


By Dr. Ara Deukmedjian, MD
Board Certified Neurosurgeon
Reviewed on July 9, 2026
Disclaimer: The information contained within this article is for educational purposes only and is not a substitute for personalized medical advice.
Key Points
✓ Foraminal stenosis is narrowing of the neural foramen. The bony tunnel where a spinal nerve root exits the spine; causing pinched-nerve pain. ¹
✓ It most commonly affects L4-L5 and L5-S1 in the lower back, and C5-C6 and C6-C7 in the neck. ² ³
✓ Symptoms include one-sided burning, shooting, or electric pain, numbness, tingling, and weakness in the arm or leg. ¹ ⁴
✓ Pain typically worsens with leaning back and improves with leaning forward. ⁴
✓ MRI is the diagnostic standard, but symptoms and exam findings must match the imaging. ⁵
✓ Most patients improve with 6–12 weeks of physical therapy, NSAIDs, and, if needed, a transforaminal epidural steroid injection. ⁶
✓ Fusion is rarely necessary and carries a long-term risk of adjacent-segment degeneration. ⁹
✓ Full-endoscopic transforaminal decompression relieves the pinched nerve through a 7 mm incision. No bone removal, no muscle cutting, no hardware. ⁷ ⁸
✓ Deuk Laser Disc Repair® has a 99.6% success rate and 0.01% complication rate across 2,700+ procedures.
The Quick Answer
If your MRI report says “foraminal stenosis” and your surgeon has recommended a laminectomy or fusion stop and get a second opinion. Foraminal stenosis is a nerve-compression problem. Not a whole-spine problem. In the great majority of cases, the disc bulge, bone spur, or thickened ligament. Can be removed through a 7 mm endoscopic procedure under local anesthesia. In under an hour, without cutting muscle, removing the lamina, or placing hardware. ⁷ ⁸
The fusion procedure fuses two vertebrae together and poses a proven risk of adjacent segment degeneration above or below the fused joint level. ⁹ This is not required for normal foraminal stenosis where there’s no instability.
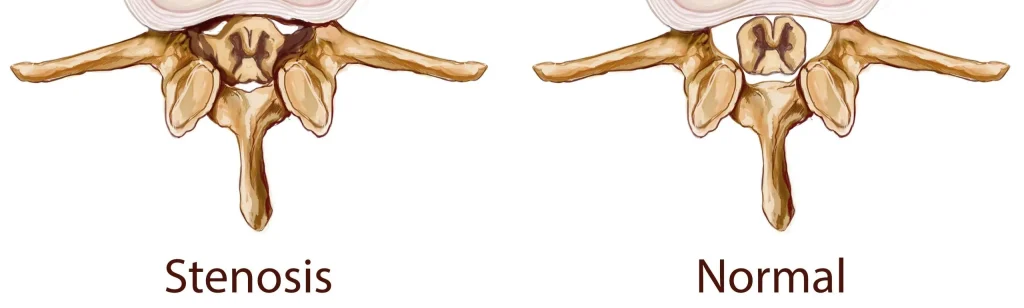
What Is Foraminal Stenosis?
Every two vertebrae in your back form a tiny tunnel known as the neural foramen. Through this tunnel comes out one spinal nerve root which travels to your arm, chest or leg. Narrowing of this tunnel causes compression of this nerve. And as a result, the muscles and the skin supplied by the nerve start sending painful messages.
