

By Dr. Ara Deukmedjian, MD
Board-Certified Neurosurgeon, Deuk Spine Institute
Medically reviewed on January 23, 2026
Medical disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
Key Takeaways
Before diving into the details, here’s what you need to know about C7-T1 bulging discs:
- C7-T1 disc herniations account for only 3.5-8% of all cervical disc problems, making them less common but uniquely challenging due to the transition zone between the mobile neck and the rigid upper back.1
- Trauma is significantly associated with C7-T1 disc herniations compared to other cervical levels, with research showing a strong correlation between injury history and this specific location.2
- The C8 nerve root compression causes distinctive symptoms: Primary, motor weakness in hands, followed by pain radiating to the ring and little fingers, and grip strength problems that affect fine motor tasks.3
- 91.7% of C7-T1 herniations occur in the foraminal region (side of the spine) rather than centrally, requiring specialized surgical approaches when conservative treatment fails.2
- Conservative treatment should be comprehensive and time-limited: Most patients benefit from 6-12 weeks of appropriate care, but persistent symptoms warrant advanced intervention.
- Ultra-minimally invasive endoscopic surgery like Deuk Laser Disc Repair® offers a motion-preserving alternative to traditional fusion, with published pain elimination success rates exceeding 99% and no major complications.
Understanding the C7-T1 Junction: Why This Area Is Uniquely Vulnerable
The C7-T1 spinal segment sits at a critical transition point in your spine: the cervicothoracic junction. This is where the highly flexible neck meets the rigid upper back, creating a stress concentration point, as biomechanical researchers describe it.
Think of it like the hinge on a door that opens and closes thousands of times. The C7-T1 junction experiences similar repetitive stress, but with an added complication: it’s nearly twice as stiff as the cervical spine above it while still maintaining some mobility.4 This unique biomechanical environment makes the disc at this level susceptible to both acute injury and chronic degeneration.
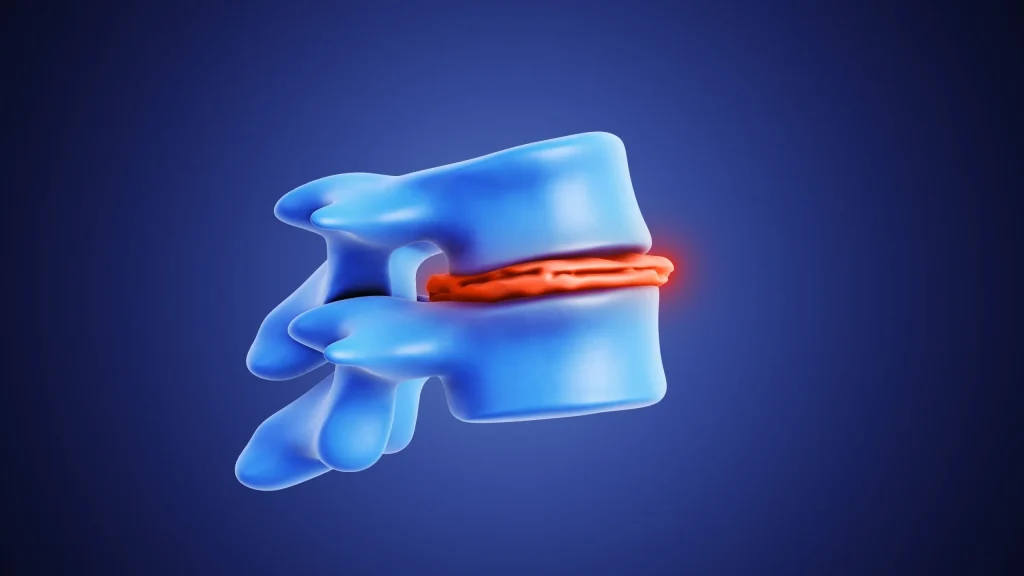
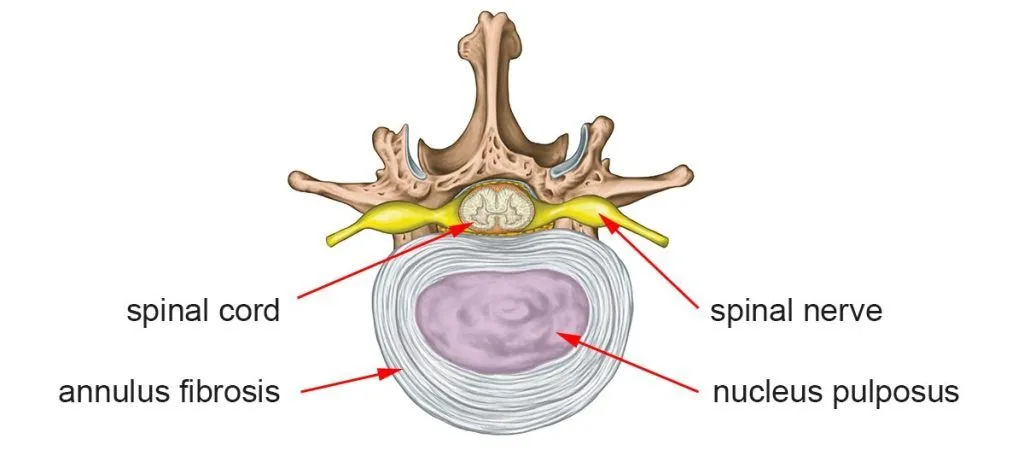
The C7 vertebra, also known as vertebra prominens, is the last cervical vertebra and features the longest spinous process, the bony bump you can feel at the base of your neck. Below it sits T1, the first thoracic vertebra, which connects to your first rib. Between these two vertebrae lies the C7-T1 intervertebral disc, a shock-absorbing cushion composed of a tough outer ring (annulus fibrosus) surrounding a gel-like inner core (nucleus pulposus).
