
By Dr. Ara Deukmedjian, MD
Board-Certified Neurosurgeon, Deuk Spine Institute
Medically reviewed on February 24, 2026
Medical disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
Key Points
Before diving into the details, here's what you need to know about back surgery:
✓ Most back pain resolves without surgery - 75-90% of patients improve with conservative treatment within 3-6 months
✓ Surgery outcomes vary dramatically by procedure - 25-33% of microdiscectomy patients report poor outcomes despite "successful" surgery
✓ Timing matters for surgical success - Longer symptom duration before surgery correlates with worse outcomes
✓ Not all "minimally invasive" procedures are equal - True minimally invasive surgery uses 4-7mm incisions, not 1-inch cuts
✓ Traditional fusion has significant long-term risks - 11-36% develop adjacent segment disease requiring additional surgery
✓ Motion-preserving alternatives exist - Deuk Laser Disc Repair® has 99.6% success rate with zero complications
✓ Recovery times differ drastically - Fusion requires 6-12 months vs. days for advanced endoscopic procedures
✓ Technology is rapidly advancing - Robotics, AI, and navigation systems are improving surgical precision
✓ Second opinions are essential - Many surgeons only offer what they're trained to perform, not all available options
✓ Patient expectations affect satisfaction - Understanding realistic outcomes before surgery is critical for satisfaction
Every day, millions of people across the United States experience back pain. If you're one of them, this comprehensive guide will help you determine whether back surgery is the right choice by explaining the different surgical options, realistic recovery timelines, and the risks and benefits of each procedure based on the latest research.
Most people with long-standing back pain have already tried several non-surgical treatments: physical therapy, medications, injections, chiropractic care, and more. If these approaches haven’t provided relief and you’re still living in pain, it may be time to discuss back surgery with a qualified spine specialist.
Understanding your options is essential. Not all back surgeries are the same, and the procedure you choose can significantly influence your recovery, long-term spinal health, and overall outcome.
Understanding Back Surgery: What It Is and When It's Needed
Back surgery aims to adjust or repair the spine’s anatomy to relieve pain caused by various spinal conditions. Because many different symptoms and underlying issues can lead to back pain, a range of surgical procedures exists. Each designed to address a specific problem based on your individual needs.
The Goal of Back Surgery
The fundamental goals of any back surgery should be to:
Eliminate or significantly reduce pain by addressing the structural source of discomfort.
Restore function and mobility, allowing you to return to normal daily activities.
Preserve as much natural anatomy as possible to protect your spine’s long-term health.
Prevent further deterioration by correcting the underlying problem.
Traditional surgical approaches often focus solely on pain relief. Typically by stopping spinal motion through fusion. However, modern motion-preserving techniques can address all four goals at the same time.
What Causes Back Pain Requiring Surgery?
Back pain severe enough to warrant surgical consideration usually stems from specific structural problems, including:
Herniated or bulging discs: When the soft inner disc material pushes through small tears in the outer layer, causing inflammation and nerve compression.
Degenerative disc disease: Age-related disc breakdown that leads to height loss, instability, and chronic pain.
Spinal stenosis: Narrowing of the spinal canal that compresses the spinal cord or nerve roots.
Spondylolisthesis: A condition in which one vertebra slips forward over the one below it.
Facet joint arthritis: Degeneration of the small joints that connect the vertebrae.
Annular tears: Tears in the outer layer of a disc that trigger chronic inflammation and pain.
Bone spurs: Bony overgrowths that can irritate or compress nearby nerves.
It’s essential to speak with your doctor about the exact symptoms and pain you’re experiencing. This allows them to identify the underlying cause and guide you toward the appropriate treatment. An accurate diagnosis is the foundation of successful care.
When Should I Consider Back Surgery?
Back surgery is a reasonable option for individuals who have experienced persistent pain for several months or longer and have not found relief despite trying comprehensive non-surgical treatments.
