

By Dr. Ara J. Deukmedjian, MD
Board Certified Neurosurgeon
Reviewed on July 7, 2026
Disclaimer: The information contained within this article is for educational purposes only and is not a substitute for personalized medical advice.
Key Points
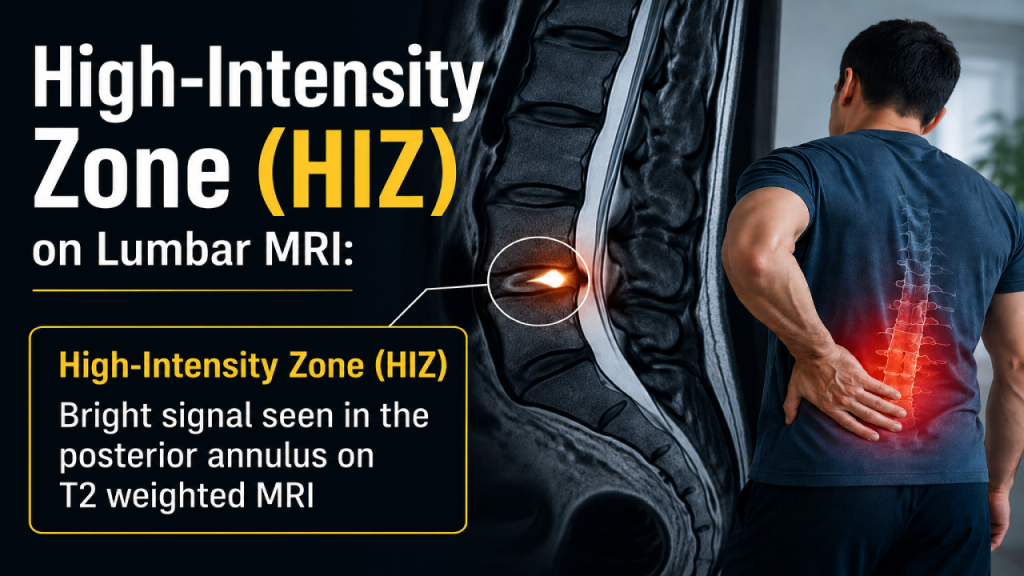
✓ A High-Intensity Zone (HIZ) is a bright, well-defined signal in the posterior annulus fibrosus of a lumbar disc, seen on T2-weighted MRI, first described by Aprill and Bogduk in 1992. ¹ ²
✓ Histologically, an HIZ corresponds to vascularized granulation tissue and inflammatory fluid trapped within an annular tear not simply a “dry” fissure. ³ ⁴
✓ HIZ is strongly associated with discogenic low back pain, with reported specificity of 83–95% for concordant pain on provocation discography, though sensitivity varies widely (25–97%) across studies. ⁵
✓ An HIZ is not always symptomatic. HIZs have been documented in asymptomatic volunteers, so diagnosis must correlate the imaging with clinical exam findings. ⁵ ⁶
✓ HIZ lesions can act as a precursor to disc extrusion; the weakened annular segment is where a future herniation is most likely to occur. ⁷
✓ Fusion is almost never the correct first-line treatment for an isolated HIZ. Motion-preserving endoscopic options directly address the annular tear without sacrificing the disc or spinal segment. ⁸
✓ At Deuk Spine Institute, Deuk Laser Disc Repair® treats the annular tear responsible for HIZ pain through a 7 mm incision, with a published 99.6% success rate and 0.01% complication rate.
The Quick Answer
If your MRI report mentions a “high-intensity zone” or “HIZ” in one of your lumbar discs, it means the radiologist has identified a bright spot in the back wall of the disc. A fluid-filled tear in the annulus fibrosus that is very often the source of chronic low back pain. ¹ ³
The problem is what typically happens next. Many patients are told the only solution is a spinal fusion at the affected level. That is rarely true. An HIZ is a localized tear in the outer disc wall, and localized problems deserve localized solutions. A skilled endoscopic spine surgeon can treat the exact painful segment of the annulus through a 7 mm incision, preserving the disc, the bone, the ligaments, and normal motion. ⁸ ⁹
This article explains what an HIZ actually is on your MRI, why it hurts, how it is diagnosed, what non-surgical options are appropriate first, and which surgical options preserve your spine.
What Is a High-Intensity Zone?