The C8 Nerve Root: Your Hand’s Communication Highway
What makes C7-T1 disc problems particularly troublesome is the C8 nerve root that exits between these vertebrae. Unlike other nerve roots in your body, the C8 nerve is composed predominantly of motor fibers responsible for controlling the intrinsic muscles of your hand, the small muscles between your fingers that allow you to grip, pinch, and perform delicate tasks.3
When a bulging disc compresses this nerve, the results are immediately noticeable in your daily life: difficulty buttoning shirts, trouble typing, weakness when opening jars, and that frustrating sensation of dropping objects unexpectedly.
How C7-T1 Disc Bulges Actually Happen: Real-World Scenarios
While medical textbooks describe disc bulges in clinical terms, understanding how they actually occur helps patients recognize risk factors and make informed decisions about prevention and treatment.
The Weekend Warrior
A 52-year-old accountant spent most weekdays at his desk, his neck craned forward, reviewing spreadsheets on dual monitors. On weekends, he’d throw himself into home improvement projects to “stay active.” One Saturday, while moving heavy lumber for a deck project, he twisted awkwardly while carrying a load, combining forward neck flexion, rotation, and compression.
He felt a sharp pain at the base of his neck immediately, but pushed through. Over the next few days, the pain intensified and began radiating down his right arm into his ring and little fingers. Within a week, he noticed weakness when trying to grip his coffee cup.
What happened? Years of poor posture had gradually dehydrated and weakened John’s C7-T1 disc. The annulus fibrosus had developed microscopic tears due to chronic forward head posture, which we now call “tech neck.”5 The acute twisting motion while lifting was the final insult that caused the disc’s inner material to bulge through those weakened fibers, compressing his C8 nerve root.
The Whiplash Connection
Research shows that trauma is significantly associated with C7-T1 disc herniations compared to other cervical levels.2 Motor vehicle accidents are a common culprit.
Let’s assume a woman was rear-ended at a stoplight. Her head snapped backward, then forward, in classic whiplash fashion. Initially, she experienced typical neck soreness, but as we discuss in our article on delayed pain after accidents, symptoms often worsen days later when inflammation peaks.6
Two weeks post-accident, she developed severe pain radiating down the ulnar (pinky) side of her left arm, accompanied by numbness in her ring and little fingers. An MRI revealed a C7-T1 disc bulge with foraminal stenosis; the disc material had been forced laterally during the trauma, narrowing the space where her C8 nerve exits the spine.
The Construction Worker’s Burden
A man worked in construction for 30 years, regularly lifting heavy materials, operating vibrating equipment, and spending long hours in awkward positions. At 48, he began experiencing intermittent neck stiffness at the base of his skull.
Workers in physically demanding jobs face elevated risk for C7-T1 disc problems due to repetitive mechanical stress. The combination of heavy lifting, vibration exposure, and sustained awkward postures accelerates disc degeneration at this already vulnerable transition zone.7
He initially ignored the symptoms, attributing them to “getting older.” By the time he sought treatment, he had developed significant weakness in his right hand, struggling to grip tools he’d used effortlessly for decades.
Recognizing C7-T1 Bulging Disc Symptoms: What You’ll Actually Feel
C7-T1 disc problems produce a characteristic symptom pattern that distinguishes them from other cervical disc issues. Understanding these symptoms helps you and your physician accurately diagnose the problem.
Neck Pain at the Base
The first symptom most patients notice is localized pain at the base of the neck. Unlike higher cervical disc problems that produce pain in the mid-neck region, C7-T1 issues cause discomfort right where your neck meets your shoulders; the area you might rub when you say your “shoulders are tight.”