Evidence-Based Criteria for Surgical Consideration
Recent research has clarified when surgery becomes appropriate:
Conservative treatment has been exhausted: A 2025 systematic review found that appropriate conservative care should include at least 6-12 weeks of physical therapy, medications, and activity modifications.1 If comprehensive conservative treatment fails, surgical evaluation is warranted.
Progressive neurological deficits: If you're developing increasing weakness, numbness, or loss of function, surgery should be considered sooner to prevent permanent nerve damage. A 2024 German study found that longer symptom duration correlates with worse surgical outcomes and lower chances of neurologic recovery.2
Severe impact on quality of life: When pain prevents you from working, sleeping, or performing basic daily activities despite appropriate conservative care.
Structural problems confirmed on imaging: MRI or CT scans show clear structural abnormalities that correlate with your clinical symptoms.
Emergency symptoms: Cauda equina syndrome (sudden loss of bowel or bladder control) requires immediate surgical intervention.

Important Timing Considerations
A 2024 study examining predictors of poor outcomes after microdiscectomy found that patients with longer symptom duration before surgery had significantly worse outcomes.3 This doesn't mean you should rush into surgery, but it does mean that once conservative care has clearly failed, unnecessarily delaying appropriate surgery can lead to worse results.
Free Expert MRI Review
If you’re unsure whether back surgery is the right option for you, the Deuk Spine Institute offers a Free MRI Review to help determine your eligibility for treatment. Dr. Ara Deukmedjian personally reviews your imaging and provides an honest, expert assessment of all available treatment options.
Understanding the Benefits and Risks of Back Surgery
Before deciding whether back surgery is right for you, it’s essential to understand the potential benefits and risks of each procedure. These can vary significantly depending on the specific type of surgery performed.
Potential Benefits of Back Surgery
When performed appropriately on the right candidates:
Pain elimination or significant reduction allowing you to return to a pain-free or manageable quality of life
Increased range of motion giving you freedom to do the physical activities you enjoy (particularly with motion-preserving procedures)
Reduced medication dependence eliminating or minimizing the need for pain medications, particularly opioids
Prevention of further deterioration addressing structural problems before they cause permanent damage
Neurological recovery reversing or preventing progression of weakness, numbness, or other nerve-related symptoms
Improved quality of life enabling return to work, hobbies, exercise, and normal daily activities
General Risks of Back Surgery
All surgical procedures carry some level of risk. General risks include:
Infection: Surgical site infections can range from superficial to deep, sometimes requiring additional procedures
Bleeding: Excessive blood loss during or after surgery
Blood clots: Deep vein thrombosis or pulmonary embolism
Anesthesia reactions: Adverse responses to anesthesia medications
Nerve damage: Injury to spinal nerves or nerve roots
Cardiovascular events: Heart attack or stroke (rare but possible, especially in high-risk patients)
Failed surgery: The procedure doesn't achieve the intended pain relief
Need for additional procedures: Complications or incomplete relief requiring revision surgery
However, risk levels vary dramatically depending on the type of surgery performed. Traditional open surgeries with fusion carry significantly higher complication rates than truly minimally invasive procedures like Deuk Laser Disc Repair®.
7 Types of Back Surgeries: Comprehensive Comparison
Understanding your surgical options empowers you to make informed decisions. Let's examine each type of back surgery, from the most advanced to traditional approaches.
1. Deuk Laser Disc Repair: The Gold Standard in Motion-Preserving Surgery
What It Is?
Deuk Laser Disc Repair® (DLDR) is a revolutionary minimally invasive procedure where the surgeon uses an endoscope (a narrow tube with a high-definition camera) to reach the source of back pain without removing stabilizing joints, bones, or ligaments. The procedure is peer-reviewed and published as a safe and effective treatment for back pain from annular tears, herniated discs, bulging discs, degenerated discs, and spinal stenosis.