That narrowing is called “foraminal stenosis“. It is a type of lateral spinal stenosis, distinct from central canal stenosis (which compresses the spinal cord or cauda equina) and lateral recess stenosis (which pinches the nerve just before it enters the foramen). ¹ ⁴
Foraminal stenosis can occur at any level of the spine, but is most symptomatic in:
- Lumbar spine: Producing sciatica down the leg. ²
- Cervical spine: Producing radiating shoulder, arm, and hand pain (cervical radiculopathy). ³
What narrows the foramen
The foramen is bordered by the vertebral body and disc in front, the facet joint behind, and the pedicles above and below. Anything that encroaches on that space can pinch the exiting nerve:
- Disc height loss and disc bulge. As a disc dehydrates with age, the vertebra above it settles down. The foramen which is bordered by the disc collapses vertically. A posterolateral disc bulge can compress the existing nerve. ¹ ¹⁰
- Facet joint hypertrophy. The facet joint enlarges and grows bone spurs in response to arthritic wear, encroaching into the foramen from behind. ¹
- Ligamentum flavum thickening. The elastic ligament that lines the back of the canal thickens with age and can bulge into the foramen. ¹
- Spondylolisthesis. When one vertebra slips forward on the one below, the foramen shears and narrows. ¹ ¹⁰
- Herniated disc. A far-lateral (foraminal) disc herniation compresses the existing nerve directly inside the tunnel. ⁴
- Congenitally short pedicles. Some people are simply born with tighter foramina. Symptoms tend to emerge earlier in life. ¹
Foraminal stenosis is degenerative in most patients over 50 and is closely related to what radiologists call “degenerative disc disease” and “spondylosis”. Labels that describe the same aging process from different angles. ¹⁰
Symptoms of Foraminal Stenosis
Foraminal stenosis produces radiculopathy. Pain and neurologic symptoms that follow the path of a single, specific nerve root. Because only one nerve is pinched, symptoms are typically one-sided and follow a predictable pattern.
Lumbar foraminal stenosis (leg symptoms)
- (L4 nerve root): Pain down the front and side of the thigh and shin, weak ankle dorsiflexion (“foot drop”). ²
- (L5 nerve root): Pain down the side of the leg to the top of the foot and big toe, weak great-toe extension. ²
- (S1 nerve root): Pain down the back of the leg to the heel and outer foot, weak plantarflexion, diminished ankle reflex. ²
Cervical foraminal stenosis (arm symptoms)
- (C6 nerve root): Pain into the shoulder, biceps, and thumb. Weak biceps and wrist extension. ³
- (C7 nerve root): Pain into the triceps and middle finger. Weak triceps and wrist flexion; diminished triceps reflex. ³
Positional pattern
Symptoms of foraminal stenosis characteristically worsen with extension and improve with flexion. That is because extending the spine (arching backward) further narrows the foramen. While flexing (leaning forward) opens it. Patients often report:
- Leg pain that comes on with prolonged standing or walking downhill. And is relieved by leaning forward on a shopping cart. ⁴
- Neck and arm pain that worsens with looking up. And is eased by tilting the head away from the painful side.
This positional signature is one of the most useful features in distinguishing foraminal stenosis from other causes of arm or leg pain. And is one of the reasons a good clinical exam still matters more than the MRI report alone. ⁴
How Foraminal Stenosis Is Diagnosed
1. History and physical exam
A skilled spine specialist will map the exact distribution of your pain. This includes a strength test and reflexes level-by-level, and performing provocative maneuvers. The Spurling test for cervical foraminal stenosis and the straight-leg raise and extension-based testing for lumbar. A textbook exam alone can often predict the pinched level before any imaging is reviewed.