This pain typically:
- Worsens with neck extension (looking up) or rotation
- Intensifies after prolonged sitting or computer work
- Creates a deep, aching sensation that can feel like muscle tension
- May be accompanied by audible clicking or grinding with neck movement
The Ulnar Nerve Distribution: Ring and Pinky Finger Symptoms
The hallmark feature of C8 nerve root compression is symptoms in the ulnar distribution; the ring and little fingers, along with the ulnar (pinky) side of the hand and forearm. Research confirms that 91.7% of C7-T1 herniations occur in the foraminal region, directly compressing the exiting C8 nerve.2
Patients describe:
- Sharp, burning, or electric-shock pain traveling from the base of the neck, through the inner upper arm, down the ulnar forearm, and into the ring and little fingers
- Numbness or “pins and needles” sensation in these same areas, often worse at night or upon waking
- Temperature sensitivity changes, with some patients reporting that their affected fingers feel colder than the others

Intrinsic Hand Muscle Weakness: The Grip Strength Problem
Because the C8 nerve root is predominantly composed of motor fibers controlling intrinsic hand muscles, weakness is a prominent and concerning feature of C7-T1 disc problems.3
Clinical studies show that the main presentation is unilateral motor weakness in intrinsic hand muscles, affecting tasks requiring fine motor control.
You might notice:
- Difficulty with precision grip: Trouble picking up small objects like coins, buttons, or pills
- Reduced grip strength: Problems opening jars, holding a coffee cup firmly, or maintaining a grip on objects
- Weakness in finger abduction/adduction: Inability to spread your fingers apart or bring them together with normal strength
- Thumb weakness: Difficulty with thumb extension and opposition (touching your thumb to your other fingers)
- Atrophy in severe cases: Visible muscle wasting in the spaces between the bones on the back of your hand
It’s Not Carpal Tunnel Syndrome
One of the most common misdiagnoses for C7-T1 disc problems is carpal tunnel syndrome. As we discuss in our comprehensive article on this topic, while both conditions can cause hand numbness and weakness, there are key differences:8
- Carpal tunnel syndrome affects the thumb, index, middle, and thumb-side of the ring finger (distribution of the median nerve). Symptoms are typically worse at night and relieved by shaking the hand. A positive Phalen’s test or Tinel’s sign at the wrist confirms the diagnosis.
- C7-T1 disc problems affect the ring and little fingers (C8/ulnar distribution). Symptoms worsen with neck positions and often improve with shoulder abduction (putting your hand on top of your head). A positive Spurling test confirms cervical nerve root compression.
Getting the correct diagnosis is crucial because treating carpal tunnel syndrome when you actually have a cervical disc problem leads to failed surgery and persistent symptoms.
The Diagnostic Process: Confirming Your C7-T1 Disc Bulge
Accurate diagnosis requires correlating your symptoms with physical examination findings and imaging studies.
Physical Examination
Your physician will perform several specific tests:
The Spurling Test: Your doctor extends your neck and rotates it toward the affected side while applying downward pressure on your head. This narrows the intervertebral foramen and reproduces radicular symptoms if nerve compression exists.9
Neurological Assessment: Testing includes evaluation of sensation in the C8 dermatome (ring and little fingers), motor strength testing of intrinsic hand muscles, and assessment of reflexes. The triceps reflex may be diminished if C7 is also involved.
Grip Strength Testing: Comparing grip strength between hands using a dynamometer provides objective evidence of motor weakness.