Using a thin endoscope to visualize the damaged disc, the surgeon uses a precision Holmium: YAG laser to remove only the damaged disc tissue causing pain. This damaged tissue represents only 5-10% of the total disc. The precision laser does not damage surrounding bone and tissues, preserving the healthy disc structure.
By leaving healthy disc tissue in place, spinal implants like artificial discs, screws, rods, cages, and fusion are not necessary. Patients are up walking within minutes after surgery. No hospital stay is needed for this outpatient procedure.
The Science Behind DLDR
The laser energy precisely vaporizes the herniated disc material and cleans the annular tear, eliminating the inflammation that causes pain. This advanced technique gently separates tissues at a microscopic level, avoiding the trauma commonly caused by traditional spine surgery. It uses the safest possible approach to the spine every time. Avoiding the complications associated with open surgeries and procedures that require accessing the spine through the abdomen.
What DLDR Can Treat:
- Bulging discs
- Herniated discs
- Sciatica
- Spinal stenosis
- Pinched nerves
- Annular tears (a primary source of discogenic pain)
- Degenerative disc disease
- Chronic back and neck pain
This procedure requires no hospital stay, no narcotic painkillers, and no opioids. After treatment, patients walk out of the facility with a quarter-inch incision covered only by a band aid.
Proven Success Record
Deuk Spine Institute has a 99.6% success rate in eliminating pain with zero complications in over 2,000 procedures performed over 20 years. The procedure even includes a surgical warranty for patients choosing this option.
Dr. Ara Deukmedjian developed this laser technology by traveling the world and studying emerging surgical technologies and techniques. He incorporated various best practices to develop an innovative and unique method using laser technology to heal the spine, avoiding any fusions, drilling, implants, or unnecessary pain.
Recovery Time
This precision laser procedure is uniquely recognized for its gentle, minimally invasive approach. The method explicitly avoids drilling, implanting, or fusing, leaving patients pain-free and able to walk out of the recovery room within an hour.
With just a 4-millimeter incision and no internal damage or scarring, the wound heals within days. Within 2 days, patients report going about their everyday life pain-free and typically return to work within the week.
Patient testimonials state:
"I walked out of the facility with my wife. Walked. That surprised me."
"Had the surgery, and within a week, I can put my socks on and clip my toenails. I’m getting my 30s back."
Post-operative care:
- Patients may use hot/cold packs if needed during recovery
- Advised not to lift anything over 20 pounds for the first 2 weeks
- Contact the facility if any redness, swelling, or unusual pain occurs
Benefits of Deuk Laser Disc Repair
Truly minimally invasive: The precision laser technology creates a 4-millimeter incision, focusing only on problematic tissue while gently moving healthy tissue aside.
Avoids collateral damage: The technology purposely avoids damaging nerves, creating internal scarring, or causing infection.
Rapid recovery: Unlike fusion or implant surgeries, laser spine surgery allows patients to walk out within one hour. Many patients return to everyday life pain-free within one week.
Exceptional safety record: 99.6% success rate with zero complications across thousands of procedures. The minimal, non-invasive approach virtually eliminates the possibility of complications.
No scarring: A 4-millimeter incision leaves no visible scarring and can be covered with a bandaid.
Posterior approach: Accesses the spine through the back, avoiding abdominal organs and reducing infection risk.
Motion preservation: Unlike fusion, your spine maintains natural flexibility permanently.
No hardware: No metal implants mean no hardware complications, no metal detectors triggered, and no need for hardware removal surgery.
2. Spinal Fusion Surgery: Understanding the Traditional Approach
What It Is?
During spinal fusion surgery, the surgeon permanently connects two or more vertebrae (the bones that make up the spine) together. When fused, these vertebrae heal into a single solid bone. This surgical technique mimics the natural healing process of broken bones.
The spine consists of a disc space in front and paired facet joints behind. Whenever you move your spine, these structures allow motion. During fusion, vertebral segments are joined using a bone graft to stop motion at one or more vertebrae. The bone graft is placed between vertebrae and grows to join the segments together.
