


Diagnosis. Answers. Relief.
Submit your MRI for a free expert review by Dr. Ara Deukmedjian, M.D. — board-certified neurosurgeon. No obligation. Real answers.
Schedule Yours Today 2,000+ procedures · Zero major complications · No cost, no obligationWhat “L4-L5 Disc Herniation” Actually Means
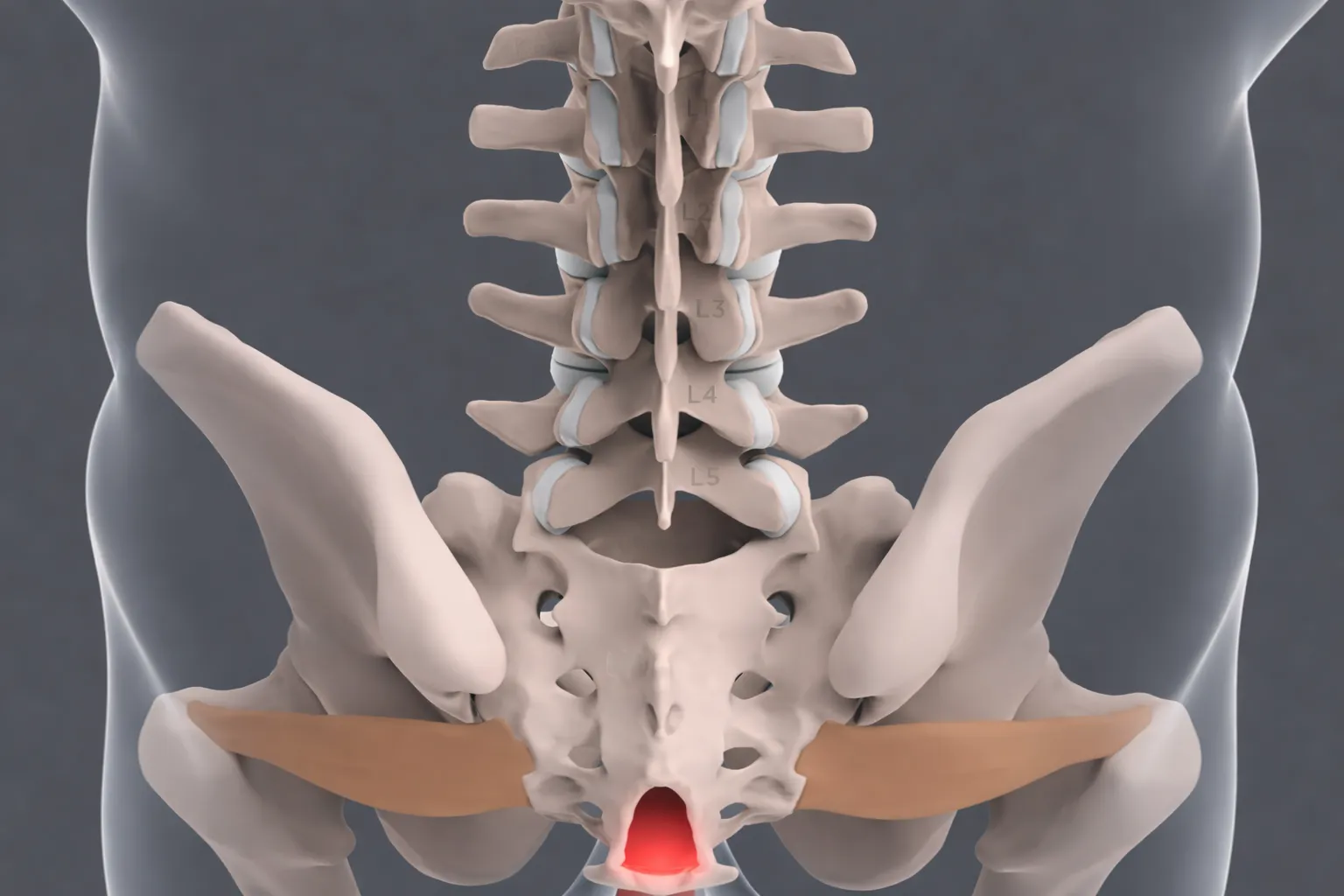
The lumbar spine consists of five vertebrae, L1 through L5, stacked between the thoracic spine above and the sacrum below. The L4-L5 segment sits at the bottom of that stack, at the point where the mobile lumbar spine transitions into the relatively fixed pelvis. Every time you bend, lift, twist, or sit, that segment absorbs a disproportionate share of the mechanical load.