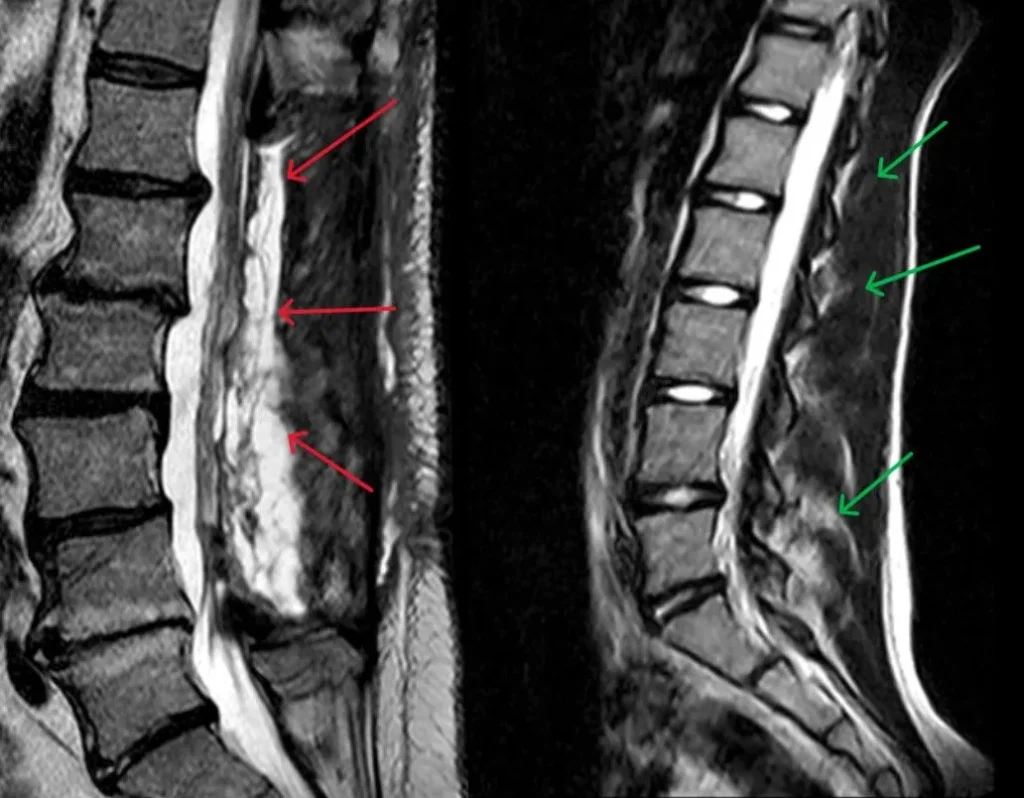
2. MRI
MRI is the imaging test of choice for foraminal stenosis. It shows the disc, ligaments, facet joints, and nerve roots in soft-tissue detail. Radiologists commonly grade lumbar foraminal stenosis using the Lee classification (Grade 0 = normal, Grade 3 = complete obliteration of perineural fat with nerve-root collapse). ⁵
3. CT and CT myelogram
CT is superior for showing bony detail: osteophytes, pedicle anatomy, and facet arthrosis. A CT myelogram is reserved for patients who cannot have an MRI or when the MRI is ambiguous. ¹
4. Electrodiagnostic studies (EMG/NCS)
When the level of nerve involvement is not clear or symptoms do not match imaging. An EMG can objectively confirm which nerve root is irritated.
The “MRI does not equal diagnosis” caveat
Population studies have found that asymptomatic adults over age 50 display signs of degeneration: disc bulges, foraminal narrowing, and facet joint arthrosis on MRI in up to 80-90% of cases. ¹¹ The MRI is one of those pieces of evidence. Symptoms, physical examination findings, and imaging findings must all be consistent with the same nerve root being irritated in order to blame that particular nerve root. Surgery based on the MRI alone is a red flag.
Non-surgical Management of Foraminal Stenosis
The majority of patients suffering from foraminal stenosis do not require surgery. Both national guidelines from the North American Spine Society and results from the SPORT trial recommend a period of 6 to 12 weeks of non-operative treatment for most patients with radiculopathy. ⁶ ¹²
Non-Surgical Treatment of Foraminal Stenosis
Most patients with foraminal stenosis improve without surgery. National guidelines from the North American Spine Society and long-term data from the SPORT trial both support an initial 6–12 week course of non-operative management for most patients with radiculopathy. ⁶ ¹²
Physical therapy
Directed physical therapy for foraminal stenosis is flexion-biased. Techniques that open the foramen, including postural retraining, hip-hinge mechanics, core stabilization. And in some cases traction. Avoid extension-loaded programs early on; they often make things worse.