Imaging Studies
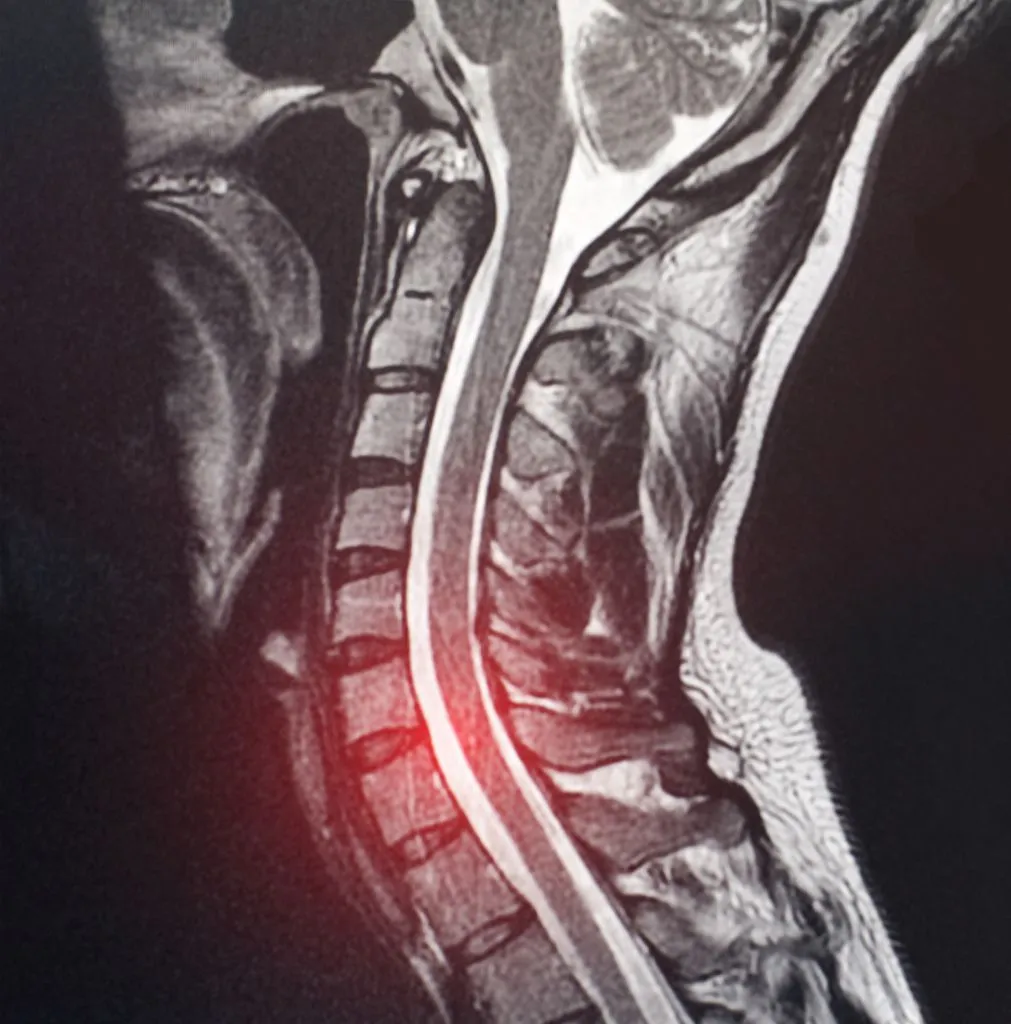
MRI: The gold standard for visualizing C7-T1 disc pathology. However, this level can be challenging to image due to shoulder overlap and the transition to the thoracic spine. Dedicated cervicothoracic junction sequences may be necessary for optimal visualization.
X-rays: While they cannot visualize the disc itself, flexion-extension x-rays can reveal instability at the C7-T1 level, which influences treatment decisions.
CT Myelography: Sometimes used when MRI is contraindicated or when bone detail is needed for surgical planning, particularly to assess foraminal narrowing from osteophytes.
EMG/Nerve Conduction Studies: Electrodiagnostic testing confirms C8 nerve root involvement, distinguishes it from ulnar neuropathy or thoracic outlet syndrome, and assesses the chronicity and severity of nerve damage.
Conservative Treatment: A Comprehensive, Time-Limited Approach
When a C7-T1 disc bulge is diagnosed, conservative treatment is typically the first approach, but it must be comprehensive, properly executed, and time-limited. Too often, patients receive half-hearted conservative care that prolongs suffering without addressing the underlying problem.

Phase 1: Acute Pain Management and Activity Modification (Weeks 1-2)
The initial focus is on controlling pain and inflammation while protecting the injured disc from further damage.
Medications: NSAIDs like ibuprofen or naproxen reduce inflammation and pain. Muscle relaxants such as cyclobenzaprine can help if muscle spasm is prominent. For severe pain, a short course of oral corticosteroids may rapidly reduce nerve inflammation.
Activity Modification: Avoid neck extension, heavy lifting, and repetitive reaching overhead. However, complete rest is counterproductive—gentle movement maintains circulation and prevents muscle deconditioning. Short walks are encouraged.
Ergonomic Adjustments: Raise computer monitors to eye level, use a headset for phone calls, and ensure your workspace supports neutral neck positioning. As discussed in our article on office chairs for herniated discs, proper lumbar support indirectly helps cervical posture.10
Sleeping Position Optimization: Side sleeping with a cervical pillow that maintains natural neck curvature is ideal. Our comprehensive guide to sleeping positions for neck pain provides specific recommendations.11
Phase 2: Physical Therapy and Targeted Exercise (Weeks 3-8)
Once acute pain subsides, structured physical therapy becomes the cornerstone of conservative care.
Manual Therapy: Gentle mobilization techniques can improve joint mechanics at the cervicothoracic junction without aggressive manipulation that might worsen disc pathology.
Nerve Gliding Exercises: Specific movements help the C8 nerve move more freely through the foramen, potentially reducing irritation and improving symptoms.
Cervical Strengthening: Deep neck flexor strengthening addresses the muscle imbalances that contribute to forward head posture. Scapular stabilization exercises improve upper back support for the cervical spine.