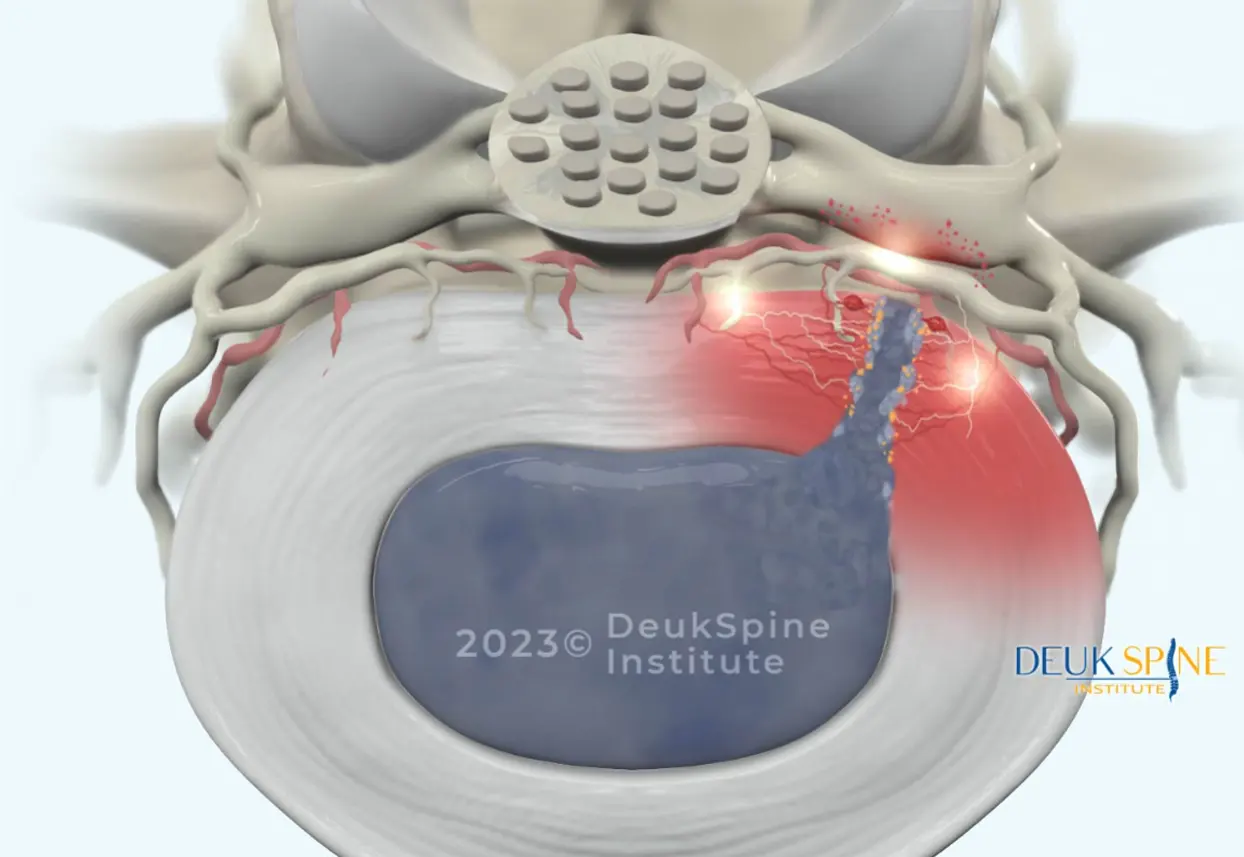
The intervertebral disc between L4 and L5 is a two-layer structure: a firm outer ring of collagen called the annulus fibrosus, and a soft, gel-like inner core called the nucleus pulposus. A herniation occurs when the annulus develops tears or weakens enough to let the nucleus push through. When that displaced material contacts and compresses a nearby nerve root, it causes the inflammation and neurological symptoms that bring most patients to a spine specialist.
The specific nerve most commonly affected at this level is the L5 nerve root, which provides sensation to the outer leg and top of the foot and controls muscles responsible for lifting the foot and extending the big toe. This anatomy explains the predictable symptom pattern that physicians use to identify L4-L5 as the pain source. Without needing to guess.
The Four Types of Disc Displacement at L4-L5
Not all disc herniations are the same, and the type affects both natural history and treatment planning:
Disc bulge: The disc extends symmetrically beyond the vertebral margin. The annulus is intact. This represents early degenerative change and may be asymptomatic.