Bone grafts are taken from the patient's hip during surgery, harvested from cadaver bone, or manufactured. Unfortunately, bone grafts are common causes of unwanted spinal surgery complications.
Metal plates, rods, or screws are used to ensure correct bone graft growth and healing. The fusion process typically takes 3-6 months as the bone graft grows to form one solid bone.

Different Types of Spinal Fusion
Anterior Cervical Discectomy and Fusion (ACDF): A neck surgery where the surgeon approaches the spine through the front of the neck, removes the damaged disc, and fuses vertebrae with a metal plate.
Posterior Cervical Discectomy and Fusion (PCDF): Identical to ACDF but accesses the spine through the back of the neck using screws and rods.
Transforaminal Lumbar Interbody Fusion (TLIF): A lumbar fusion through the back of the spine where an interbody spacer and bone graft are inserted into the disc space.
Extreme Lateral Interbody Fusion (XLIF): Accesses the lumbar spine from the patient's side. Often recommended for lumbar disorders like scoliosis and spondylolisthesis.
Anterior Lumbar Interbody Fusion (ALIF): Uses an anterior (abdominal) approach to fuse lumbar vertebrae. Often used when multiple vertebrae are being fused. This surgery has been reported to carry the highest risk of complications among lumbar fusion techniques.
Recent Research on Fusion Outcomes
A comprehensive 2025 systematic review found that adjacent segment degeneration occurs in 36% of patients and symptomatic adjacent segment disease requiring treatment occurs in 11% within 2-7 years post-operation.4
A 2025 ten-year study found that while 80-85% of patients felt improved in the first two years, this declined to only 68% still feeling improved at 10 years.5
Recovery Time
The recovery timeline for spinal fusion is extensive:
Bone fusion timeline: 3-6 months for the bone graft to solidify
Hospital stay: At Deuk Spine Institute, fusions are performed outpatient when possible. At other facilities, patients typically stay 2-4 days.
Activity restrictions: The first 1-3 months are critical for fusion establishment
Physical therapy: Usually begins after about one month
Return to driving: Approximately 4 weeks if off opioid medications
Return to work: 6 weeks for sedentary jobs, longer for physical occupations
Full recovery: 6-12 months before resuming all normal activities
Continued healing: Bone continues solidifying throughout the first year

Benefits of Spinal Fusion Surgery
Stability for fractures: Fusion adds stability by creating one stronger bone, allowing early mobilization
Restores alignment: Reduces post-decompressive deformity and restores proper spinal alignment
Eliminates painful motion: Relieves pain by eliminating movement at painful joints
Note: Spinal fusion is NOT a decompressive surgery. Laminectomy may need to be performed separately if nerves are compressed.
Risks of Spinal Fusion Surgery
Fusion failure: The bone graft may not properly fuse vertebrae together, leaving the spine unstable
Adjacent segment disease: Fusion transfers stress to nearby levels, causing accelerated degeneration (affects 11-36% of patients)
Need for additional surgery: Failed fusion or adjacent segment problems may require revision
Infection, bleeding, blood clots: Serious risks inherent to invasive surgery
Nerve or blood vessel injury: Damage can occur while placing bone graft or metal implants
Bone graft site pain: Pain where bone is harvested from the hip
Hardware complications: Screws can become loose and erode surrounding bones or soft tissues
Extensive scar tissue: All spinal fusions create substantial scar tissue and destroy normal tissues
Permanent motion loss: Fused segments never move again
Cost: $60,000 to $500,000
3. Laminectomy and Laminotomy: Decompression Surgery
What It Is?
During a laminectomy or laminotomy, the surgeon makes an incision in the back to access the affected vertebrae. This procedure is sometimes referred to as “open decompression”. It focuses on the lamina, the part of the vertebra that forms the protective arch over the spinal canal.