A High-Intensity Zone is a focal, well-defined area of increased signal intensity in the posterior annulus fibrosus of an intervertebral disc, visible on T2-weighted magnetic resonance imaging. ¹ It appears as a small, bright dot or comma-shaped mark at the back edge of an otherwise darker, degenerated disc.
The HIZ was first described by Aprill and Bogduk in 1992 in a landmark paper correlating the finding with positive provocation discography. ² Since then, dozens of studies have refined our understanding of what the bright spot actually represents.
What the HIZ represents pathologically
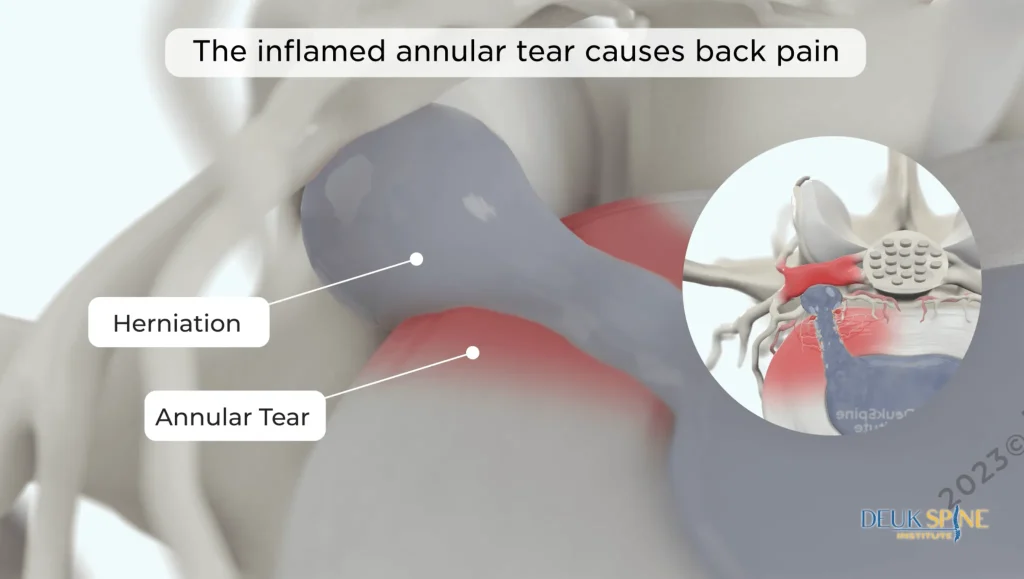
An HIZ is not just “a bright spot.” Histological studies of surgically excised HIZ discs have shown consistent findings: ³ ⁴
- A radial or concentric annular tear extending into or through the outer third of the annulus fibrosus.
- Vascularized granulation tissue new blood vessels and inflammatory cells that have grown into the tear as the body attempts to heal it.
- Fluid or mucoid nuclear material trapped between torn annular lamellae, which is what produces the bright T2 signal.
- Nerve ingrowth into a region of the annulus that is normally not innervated, which is the mechanical basis for why the tear hurts. ³
In other words, an HIZ is an inflamed, innervated, healing-but-not-healed tear in the back wall of the disc. That combined with a small tear plus inflammation is a well-established recipe for chronic axial low back pain. ³ ⁴
HIZ vs. herniated disc vs. degenerative disc
These terms are frequently confused. They describe different but related things:
- Degenerative disc disease is a chronic loss of disc height, hydration, and structural integrity, seen on MRI as a “black disc.”
- HIZ is a focal tear within the outer annulus of that disc, often in an otherwise moderately preserved-looking disc.
- Disc herniation is displacement of nuclear material through a tear in the annulus, producing a bulge or extrusion that can compress a nerve.
An HIZ can exist on its own, causing purely axial low back pain without leg symptoms, or it can progress. Case series have documented HIZs that later extruded through the same weakened annular segment and produced classic radicular leg pain. ⁷ For that reason, an HIZ should never be dismissed as an incidental finding without a proper clinical evaluation.
Symptoms of an HIZ
The classic clinical presentation of a painful HIZ is:
- Chronic, deep, midline or paramedian low back pain, usually at the L4-L5 or L5-S1 level, which is where the majority of HIZ lesions occur. ¹⁰
- Pain that is worse with sitting, bending forward, coughing, or sneezing. Anything that raises intradiscal pressure.
- Pain that is relieved by lying flat.
- Pain that has often been present for more than 6 months and has failed conservative care.
- Frequently no leg pain and no neurological deficit, because the tear itself does not compress a nerve root; the pain is from the tear.