Activity modification
Short-term relative rest, ergonomic adjustments. A supportive chair, monitor height corrections for cervical cases. And pacing of upright activities can meaningfully reduce nerve irritation while inflammation subsides.
Medication
NSAIDs are the first-line pharmacologic option. Short courses of oral steroids are used in select acute cases. Opioids are not appropriate long-term treatment for foraminal stenosis and do not treat the underlying compression.

Transforaminal epidural steroid injection
For patients whose pain has not settled after several weeks of conservative care, an image-guided transforaminal epidural steroid injection delivers steroids directly at the offending nerve root. It can provide meaningful relief and, importantly, helps confirm the pain generator before any surgery is considered. ⁶
When conservative care is not enough
Non-surgical care fails when:
- Symptoms persist despite 6–12 weeks of appropriate treatment
- Weakness is present or progressing
- Pain is severe enough to disable normal daily function
- There are red-flag features (bowel/bladder changes, saddle numbness. These require urgent evaluation
At that point, decompression should be discussed. But the type of decompression matters enormously.
Surgical Treatment: The Case Against Fusion First
The standard surgical solution for foraminal stenosis used to be open decompression, which included fusions, laminectomies, foraminotomies, and rods-and-screws instrumentation to stabilize the level. This procedure had been developed at a time when there was no such thing as high-definition endoscopy. And it treats the entire spinal segment for what is. In most cases, a focal nerve-compression problem.
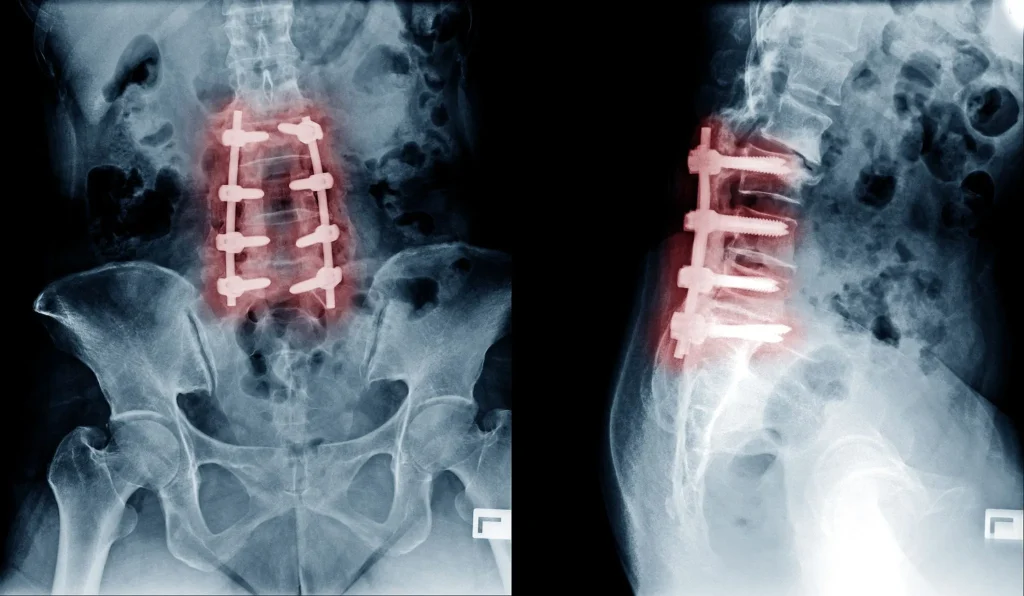
Fusion has three durable costs:
- Loss of motion at the fused level, forever. ⁹
- Adjacent-segment degeneration. Levels above and below a fusion carry more mechanical load and develop new symptomatic degeneration at a documented rate over the following decade. ⁹
- Long recovery. Open decompression and fusion typically involves an inpatient stay, weeks off work, and months of restricted activity.
