic techniques offer the possibility of addressing the problem while preserving your spine’s natural structure and avoiding fusion surgery.
At Deuk Spine Institute, we specialize in minimally invasive approaches that address spine problems while maintaining your natural spinal motion and stability. Rather than recommending fusion surgery that permanently alters spine mechanics, we focus on identifying and treating specific pain generators through targeted, tissue-preserving techniques.
Real Patient Experience: Finding Relief Without Fusion
While we don’t have specific testimonials from patients discussing menopause-related spine issues, many of our female patients in the age range affected by menopause have found relief from chronic back pain through our minimally invasive approaches. For instance, a California native recently shared her experience after 30 years of debilitating pain. She had exhausted conservative treatments, surgical options and was living with constant pain that affected every aspect of her life.
After receiving treatment with our advanced minimally invasive techniques, she reports being “totally pain-free.” She was back on her feet within an hour of the procedure and experienced rapid recovery without the extended downtime associated with traditional spine surgery.
Stories like this illustrate an important point: when conservative treatments fail to provide adequate relief, advanced minimally invasive options can offer life-changing results without the risks, prolonged recovery, and permanent alterations to spine mechanics associated with traditional fusion surgery.
Key Takeaways: What You Need to Remember
- Menopause fundamentally affects spine health: Declining estrogen doesn’t just cause bone loss, it also accelerates disc degeneration, facet joint arthritis, and increases inflammation and pain perception
- Osteoporosis is common and serious: Women can lose up to 20% of bone mass in the first five to seven years after menopause, dramatically increasing fracture risk. Early screening with DEXA scans is essential
- Vertebral fractures have lasting consequences: Beyond acute pain, they can cause height loss, kyphosis, reduced mobility, and respiratory compromise. They often occur during routine activities
- Accurate diagnosis requires correlation: Imaging findings must match your symptoms and physical examination. Not all abnormalities seen on MRI cause pain, and proper diagnosis identifies specific pain generators
- Exercise is your most powerful tool: Weight-bearing exercise, resistance training, and balance activities improve bone density, muscle strength, and overall spine health. The evidence strongly supports this approach
- Multiple treatment options exist: From lifestyle modifications to medications to minimally invasive procedures, modern medicine offers many ways to protect bone health and address spine problems
- Second opinions matter: Given the complexity of menopause-related spine issues and the significant variation in treatment recommendations, seeking expert second opinions helps ensure you understand all your options
- Prevention is possible: Taking proactive steps in perimenopause and early postmenopause, getting screened, starting appropriate exercise, and ensuring adequate nutrition can significantly reduce your risk of serious problems later
Frequently Asked Questions
-
At what age should I get a DEXA scan to check my bone density?
The National Osteoporosis Foundation recommends that all women 65 and older receive DEXA screening. However, you should be screened earlier (starting at menopause) if you have risk factors, including: early menopause (before age 45), family history of osteoporosis, low body weight (under 127 pounds), history of fractures as an adult, prolonged corticosteroid use, certain medical conditions (rheumatoid arthritis, hyperthyroidism), smoking, or excessive alcohol consumption. Don’t wait for symptoms; osteoporosis is silent until a fracture occurs.
-
Can I reverse osteoporosis once I have it?
While you cannot completely reverse osteoporosis to pre-disease levels, you can significantly improve bone density and reduce fracture risk with appropriate treatment. The most effective approach combines medication (when indicated), weight-bearing exercise, resistance training, adequate calcium and vitamin D intake, and lifestyle modifications. Studies show that anabolic medications like romosozumab can produce substantial increases in bone density. Recent research even suggests that future treatments targeting the GPR133 receptor may strengthen existing bone and rebuild degraded bone. The key is early intervention; the earlier treatment begins, the better the outcomes.
-
Is hormone replacement therapy safe for preventing osteoporosis?
Hormone replacement therapy (HRT) is effective at preventing bone loss and reducing fracture risk in postmenopausal women. Large studies, such as the Women’s Health Initiative, demonstrated significant reductions in hip and vertebral fractures with HRT. However, HRT also carries potential risks, including increased risk of blood clots, stroke, and certain cancers, depending on the formulation and duration of use. Current guidelines recommend considering HRT primarily for women who have significant menopausal symptoms (hot flashes, night sweats) AND need fracture prevention, rather than for bone health alone. The decision requires individualized assessment of your personal risk factors, symptoms, and preferences in consultation with your healthcare provider.
-
Will I definitely get osteoporosis after menopause?