Laminectomy: The lamina is completely removed from a portion of the spine.
Laminotomy: Only part of the lamina is removed.
After gaining access to the vertebra, the surgeon removes the lamina, associated ligaments, and any bone spurs or fragments that may be compressing the nerves. Unfortunately, while laminectomy and laminotomy can relieve nerve compression, they do not treat back or neck pain and often worsen mechanical back pain because they do not correct the underlying disc damage.
These procedures create more space for the spinal cord and nerves, reducing compression, but they fail to address the structural disc issues that are typically responsible for pain. The surgery generally takes 2–3 hours.
Common Combination with Fusion
During laminectomy, it's common to perform spinal fusion due to the instability the bone removal causes. A bone graft is placed between vertebral discs to fuse them together. Laminotomy is always performed as part of lumbar microdiscectomy to decompress nerves.
Recovery Time
Hospital stay: 2-4 days to monitor for complications
Initial recovery: Powerful pain medications and stool softeners typically prescribed
First month: Restrict intense exercise while maintaining some movement
Physical therapy: Assists recovery, which can take months or years
Return to driving: Approximately 2 months if not taking opioids
Full recovery: 2-6 months depending on patient health and procedure complexity
Permanent stiffness: Most patients experience some degree of lasting stiffness
Benefits of Laminectomy/Laminotomy
Pressure relief: Reduces or eliminates leg or arm pain from nerve compression
Increased mobility: More room for spinal cord and nerves reduces pain, allowing better movement
Reduced radiating symptoms: Eliminates numbness, tingling, and prickling sensations
Note: Back pain typically worsens permanently after these procedures.
Risks of Laminectomy/Laminotomy
Collateral tissue damage: Invasive procedure may damage surrounding tissues and nerves
Persistent pain: Unsuccessful procedure may result in continued or worsened back pain
Cerebrospinal fluid leak: Tear of the dura mater membrane can occur
Infection and bleeding: Risk of excessive bleeding requiring transfusion
Severe postoperative pain: All laminectomies result in significant pain necessitating prolonged opioid use
Spinal instability: Bone removal weakens spinal structure
Cost: $50,000 to $150,000
4. Discectomy Surgery: Removing Herniated Disc Material
What It Is?
A discectomy aims to remove the herniated part of a damaged disc, easing pressure on nerves. The surgeon accesses the spine through the back using various tools to cut through tissues surrounding the vertebra and remove herniated disc material.
A discectomy is commonly performed on the lumbar spine and relieves leg pain from herniated discs. This procedure does not help back pain and frequently makes it permanently worse.
"Discectomy" means "cutting out the disc." Patients can have one disc (single-level) or multiple discs (multi-level) removed. A traditional discectomy uses an "open" technique with a larger incision to see the spine directly. Thereby, making it a highlyinvasive spine surgery.