When an HIZ patient does have leg symptoms, it is usually because the annular tear has begun to leak inflammatory chemicals onto the adjacent nerve root, or because a small extrusion has developed through the same segment of annulus. ⁷
How an HIZ Is Diagnosed
1. MRI
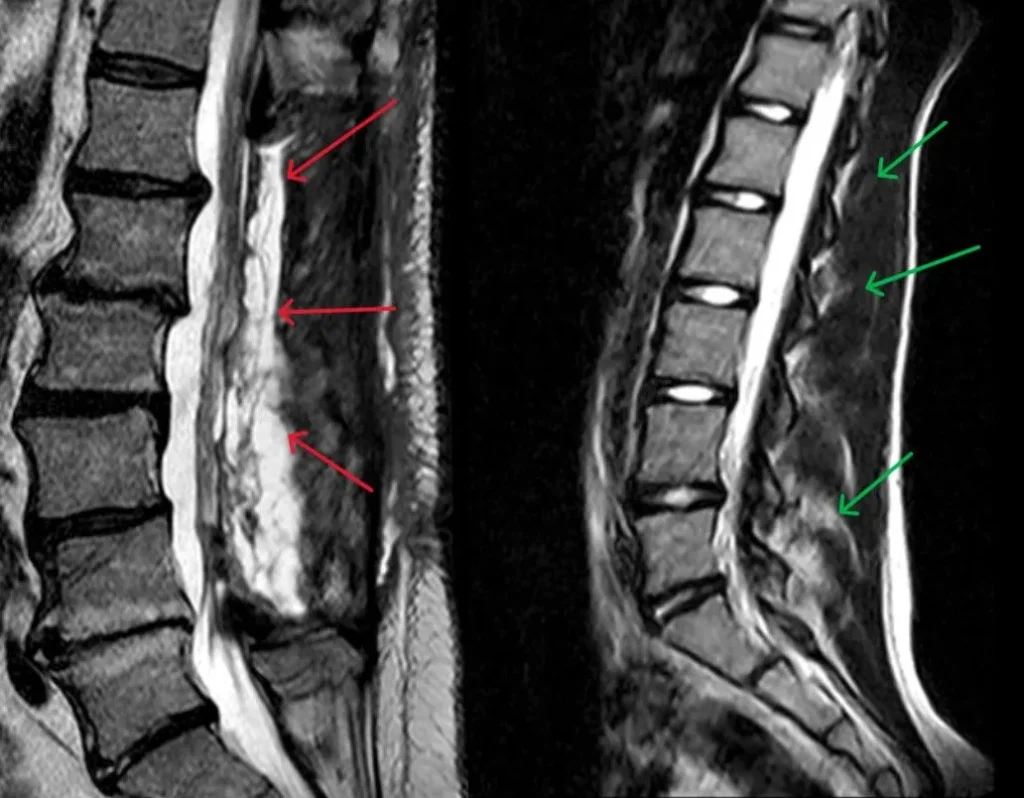
A high-quality T2-weighted lumbar MRI is the imaging test of choice. The HIZ appears as a bright, well-defined focus in the posterior annulus of the affected disc, distinct from the darker signal of the surrounding degenerated annulus. ¹ ² Modern high-resolution MRI can also detect nonconsecutive or subtle HIZ signals that older scanners missed. ⁶
2. Clinical correlation
An HIZ finding is only meaningful when it matches the patient’s symptoms. Because HIZs have been documented in asymptomatic individuals, the imaging finding must correlate with a clinical picture consistent with discogenic pain. Axial back pain worsened by loading, relieved by unloading, and without another obvious source. ⁵ ⁶
3. Provocation discography
Historically, provocation lumbar discography was used to confirm that an HIZ disc was the true pain generator by reproducing the patient’s typical pain when the disc was pressurized. Reported specificity of HIZ for concordant discography is high (83–95%), which is why it remains a useful screening finding, but sensitivity is variable. ⁵ Discography is invasive and is used selectively today, typically when surgical planning depends on definitively identifying the pain generator.
4. Diagnostic anesthetic injection
An intradiscal or transforaminal anesthetic block can serve as a less invasive way to confirm that the suspected disc is producing the pain.