Postural Training: Learning proper biomechanics for daily activities—how to lift, reach, and position yourself—prevents recurrence.
Home Exercise Program: Success depends on patient compliance with daily exercises. Most effective programs require 15-20 minutes of targeted exercises twice daily.
Phase 3: Injection Therapy for Persistent Symptoms (Weeks 8-12)
If symptoms persist despite appropriate conservative care, selective nerve root blocks or epidural steroid injections may be considered.
Cervical Epidural Steroid Injection: Delivers anti-inflammatory medication directly to the epidural space around the C8 nerve root, potentially providing weeks to months of relief.
Selective Nerve Root Block: A more targeted approach that both diagnoses and treats C8 nerve root compression. If symptoms significantly improve after a diagnostic block, it confirms that C7-T1 is the pain generator.
Limitations of Injections: These provide temporary relief and don’t address the structural disc problem. They’re most useful for severe pain that prevents participation in physical therapy or for diagnostic purposes.
When Conservative Treatment Isn’t Working
Research shows that approximately 75-90% of patients with disc problems improve with comprehensive conservative care. However, improvement should be evident within 6-12 weeks. You should consider a more advanced intervention if:
- Pain is progressively worsening despite appropriate treatment
- You develop a new or worsening weakness in your hand
- Symptoms significantly impact your ability to work or perform daily activities
- You’ve completed 12 weeks of comprehensive conservative care without adequate improvement
- You experience bowel or bladder dysfunction (immediate surgical emergency)
Surgical Options: Traditional Approaches vs. Ultra-Minimally Invasive Endoscopic Surgery
When conservative treatment fails to provide adequate relief, surgery may be necessary. However, not all surgical approaches are created equal, and the C7-T1 level presents unique challenges that require specialized expertise.
The C7-T1 Surgical Challenge
The cervicothoracic junction is one of the most technically demanding areas of the spine to access surgically. The T1 vertebra sits behind the sternum, major blood vessels course through this region, and the thoracic duct, pleura, and apex of the lung are all in close proximity.1
Traditional anterior approaches may require a sternotomy or partial removal of the manubrium in patients with unfavorable anatomy. Posterior approaches must navigate the transition from the mobile cervical spine to the fixed thoracic spine.
Traditional Surgical Approaches
Anterior Cervical Discectomy and Fusion (ACDF): This has been the standard surgical treatment for C7-T1 disc problems. The surgeon approaches from the front of the neck, removes the damaged disc, decompresses the C8 nerve root, and fuses C7 to T1 using a cage and plate.
Studies show ACDF can be effective, with research indicating reasonable outcomes at this level.3 However, fusion comes with significant drawbacks:
- Permanent loss of motion at the C7-T1 segment
- Adjacent segment disease: Increased stress on C6-C7 and T1-T2 discs above and below the fusion
- Hardware complications: Risks of plate migration, screw loosening, or pseudoarthrosis (failed fusion)
- Longer recovery: Typically 6-12 weeks before returning to normal activities
- Dysphagia risk: Difficulty swallowing affects 50% of patients immediately post-op, with 10-20% experiencing chronic symptoms
Posterior Foraminotomy: Some surgeons perform this procedure from the back of the neck, removing bone to enlarge the foramen and decompress the C8 nerve. While it preserves the disc, it requires significant muscle dissection and bone removal, potentially compromising spinal stability.
Cervical Disc Replacement: An emerging option that preserves motion, but data on cervical disc replacement at C7-T1 is limited. A recent case series found reasonable outcomes, but long-term data and FDA approval specifically for this level remain uncertain.1
The Ultra-Minimally Invasive Alternative: Deuk Laser Disc Repair®
At Deuk Spine Institute, we’ve developed an advanced endoscopic approach that addresses the limitations of traditional surgery while preserving your spine’s natural structure and function.
Deuk Laser Disc Repair® (DLDR) for C7-T1 disc problems uses a full-endoscopic technique performed through an incision of less than ¼ inch. The procedure addresses both the herniated disc material compressing the nerve AND the inflamed annular tear that’s the actual source of discogenic pain; something traditional surgery often overlooks.