Recovery Time
Hospital stay: Usually required for several days following procedure
Immediate relief: Leg pain should cease immediately post-surgery
Initial discomfort: Soreness from incision and spinal nerve irritation
Return to desk work: 3-4 weeks
Return to heavy lifting jobs: 8-12 weeks
Physical therapy: May be prescribed to regain full spinal movement
Benefits of Discectomy Surgery
Pain relief: Treats numbness, weakness, and tingling in legs from herniated discs
Removes problem tissue: Reduces chances of recurrence by removing herniated material
Risks of Discectomy Surgery
Nerve damage: Tools and incisions can damage neighboring nerves
Persistent pain: If herniation not properly removed
Cerebrospinal fluid leak: Can damage nerves
Bleeding, infection, blood clots: Standard surgical risks
Worsening back pain: Common outcome as spine becomes less stable
Spinal instability: From removal of bone, facet joints, and ligaments
Muscle damage: Cutting through back muscles creates lasting weakness
5. Microdiscectomy Surgery: A "Minimally Invasive" Approach
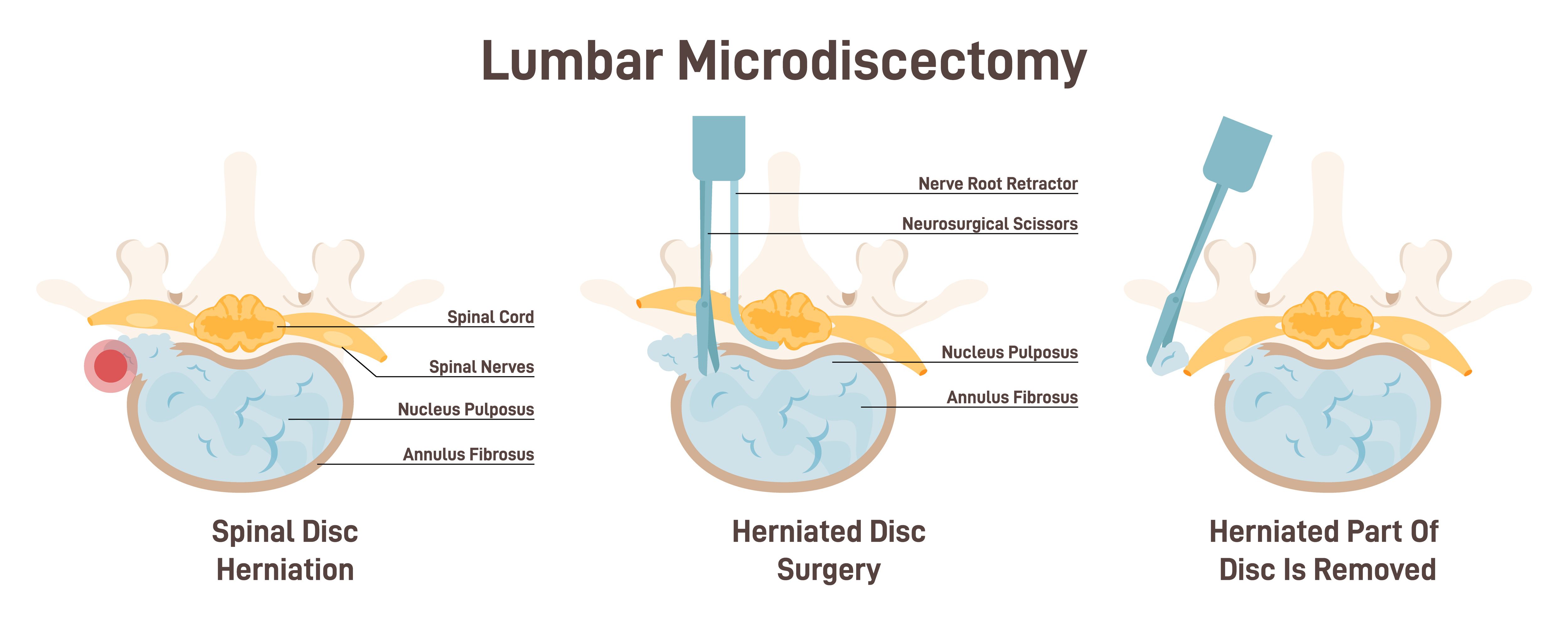
What It Is?
A microdiscectomy is similar to a standard discectomy but uses a smaller skin incision (1-2 inches) and a microscope for magnification. It's usually recommended for sciatica caused by spinal nerve compression.
The surgeon makes a 1-2 inch incision on the back above the herniated disc location. After cutting muscle away from the spine, the surgeon removes bone and ligaments to access the herniated disc material. Unfortunately, part of a spinal facet joint must also be removed, leading to significant spinal instability. This instability magnifies back pain and often requires a second procedure such as fusion.
Once herniated disc material is removed, pressure on surrounding nerves is relieved and leg pain should cease.