Disc protrusion: The nucleus pushes against an intact but weakened annulus, creating a focal outpouching. The base of the protrusion is wider than the displaced portion.
Disc extrusion: The nucleus breaks fully through the annulus but remains connected to the parent disc. This typically causes more significant nerve compression and paradoxically, extruded fragments are more likely to reabsorb naturally because the immune system identifies them as foreign tissue. ⁴
Disc sequestration: A free fragment of disc material separates completely and migrates within the spinal canal. This is the most severe displacement but, counterintuitively, may show greater spontaneous reabsorption over time.
Each vertebra in your lumbar spine has specific characteristics and potential issues:4

What Causes L4-L5 Disc Herniation
Understanding causation helps explain why the same segment is so frequently affected and why some patients are more vulnerable than others.
Age-related degeneration is the dominant driver. Discs lose water content progressively beginning in the third or fourth decade of life, making the annulus stiffer and more prone to tearing. This is not pathology in the clinical sense. It is universal but it creates the substrate for herniation under load.
This degenerative process on its own doesn’t always cause pain, and telling the difference between a degenerated disc and one that’s actually generating your symptoms is a separate diagnostic step worth understanding before any treatment decision.
Acute trauma can herniate an otherwise healthy disc. Motor vehicle accidents, falls, and improper lifting with heavy loads can generate forces that exceed the disc’s structural tolerance in a single event. ⁹

Cumulative occupational stress: heavy lifting, prolonged sitting, vibration exposure can cause cumulative annular damage over months and years. Each individual stress is minor; the aggregate effect is not.
Genetic predisposition is increasingly recognized as a contributor. Studies show that disc degeneration has a hereditary component, with some individuals showing accelerated disc aging at relatively young ages regardless of activity level.
Modifiable Risk Factors That Affect Prognosis
Several factors within a patient’s control affect both the risk of initial herniation and the likelihood of symptom improvement:
Smoking reduces disc nutrition by impairing vascular supply, increases systemic inflammation, and creates repetitive spinal stress through chronic coughing. Smokers consistently show worse disc degeneration and poorer treatment outcomes across studies.
Obesity increases compressive loads on lumbar discs and is associated with chronic systemic inflammation that may impair disc metabolism.
Prolonged sitting increases intradiscal pressure by approximately 40% compared with standing. A figure from biomechanical research that explains the near-universal experience of sitting-intolerant sciatica. ¹⁰ This single data point should inform every acute management plan.
Sedentary lifestyle and weak core musculature remove the active stabilization that reduces disc loading during daily movement.
Recognizing L4-L5 Disc Herniation: Symptoms
The distribution of symptoms at L4-L5 is specific enough that an experienced clinician can often identify the correct level before any imaging is ordered. Understanding this distribution helps patients recognize whether their symptoms fit the pattern.
The Hallmark: L5 Radiculopathy

When the herniated disc at L4-L5 compresses the L5 nerve root, it produces a characteristic pain that travels from the lower back or buttock down the outer side of the leg, continuing to the top of the foot and the space between the first and second toes. This is not generalized leg pain. It follows a specific anatomical path.
The pain is typically described as sharp, shooting, or electric feeling dull, aching back pain. It can be severe enough to stop movement mid-stride or make sitting in a car or chair nearly impossible.
Neurological Findings That Confirm Back Pain At L5
Beyond pain, L5 nerve root compression produces predictable neurological deficits that a physician can test at the bedside.
Weakness in ankle dorsiflexion: Difficulty lifting the front of the foot, which can progress to foot drop. The inability to clear the foot during walking. This is one of the more serious functional consequences of L4-L5 compression.
Weakness in Big toe extension: Inability to push the big toe up against resistance.
Numbness and tingling in the L5 dermatome distribution: outer leg, top of foot, and the first two toes.
Trendelenburg gait: Hip dropping on the affected side during single-leg stance, indicating gluteus medius weakness. Recent clinical guides specifically identify this as a 2025-confirmed finding in L5 radiculopathy. ²
These specific findings are clinically valuable because they help distinguish L4-L5 compression from L5-S1 compression (which typically affects the heel and outer foot via the S1 nerve root) and from peripheral nerve disorders.