How DLDR® Works at C7-T1:
- Precision Access: Using advanced imaging guidance, a tiny tubular retractor gently spreads muscle fibers without cutting them, creating a surgical corridor to the C7-T1 level
- Endoscopic Visualization: A high-definition endoscopic camera provides magnified, illuminated views of the surgical area—far superior to microscopic visualization used in traditional surgery
- Laser Decompression: A surgical-grade Holmium:YAG laser precisely vaporizes only the inflamed, damaged disc material, compressing the C8 nerve root
- Annular Tear Debridement: The laser debrides the painful annular tear, addressing the source of discogenic pain that fusion doesn’t treat
- Preservation of Structure: The healthy disc is left intact, spinal motion is maintained, and no hardware is implanted
Advantages of DLDR® Over Traditional C7-T1 Surgery:
- Outpatient procedure: Patients go home the same day
- Minimal incision: Less than ¼ inch compared to 1-2 inches for traditional approaches
- No fusion: Natural spinal motion is preserved at the critical cervicothoracic junction
- No hardware: No plates, screws, or cages that can loosen, migrate, or cause complications
- Rapid recovery: Most patients return to light activities within 1-2 weeks
- Published outcomes: 94.6% success rate with zero major complications in peer-reviewed studies12
- Addresses root cause: Treats both nerve compression AND the inflamed annular tear
Recent advances in full-endoscopic spine surgery have made procedures at the challenging C7-T1 level increasingly safe and effective. A 2024 case report on C7-T1 endoscopic foraminotomy demonstrated how modern navigation systems and endoscopic techniques allow precise decompression with minimal tissue damage, further supporting this technique.13
For more information on identifying authentic laser spine surgeons and understanding how ultra-minimally invasive endoscopic surgery differs from marketing-based “laser” procedures, see our comprehensive guide.14
A Patient’s Story: From Chronic Neck Pain to Pain-Free Life
Meet our 58-year-old patient from Massachusetts who had been dealing with severe neck pain radiating into his hand, along with thumb numbness that affected her daily life. After being told he needed spinal fusion, a procedure that would permanently eliminate motion in her neck and require a lengthy recovery, he refused and sought alternatives.
Eight months after undergoing Deuk Laser Disc Repair® and Deuk Plasma Rhizotomy® procedures, he returned to share his remarkable recovery story. “I’m pain-free.” “I can do everything I want to do.”
This case illustrates an important point: When patients are told fusion is their only option, seeking a second opinion from specialists in advanced minimally invasive techniques can reveal alternatives that preserve spinal function while eliminating pain.
The key to this patient’s success was finding a surgeon who addressed the root cause of his pain, the inflamed disc and nerve, rather than simply fusing the segment. His story demonstrates that even when conventional surgeons recommend fusion, motion-preserving alternatives may be available for properly selected patients.
Seeking Multiple Opinions: Making an Informed Decision
One of the most critical steps in managing a C7-T1 disc bulge is ensuring you have an accurate diagnosis and understanding of all your treatment options before making decisions about surgery.

Why Second Opinions Matter for Spine Surgery
The medical literature reveals significant variation in surgical decision-making for cervical disc problems. A 2025 systematic review found high variability in how motor and sensory deficits are defined and when surgery is recommended.15
This variability means different surgeons may offer vastly different recommendations for the same condition. One surgeon might recommend immediate fusion. Another might suggest conservative care. A third might offer motion-preserving endoscopic surgery.
Without multiple perspectives, you risk:
- Unnecessary fusion: Being recommended fusion when less invasive options could work
- Delayed appropriate treatment: Pursuing ineffective conservative care when you’re actually a surgical candidate
- Missing specialized options: Not learning about advanced techniques like DLDR that many surgeons don’t perform
Searching for a Second Opinion?
Upload your latest MRI today for a free virtual consultation and review with ultra minimally invasive surgeon, Dr, Ara Deukmedjian.

Finding Objective Assessment
The challenge with spine surgery is that most surgeons recommend what they know how to do, rather than what is best for the patient. A surgeon who only performs fusion will recommend fusion. A pain management specialist who doesn’t perform surgery will recommend injections. An endoscopic spine surgeon will evaluate whether you’re a candidate for minimally invasive approaches.
This is why seeking opinions from specialists with diverse skillsets helps you make truly informed decisions. The goal isn’t to “shop around until someone tells you what you want to hear.” It’s to gather comprehensive information from experts with different perspectives and techniques.
Questions to Ask During Consultations
When seeking second opinions, come prepared with specific questions:
- What is the exact source of my pain? Not all neck and arm pain comes from disc problems. Ensure your symptoms correlate with imaging findings.
- Have you personally reviewed my MRI images? Many physicians rely on radiology reports without examining the actual images themselves.
- What happens if I do nothing? Understanding the natural history helps you weigh the risks versus the benefits of intervention.
- What are all my treatment options? Not just the option that the surgeon performs, but comprehensive alternatives, including those they don’t offer.
- If you needed this surgery, what would you choose? This question often reveals what physicians really think about the treatments they recommend.
- What are your complication rates and outcomes for this specific procedure? Surgeons with published outcomes can show you their actual results, not just industry averages.
The Deuk Spine Free MRI Review
At Deuk Spine Institute, we offer free MRI reviews and virtual consultations for patients considering spine surgery. Dr. Deukmedjian personally reviews your imaging studies and performs a virtual physical examination via video consultation.