Causes of High-Intensity Zones
HIZ lesions develop because the outer annulus fibrosus has been mechanically injured. Common contributors include:
- Repetitive flexion and rotational loading (heavy lifting with a twist)
- Acute injury: a fall, motor vehicle collision, or lifting event
- Age-related annular degeneration, which weakens the collagen lamellae
- Genetic predisposition to early disc degeneration
- Prior disc injury at the same level

Most HIZ patients cannot identify a single moment of injury. The tear develops through repeated microtrauma over months or years, and only becomes clinically important once inflammation and nerve ingrowth reach a threshold that produces pain. ³
Non-Surgical Treatment for HIZ
Not every HIZ needs surgery. A structured course of conservative care should almost always come first, and for a meaningful percentage of patients it is enough:
- Activity modification to reduce compressive and flexion loading of the disc.
- Physical therapy focused on core stabilization, hip mechanics, and neutral-spine loading not passive modalities.
- NSAIDs for the inflammatory component of HIZ pain, when medically appropriate.
- Epidural steroid injection, which can reduce annular and perineural inflammation and give some patients durable relief.
- Time. Some annular tears do heal, particularly in younger patients with good disc hydration.
If symptoms persist beyond 3–6 months of appropriate conservative care, or if pain is disabling from the outset, targeted treatment of the annular tear itself becomes the next reasonable step.
Surgical Treatment for HIZ
This is where patients are most commonly given the wrong recommendation. A single-level HIZ with no instability, no deformity, and no significant nerve compression does not require a fusion. Removing an entire disc and bolting two vertebrae together to treat a small tear in the back wall of that disc is disproportionate to the actual pathology and carries a documented long-term risk of adjacent-segment degeneration. ⁸
Endoscopic annular repair and thermal annuloplasty
Percutaneous endoscopic techniques allow direct visualization of the posterior annulus through a working channel roughly 7 mm in diameter. The surgeon can see the annular tear on a magnified video display, remove degenerated nuclear material that is leaking into the tear, and use a precisely controlled radiofrequency or laser probe to seal the tear and denervate the ingrown pain fibers within the annulus. ⁹ ¹¹
Because no bone is removed, no muscle is cut, and no hardware is placed, this approach preserves the disc, the facet joints, and normal motion at the treated level.
Deuk Laser Disc Repair®
Deuk Laser Disc Repair® (DLDR) is a specific outpatient, endoscopic, laser-based technique developed by Dr. Ara Deukmedjian to treat exactly this category of pathology: annular tears, HIZ lesions, contained herniations, and other discogenic sources of pain. The procedure is performed through a 7 mm incision under local anesthesia and light sedation. The laser precisely removes a small amount of disc producing the pain while leaving the healthy disc, bone, and ligaments.
Across more than 2,700 Deuk Laser Disc Repair procedures, the reported success rate is 99.6% with a complication rate of 0.01%. And most patients return to normal activity within 72 hours.
Why Endoscopic Treatment Fits HIZ Pathology
For a lesion as focal as an HIZ, endoscopic treatment offers measurable advantages over open decompression or fusion, most of which come from what the surgeon doesn’t have to do.
Direct visualization of the tear
Under endoscopic magnification with continuous saline irrigation, the surgeon can see the exact edge of the annular tear, the granulation tissue within it, and the ingrown nerve fibers responsible for the pain. That level of visualization is not possible through open techniques. ⁹
Preservation of the disc
An HIZ is a tear in a disc that is otherwise still working. Endoscopic annular repair treats the tear without removing the disc. Fusion, by contrast, requires complete discectomy at the level, permanently sacrificing motion.
Lower biomechanical liability
Motion-preserving procedures do not create the adjacent-segment stress that follows fusion. Patients who undergo lumbar fusion have a documented risk of adjacent-segment degeneration at the level above or below the fusion, which can drive additional surgery years later. ⁸
Faster recovery
Because muscle, bone, and ligament are preserved. Patients undergoing endoscopic procedures typically go home the same day, walk within hours, and return to sedentary work within a week.
How to Choose the Right Surgeon for an HIZ
Endoscopic spine surgery is one of the most technically demanding subspecialties in spine care. And outcomes vary widely by surgeon. Case-volume studies show a defined learning curve of 20–40+ cases before complication rates and operative times stabilize. ¹² Use these criteria when evaluating a surgeon for HIZ treatment:
- Board certification by the American Board of Neurological Surgery or the American Board of Orthopaedic Surgery, plus fellowship training that specifically included endoscopic spine surgery.
- Endoscopic case volume. Ask directly how many endoscopic procedures the surgeon has personally performed in the past 12 months. A high-volume endoscopic surgeon and a fusion surgeon who occasionally does endoscopic work are not equivalent.