No, not all women develop osteoporosis after menopause. While the risk increases significantly, affecting roughly 30% of postmenopausal women in the United States, many women maintain healthy bone density throughout their lives. Factors that influence your risk include genetics (family history), peak bone mass achieved in youth, race and ethnicity (Caucasian and Asian women face higher risk), body weight (higher weight provides some protection), physical activity levels throughout life, nutrition (calcium and vitamin D intake), smoking and alcohol use, and certain medications. By addressing modifiable risk factors, you can significantly reduce your likelihood of developing osteoporosis even after estrogen levels decline.
-
How do I know if my back pain is from osteoporosis, disc problems, or something else?
This is precisely why proper diagnosis is so important. Osteoporotic vertebral fractures typically cause sudden, severe back pain that may occur after minimal trauma or even spontaneously. The pain is usually localized to the fractured vertebra and may worsen with movement. Disc-related pain often develops more gradually, may radiate into the legs (sciatica), and has specific patterns that worsen with certain positions (sitting for disc problems, standing/walking for stenosis).11 Facet joint arthritis typically causes pain that worsens with extension (bending backward). However, these conditions frequently coexist in postmenopausal women, and symptoms can overlap. A comprehensive evaluation by a spine specialist, correlating your clinical symptoms with physical examination findings and appropriate imaging (MRI, X-rays, DEXA scan), is essential for accurate diagnosis. Don’t accept treatment recommendations based on imaging alone without thorough clinical correlation.
-
Can physical therapy actually help osteoporosis, or is medication the only real treatment?
Physical therapy and exercise are not just helpful; they’re essential components of osteoporosis management and may be more effective than medication alone. Research consistently shows that weight-bearing exercise and resistance training improve bone density, reduce fall risk, improve balance and coordination, and enhance quality of life. A 2025 review found that exercise significantly improves bone mineral density in menopausal women. For many women with osteopenia or mild osteoporosis, exercise-based interventions may be sufficient without medication. For those with more significant bone loss, combining exercise with appropriate medications produces better results than either approach alone. The key is working with a physical therapist experienced in osteoporosis who can design a safe, progressive program appropriate for your bone density and current fitness level.
Taking Control of Your Spine Health During and After Menopause
The connection between menopause, osteoporosis, and spine health is profound and affects millions of women worldwide. The hormonal changes that occur during this natural transition have far-reaching effects on your bones, discs, joints, muscles, and even how your body experiences pain. The risks are real: accelerated bone loss, vertebral fractures, disc degeneration, and chronic back pain can significantly impact quality of life.
But here’s the encouraging news: you have more control over your spine health than you might think. Early screening, evidence-based prevention strategies, comprehensive exercise programs, proper nutrition, and appropriate medical treatments when needed can dramatically reduce your risk of serious problems. The research shows that taking action during perimenopause and early postmenopause, when bone loss is most rapid, provides the greatest benefits.
If you’re already experiencing symptoms, whether back pain, neck pain, height loss, or concerns about your bone density, don’t wait.12 Seek evaluation from a spine specialist who will take the time to properly diagnose your condition by correlating your symptoms with examination findings and imaging results, not just looking at pictures. Insist on identifying specific pain generators rather than receiving generic diagnoses based on common imaging findings.
And if you’ve been told you need surgery, or if conservative treatments haven’t provided adequate relief, consider getting a second opinion. Advances in minimally invasive spine surgery mean that many conditions once requiring fusion or other major procedures can now be addressed through targeted, tissue-preserving techniques that maintain your spine’s natural structure and function.
At Deuk Spine Institute, we’re committed to providing comprehensive evaluations and the full spectrum of treatment options, from conservative care guidance to the most advanced minimally invasive procedures available. We believe in accurate diagnosis, identifying specific pain generators, and choosing treatments that address your particular problem while preserving your spine’s natural capabilities.
Upload your latest MRI for a free virtual consultation and review with Dr. Ara Deukmedjian. Take the first step toward understanding your diagnosis, exploring all your options, and making informed decisions about your spine health. Schedule your free consultation today.

Sources
1: https://www.mdpi.com/2073-4409/15/2/148
2: https://www.mdpi.com/1422-0067/25/22/12139
3: https://www.nejm.org/doi/full/10.1056/NEJM199809103391104
5: https://pmc.ncbi.nlm.nih.gov/articles/PMC6059859/
6: https://pmc.ncbi.nlm.nih.gov/articles/PMC11920839/
7: https://pmc.ncbi.nlm.nih.gov/articles/PMC4435629/
8: https://www.nature.com/articles/s41413-023-00280-x
9: https://www.frontiersin.org/journals/reproductive-health/articles/10.3389/frph.2025.1542746/full
11: https://deukspine.com/blog/understanding-l4-l5-disc-herniation/