This provides a valuable second opinion from a surgeon who has published peer-reviewed research on minimally invasive cervical spine surgery and has performed over 2,700 Deuk Laser Disc Repair procedures with documented outcomes.
During the consultation, Dr. Deuk will:
- Confirm whether your symptoms match your imaging findings
- Explain whether you’re a candidate for DLDR or if other approaches are more appropriate
- Recommend conservative management if surgery isn’t necessary
- Provide an honest assessment of expected outcomes
Understanding Statistics: What Research Says About C7-T1 Disc Problems
Staying informed with current research helps you make evidence-based decisions about your care.
Epidemiology and Incidence
C7-T1 disc herniations account for 3.5-8% of all cervical disc herniations, making them significantly less common than C5-C6 (23%) or C6-C7 (45-60%) level problems.1 A large surgical series found that only 1.11% of cervical spine surgeries performed over 9 years were for isolated C7-T1 level pathology.2
Trauma Association
Research demonstrates a significant association between trauma and C7-T1 disc herniations (P < 0.0001) compared to disc problems at other cervical levels.2 This suggests that acute injury plays a more prominent role at this level than pure degeneration.
Unique Anatomic Characteristics
Studies show that 91.7% of C7-T1 herniations occur in the foraminal (lateral) location, while only 8.3% are central or paracentral.2 This lateral predominance differs markedly from that at more cephalad levels, where central/paracentral herniations are common.
The biomechanical explanation relates to the absence of uncovertebral joints (Luschka joints) at C7-T1. These structures, present at C3-C7, provide lateral reinforcement to the disc. Without them, the C7-T1 disc is more prone to lateral herniation.
Surgical Outcomes
For patients who require surgery, outcomes at C7-T1 are generally favorable when performed by experienced spine surgeons. Research on anterior approaches shows that most patients experience significant improvement in arm pain and weakness after decompression.3
Minimally invasive endoscopic approaches show particularly promising results. Published data on Deuk Laser Disc Repair® for cervical disc disease demonstrates 94.6% success rates with no major complications in prospective studies.12
Prevention and Long-Term Management: Protecting Your Cervicothoracic Junction
Whether you’ve already experienced C7-T1 disc problems or want to prevent them, specific strategies can protect this vulnerable area.
Rest And Activity Modification
The modern epidemic of “tech neck,” excessive forward head posture from smartphone and computer use, places tremendous stress on the lower cervical spine. For every inch your head moves forward from neutral alignment, the effective weight on your lower cervical spine increases by approximately 10 pounds.
As detailed in our comprehensive article on this topic, reversing tech neck requires:5
- Awareness: Recognizing when you’re in forward head posture
- Ergonomic corrections: Positioning screens at eye level
- Postural exercises: Chin tucks and cervical retraction exercises
- Strengthening: Building deep neck flexor strength to counteract forward head positioning
Biomechanically Sound Lifting Techniques
Given the strong association between trauma and C7-T1 disc problems, learning proper lifting mechanics is crucial:
- Keep loads close: Holding objects away from your body dramatically increases cervical spine load
- Avoid twisting while loaded: The combination of compression, flexion, and rotation is particularly damaging
- Use your legs: Squatting to lift rather than bending at the waist protects your entire spine
- Get help with heavy loads: There’s no shame in asking for assistance with awkward or heavy items
Occupational Considerations
Workers in high-risk occupations should be particularly vigilant. As discussed in our workers’ compensation guide, certain jobs place workers at elevated risk:7
- Construction workers: Heavy lifting, vibration exposure, awkward positions
- Manufacturing: Repetitive reaching overhead, sustained static postures
- Healthcare: Patient transfers, equipment lifting
- Desk workers: Prolonged sitting with forward head posture
If your job involves these risk factors, preventive strategies like proper ergonomics, regular breaks, and strengthening exercises become even more critical.

Chiropractic Care And Alternative Therapies
Chiropractic care and other alternative therapies may also be explored by patients with a C7-T1 bulging disc who wish to avoid invasive treatments.
Chiropractic adjustments focus on spinal manipulation to restore proper alignment. Chiropractors may use gentle spinal adjustments or mobilization techniques.
Some patients seek alternative therapies such as acupuncture, massage therapy, or osteopathic manipulation. It is important to note that not all alternative therapies are supported by clinical evidence.
Managing Cold Weather Effects
Many patients report worsening symptoms during cold weather. As explained in our article on cold weather and back pain, temperature changes can affect disc symptoms through several mechanisms:16
- Muscle tension increases in cold, reducing spinal support
- Reduced blood flow to discs may impair healing
- Barometric pressure changes may affect inflammation
- Decreased activity in winter reduces conditioning
Staying active during winter months, maintaining warm indoor temperatures, and continuing exercise programs can help minimize the effects of cold weather.