Symptoms That Require Emergency Evaluation
One symptom cluster demands immediate emergency care, not a scheduled appointment:
Bowel or bladder dysfunction. Difficulty urinating, urinary retention, or loss of bowel control; combined with saddle anesthesia (numbness in the groin and inner thighs) and bilateral leg weakness indicates cauda equina syndrome. This occurs when a massive herniation compresses multiple nerve roots simultaneously. Without urgent surgical decompression, permanent loss of bowel, bladder, and lower extremity function can result. ⁵
If you develop any combination of these symptoms, go to an emergency room immediately. This is the one situation in which waiting for conservative treatment is not appropriate.
Diagnosis. Answers. Relief.
Submit your MRI for a free expert review by Dr. Ara Deukmedjian, M.D. — board-certified neurosurgeon. No obligation. Real answers.
Schedule Yours Today 2,000+ procedures · Zero major complications · No cost, no obligation
No cost · No obligation
Live Pain Free
Upload your MRI for a free expert review by Dr. Ara Deukmedjian, M.D. — board-certified neurosurgeon. Ten minutes can change your life.
No cost · No obligation
Live Pain Free
Upload your MRI for a free expert review by Dr. Ara Deukmedjian, M.D. — board-certified neurosurgeon. Ten minutes can change your life.
What These Numbers Don’t Tell You
- The Most Important Variable Is Whether the Right Operation Was Chosen
A 95% successful procedure applied to the wrong diagnosis has a 0% chance of helping the patient. The most common reason spine surgery fails is not technical execution. It is a mismatch between the procedure performed and the actual pain source. A patient with discogenic pain from a contained herniation is not made better by fusion regardless of how cleanly the screws are placed. A patient with true mechanical instability from spondylolisthesis is not made better by an endoscopic discectomy regardless of how elegant the technique.
The diagnostic process; clinical correlation of symptoms, examination, and imaging. Is not administrative. It is the most consequential step in the entire treatment pathway.
- “Minimally Invasive” Describes the Access, Not the Operation
This distinction matters when evaluating any surgical recommendation. A minimally invasive fusion is still a fusion. The smaller incision spares some muscle and shortens early recovery. It does not change what happens to the vertebrae, the disc, the hardware, or the adjacent segments over the following decade. Patients consenting to any spine surgery should understand what is being done to their spine beneath the skin. Not just how large the incision is.
- Delaying Necessary Surgery Has Real Costs
The appropriate framing is not “avoid surgery as long as possible.” It is “give conservative treatment a genuine, time-limited trial, then make a deliberate decision.” Prolonged compression of the L5 nerve root can cause:
- Irreversible nerve damage: Muscle atrophy from denervation may not fully recover even after successful surgical decompression. The window for optimal neurological recovery is not unlimited.
- Central sensitization: Extended severe pain alters the nervous system’s pain processing, making pain harder to treat even after the structural source is addressed.
- Disability cascade: Job loss, deconditioning, depression, and opioid dependence are documented consequences of undertreated chronic radiculopathy.

Living with L4-L5 Disc Herniation: Evidence-Based Self-Management
While pursuing evaluation or treatment, practical management strategies can reduce symptom burden and prevent worsening.
Sleep position: Back sleeping with a pillow under the knees is optimal. It maintains the lumbar curve and minimizes disc pressure. Side sleeping with a pillow between the knees is acceptable. Stomach sleeping increases lumbar extension and disc loading and should be avoided entirely.
Sitting: Given the 40% intradiscal pressure increase that sitting produces compared with standing, ¹⁰ taking a 2–3 minute standing break every 30 minutes is not a comfort preference. It is evidence-based management. Lumbar support that maintains the natural lordosis is important when sitting cannot be avoided.
Lifting: Bend at the knees, not the waist. Keep objects close to the body. Avoid twisting during the lift. Ask for help with heavy objects.
Exercise: Walking, water exercise, and stationary cycling are appropriate for most patients in the subacute phase. High-impact activities, heavy deadlifts and squats, and sports involving twisting should be avoided until symptoms are controlled.
Smoking cessation: One of the few modifiable variables with documented impact on disc healing and surgical outcomes.
Diagnosis. Answers. Relief.
Submit your MRI for a free expert review by Dr. Ara Deukmedjian, M.D. — board-certified neurosurgeon. No obligation. Real answers.
Schedule Yours Today 2,000+ procedures · Zero major complications · No cost, no obligation
No cost · No obligation
Live Pain Free
Upload your MRI for a free expert review by Dr. Ara Deukmedjian, M.D. — board-certified neurosurgeon. Ten minutes can change your life.