The critical question is whether your specific foraminal stenosis actually requires that trade. In the absence of documented instability (spondylolisthesis with motion on flexion-extension x-rays), the answer for most patients is no. ⁶ ¹²
The Endoscopic Alternative: Full-Endoscopic Transforaminal Decompression

Full-endoscopic transforaminal decompression is the modern, ultra-minimally-invasive treatment of choice for foraminal stenosis in appropriately selected patients. ⁷ ⁸
How it works
- A 7 mm skin incision is made off the midline under fluoroscopic guidance.
- A tubular dilator is passed between paraspinal muscles. The muscles are spread, not cut.
- A high-definition endoscope with an integrated working channel is advanced directly into the foramen under continuous saline irrigation.
- Under magnified live video, the surgeon uses precision instruments: micro-graspers, a side-firing laser, and radiofrequency probes. To remove the exact offender: a bone spur, a hypertrophic ligament, or a foraminal disc herniation. The lamina, facet joint, and spinal ligaments are preserved. ⁷ ⁸
- The instruments are withdrawn and the incision closed with a single stitch or skin adhesive.
Because no bone is cut and no structural element of the spine is removed, the procedure is motion-preserving. There is no fusion, no hardware, and no biomechanical liability for the adjacent levels.
What the evidence shows
- Randomized and prospective studies of full-endoscopic decompression for lumbar foraminal stenosis and foraminal disc herniation report clinical success rates in the 85–95% range, with outcomes equivalent or superior to open microdiscectomy. ⁷ ⁸
- Reported major complication rates in large endoscopic series are on the order of 1.5–3.4%, comparable to or lower than open microsurgical decompression. ⁸ ¹³
- Patients are typically discharged the same day, walking within hours, and back to sedentary work within a week. ⁷
Deuk Laser Disc Repair® for foraminal stenosis
Deuk Laser Disc Repair® is our proprietary endoscopic-laser decompression developed and refined by Dr. Deukmedjian over more than 15 years of dedicated endoscopic practice. When the pain generator in foraminal stenosis is a bulging or herniated disc, DLDR® uses a side-firing holmium laser through a 7 mm working channel to precisely ablate the offending disc tissue and relieve the nerve. Under local anesthesia, as an outpatient. Across more than 2,000 procedures, DLDR® has a published 99.6% success rate and 0.01% complication rate, and the vast majority of patients return to normal activity within 72 hours.
Who Is a Candidate. And Who Isn’t
Endoscopic decompression is not appropriate for everyone. It is best suited for patients with:
- Symptomatic foraminal stenosis correlated to a specific nerve root
- Failure of 6–12 weeks of appropriate conservative care
- MRI-confirmed foraminal narrowing at 1–2 levels
- No radiographic instability
It is less appropriate for patients with:
- Severe central canal stenosis with myelopathy
- Documented instability (spondylolisthesis with dynamic motion)
- Fracture, tumor, or infection
- Multi-level severe deformity
These conditions may still require a more traditional decompression or a fusion. An honest surgeon will tell you which category you are in.
How to Choose the Right Surgeon for Foraminal Stenosis
Not every “minimally invasive” surgeon performs full-endoscopic work, and outcomes in endoscopic surgery are strongly surgeon-dependent. A defined learning curve of 20–40+ cases is required before complication rates and operative times stabilize. ¹⁴
Before consenting to any procedure, ask:
- Are you board certified and fellowship trained? In neurological surgery, orthopedic spine surgery, or through the American Board of Spine Surgery.
- How many endoscopic decompressions have you personally performed in the last 12 months? Not lifetime. Recent volume matters.
- What is your published success and complication rate? A high-volume endoscopic surgeon can quote their own outcome data.
- Why do you recommend this specific procedure over the alternatives? The plan should be proportional to the pathology.
- What will you not do? A surgeon who defaults to fusion for every foraminal stenosis is not the right surgeon for a focal nerve-compression problem.