- Published outcomes a reputable high-volume endoscopic surgeon can quote their own success and complication rates.
- A proportional treatment plan. If fusion is the first recommendation for a single-level HIZ without instability, get a second opinion.
- Independent patient reviews on sites like Healthgrades, Vitals, and Google, for the individual surgeon rather than the practice.
Treat the annular tear without removing the disc.
A High-Intensity Zone is a small, localized tear in the back wall of your disc and a small tear deserves a small solution, not a fusion. Send your MRI for a free review by Dr. Deukmedjian and learn whether Deuk Laser Disc Repair® can seal the tear directly through a 7 mm incision, with the disc, the bone, the ligaments, and your natural motion left intact.
- 99.6%
- Average pain relief
- 0.01%
- Complication rate
- 7mm
- Incision, outpatient
FAQs
Is an HIZ on my MRI always painful?
No. HIZs have been observed in asymptomatic individuals in every large imaging study on the subject. ⁵ ⁶ The imaging finding must correlate with clinical symptoms. Is a deep axial low back pain worsened by sitting or loading and relieved by lying flat is the classic pattern. A radiologist reporting an HIZ is describing what they see; the treating physician determines whether that HIZ is your pain generator.
Can an HIZ heal on its own?
Some do. The granulation tissue and vascular ingrowth found within HIZ lesions represent the body’s attempt to repair the annulus. ³ In younger patients with well-hydrated discs, a period of activity modification, physical therapy, and inflammation control is often enough. In patients with persistent symptoms beyond 3–6 months, the tear has generally reached a chronic, self-perpetuating state and needs direct treatment.
Does an HIZ mean I will eventually herniate?
Not always, but the risk is real. Case reports have documented HIZ lesions that progressed to disc extrusion through the same weakened segment of annulus, producing radicular leg pain. ⁷ Treating an HIZ before it extrudes preserves more options.
Do I need a fusion for an HIZ?
Almost never as a first-line treatment. A single-level HIZ without instability, deformity, or significant nerve compression can be treated with a motion-preserving endoscopic procedure that addresses the annular tear directly. ⁸ ⁹ Fusion is a reasonable option only for patients with documented instability or after other appropriate treatments have failed.
What is the success rate of endoscopic treatment for HIZ?
For appropriately selected patients, endoscopic annular repair and thermal annuloplasty produce meaningful pain relief in the great majority of cases. ⁹ ¹¹ Deuk Laser Disc Repair®, a specific endoscopic-laser technique used at Deuk Spine Institute for HIZ and other discogenic pain, has a published success rate of 99.6% across more than 2,000 procedures.
How long is recovery after endoscopic HIZ treatment?
Most patients are discharged the same day, walking within hours, and back to sedentary work within 3–7 days. Return to full activity typically takes 4–6 weeks depending on the patient.
Does insurance cover endoscopic treatment for HIZ?
Most major U.S. insurance plans, Medicare, and workers’ compensation cover medically necessary endoscopic spine procedures, though coverage for specific advanced techniques varies by carrier. Deuk Spine Institute verifies benefits during a free MRI review.
Sources
View Sources
- Aprill C, Bogduk N. High-intensity zone: a diagnostic sign of painful lumbar disc on MRI. Br J Radiol. 1992.
- Peng B, et al. Pathogenesis and clinical significance of HIZ on MR imaging. Eur Spine J. 2006.
- Peng B, et al. The pathogenesis of discogenic low back pain. J Bone Joint Surg Br. 2005.
- Kang Y, et al. Imaging analysis of the HIZ on lumbar MRI. J Pain Res. 2021.
- Murtagh RD, et al. Annular fissures and HIZ at provocation discography. AJNR. 2023.
- Liu C, et al. Correlation between HIZ on MRI and discography. Medicine. 2017.
- Sharma A, et al. Lumbar annular HIZ as a precursor to disc extrusion. Cureus. 2021.
- Hilibrand AS, Robbins M. Adjacent segment degeneration after fusion. Spine J. 2004.
- Hasan S, et al. The benefit zone of full-endoscopic spine surgery. J Spine Surg. 2019.
- Wang ZX, Hu YG. HIZ on T2-weighted MRI: distribution and correlation with LBP. Eur Spine J. 2012.
- Tsou HK, et al. Discoscopic findings of HIZs on lumbar MRI. Asian Spine J. 2014.
- Ahn Y, et al. Learning curve for interlaminar endoscopic lumbar discectomy. World Neurosurg. 2021.