Your Path Forward
A C7-T1 bulging disc presents unique challenges due to the complex anatomy at the cervicothoracic junction. Understanding your condition, pursuing comprehensive conservative care when appropriate, and making informed decisions about surgical intervention when necessary are the keys to successful outcomes.
The most important points to remember:
- C7-T1 disc problems produce characteristic symptoms affecting the ring and little fingers, with intrinsic hand muscle weakness
- Trauma plays a significant role at this level compared to pure degeneration
- Conservative treatment should be comprehensive and time-limited (6-12 weeks)
- When surgery becomes necessary, motion-preserving endoscopic options like Deuk Laser Disc Repair® offer significant advantages over traditional fusion
- Seeking multiple opinions ensures you understand all available treatment options
- Prevention through proper ergonomics, postural correction, and biomechanically sound movement patterns protects your cervicothoracic junction long-term
If you’re struggling with C7-T1 disc symptoms, don’t wait for the problem to worsen. Early, appropriate intervention provides the best chance for full recovery and prevents the development of chronic weakness or nerve damage.
At Deuk Spine Institute, we’re committed to providing honest, evidence-based assessments and offering the full spectrum of treatment options, from conservative care to the most advanced minimally invasive procedures.
Upload your MRI for a free review and personal consultation with Dr. Ara Deukmedjian. Take the first step toward lasting relief and return to the activities you love, without the risks and limitations of spinal fusion.
Frequently Asked Questions
-
How long does it take for a C7-T1 disc bulge to heal naturally?
The timeline for natural healing varies significantly between patients. Many cases improve within 6-12 weeks with comprehensive conservative treatment, including physical therapy, activity modification, and anti-inflammatory measures. However, “healing” doesn’t necessarily mean the bulge disappears on imaging; rather, inflammation resolves and symptoms improve as the body stabilizes the area. Research shows that disc material can naturally reabsorb over several months in some cases. The key is symptom improvement rather than complete resolution of the bulge on MRI. If you haven’t experienced significant improvement after 12 weeks of appropriate conservative care, more advanced intervention should be considered.
-
Can C7-T1 disc problems cause permanent hand weakness?
Yes, if left untreated, prolonged compression of the C8 nerve root can lead to permanent weakness in the intrinsic hand muscles. Because the C8 nerve is predominantly composed of motor fibers controlling your hand’s small muscles, chronic compression can cause irreversible damage. Early warning signs include progressive weakness, visible muscle atrophy in the spaces between finger bones on the back of your hand, or worsening grip strength despite treatment. This is why timely intervention is crucial when conservative treatment fails; waiting too long risks permanent neurological deficits that cannot be reversed even with successful surgery.
-
Why is the C7-T1 level more difficult to treat surgically than other cervical levels?
The cervicothoracic junction presents unique surgical challenges due to its anatomy. The T1 vertebra sits behind the sternum; major blood vessels course through this region, and the thoracic duct, pleura, and the apex of the lung are nearby. Traditional anterior approaches may require a sternotomy or partial removal of the manubrium in some patients. Posterior approaches must navigate the transition from the mobile cervical spine to the fixed thoracic spine. Additionally, 91.7% of C7-T1 herniations occur in the foraminal (lateral) region rather than centrally, requiring specialized surgical techniques to access. This is why choosing a surgeon with specific experience at this level, particularly with advanced endoscopic techniques, is essential for optimal outcomes.
-
Sources
1: https://pmc.ncbi.nlm.nih.gov/articles/PMC9399142/
2: https://www.sciencedirect.com/science/article/abs/pii/S1878875018314931
3: https://pmc.ncbi.nlm.nih.gov/articles/PMC4949167/
5: https://deukspine.com/blog/tech-neck-forward-head-posture-treatment/
6: https://deukspine.com/blog/whiplash-delayed-pain-symptoms-treatment-12-04-2025/
7: https://deukspine.com/blog/workers-compensation-settlement-for-back-injury/
8: https://deukspine.com/blog/its-not-carpal-tunnel/
9: https://www.ncbi.nlm.nih.gov/books/NBK546618/
10: https://deukspine.com/blog/best-office-chairs-for-herniated-disc/
11: https://deukspine.com/blog/best-sleeping-positions-pillows-neck-pain-relief/
12: https://pubmed.ncbi.nlm.nih.gov/23776754/
13: https://www.e-neurospine.org/journal/view.php?number=1642
14: https://deukspine.com/blog/laser-spine-surgeons/
15: https://www.sciencedirect.com/science/article/pii/S2772529425014389
16: https://deukspine.com/blog/does-cold-weather-cause-back-pain/