- Have you gotten a second opinion? If a fusion has been recommended, get one. It costs a phone call and can prevent an irreversible surgical decision.
Free the pinched nerve without fusing your spine.
Foraminal stenosis is a focal nerve-compression problem, not a whole-spine problem. Before you consent to a laminectomy or fusion, send your MRI for a free review by Dr. Deukmedjian and learn whether Deuk Laser Disc Repair® can decompress the exact bone spur, ligament, or disc pinching your nerve through a 7 mm incision — under local anesthesia, in under an hour, with the lamina, facet joints, and motion of your spine preserved.
- 99.6%
- Average success rate
- 0.01%
- Complication rate
- 7mm
- Incision, outpatient
FAQs
What is the main cause of foraminal stenosis?
Age-related degeneration is the primary causative factor, characterized by reduction in disc height, facet joint arthropathy with bone spurs, and ligamentum flavum thickening, which encroach on the foraminal space where the nerve root exits. ¹ ¹⁰ The other factors that can be implicated are far lateral disc prolapse, spondylolisthesis, and congenital short pedicles.
Can foraminal stenosis heal on its own?
While the bony narrowing does not get reversed, the symptoms usually will. The symptoms tend to improve significantly in a majority of patients who develop radiculopathy due to foraminal stenosis in 6-12 weeks due to the subsiding inflammatory process affecting the pinched nerve. ⁶ ¹² Narrowing that is asymptomatic does not need any treatment.
What is the difference between foraminal stenosis and spinal stenosis?
“Spinal stenosis” most commonly means narrowing of the central spinal canal, or in other words, compression of the spinal cord/cauda equina, causing bilateral leg problems on walking. Lateral canal narrowing is called foraminal stenosis; it results in one-sided leg pains, involving a certain nerve root only. ¹ ⁴ Some patients suffer from both.
Is foraminal stenosis a disability?
Whether or not this is considered to be a disability would depend on the functional impairment caused by this condition. Foraminal stenosis that is severe and untreated, resulting in weakness or radicular pain that cannot be controlled, can be classified as a disability. However, the treatment for this problem is usually effective. ⁷ ⁸
Do I need surgery for foraminal stenosis?
Most patients do not. National guidelines recommend an initial 6–12 week course of conservative care for lumbar and cervical radiculopathy in the absence of red flags. ⁶ ¹² Surgery is considered when conservative care fails, when there is progressive weakness, or when pain is severe and disabling. Even then, the surgery does not need to be a fusion.
Is fusion necessary for foraminal stenosis?
Almost never, unless there is documented instability. Foraminal stenosis is a focal nerve-compression problem, and a focal endoscopic decompression addresses it without the long-term cost of adjacent-segment degeneration that fusion carries. ⁷ ⁸ ⁹ If fusion has been recommended for uncomplicated foraminal stenosis, get a second opinion.
How successful is endoscopic surgery for foraminal stenosis?
Published outcomes for full-endoscopic transforaminal decompression report meaningful improvement in pain and function in approximately 85–95% of appropriately selected patients at 1–2 years — statistically equivalent to or better than open microdiscectomy, with less blood loss, shorter hospital stays, and faster return to work. ⁷ ⁸ Deuk Laser Disc Repair®, our specific endoscopic-laser technique, reports a 99.6% success rate across more than 2,000 procedures.
How long does recovery take after endoscopic foraminal decompression?
Most patients are discharged the same day, walking within hours, and back to desk work within 3–7 days. Return to full activity typically takes 4–6 weeks depending on the procedure and the patient. ⁷
Does insurance cover endoscopic decompression for foraminal stenosis?
Most major U.S. insurance plans, Medicare, and workers’ compensation cover medically necessary endoscopic spine procedures, though coverage for specific advanced techniques varies by carrier. Deuk Spine Institute verifies benefits during a free MRI review.