Recent Research on Microdiscectomy Outcomes
A critical 2024 study found that 25-33% of microdiscectomy patients report poor surgical outcomes despite technically successful procedures.
- The study identified several predictors of poor outcomes:
- Longer symptom duration before surgery
- Primarily axial back pain rather than radicular leg pain
- High BMI
- Interestingly, preoperative physical therapy was associated with worse outcomes, suggesting patients destined for surgery may benefit from earlier intervention
Recovery Time
Hospital stay: Usually outpatient (same-day discharge)
Immediate leg pain relief: Should occur post-surgery
Initial discomfort: Soreness from incision site
Activity restrictions: First 1-2 weeks avoid driving, prolonged sitting, heavy lifting
Physical therapy: May be prescribed to regain full movement
Full recovery: 6 weeks to 3 months for most patients
Benefits of Microdiscectomy
Immediate leg pain relief: Once nerve pressure is removed
Small incision: 1-2 inches, less than open discectomy
Limited tissue disruption: Smaller incision means less surrounding damage
Quick return to mobility: Patients often walk out same day
Risks of Microdiscectomy
Recurrent herniation: Surgery doesn't prevent future herniations (5-15% recurrence rate)
Cerebrospinal fluid leak: Can damage nerves
Nerve damage: Tools and incisions can injure spinal nerves
Bleeding, infection, blood clots: Standard surgical risks
Worsening back pain: Common outcome due to spinal instability
Spinal instability: Frequent consequence from removing bone, joints, and stabilizing ligaments
Poor outcomes: 25-33% of patients report unsatisfactory results
6. Sacroiliac Joint (SI Joint) Fusion
What It Is?
The sacroiliac joint links the iliac (pelvic) bones to the sacrum (lowest part of spine above tailbone). This joint absorbs shock, protecting the spine from impact forces. When injured or deteriorated, it causes pain in buttocks, low back, and legs.
Important note: The SI joint is an uncommon but significant cause of pelvic and lower back pain. Prior to surgery, injections and therapy should be tried, as they result in pain resolution 90% of the time when done properly.
During SI joint surgery, the patient lies face down while the surgeon makes a small incision on the side of the buttocks. A bone graft is placed between the ilium and sacrum with the intention of connecting the two bones, relieving joint pain.
The bone graft (usually taken from hip bone) doesn't automatically fuse bones. Over time, it grows to create one immobile joint. The bone graft continues solidifying for up to 12 months, though patients feel immediate relief.
Recovery Time
Hospital stay: Same or next day discharge
Post-procedure pain: Some pain from incision or graft site; ice and medication recommended
Immediate mobility: Walking within hours, usually with cane or walker assistance
Full walking: Within one month
Physical therapy: Begins one month post-surgery to ensure proper fusion
Activity restrictions: Avoid heavy lifting or strenuous activity for 3-4 months
Full recovery: 6 months to return to normal life
Benefits of SI Joint Fusion
Stabilizes the joint: Reduces pain and increases stability
Minimally invasive: Patients walk within hours with lowest infection risk
Short operating time: Minimal tissue displacement results in easier, quicker recovery
Risks of SI Joint Fusion
Fusion failure: Bone graft may not properly connect the joint
Adjacent segment disease: Pressure transfers to other pelvic areas
Bleeding, infection, blood clots: Standard surgical risks
Pelvic fractures: Possible complication
7. Artificial Disc Replacement
What It Is?
Recommended for patients suffering from recurring back pain for 6+ months who find no relief in non-surgical procedures. During artificial disc surgery, the surgeon removes the pain-causing disc and replaces it with an artificial replacement.
Over time, discs can become damaged or deteriorate, causing back pain. When discs can no longer support vertebrae, artificial disc placement may be recommended.
The surgeon reaches the spine through the anterior (front) of the patient through the abdomen, moving organs aside. This is generally regarded as the most risky and dangerous approach to the spine due to severe complications known to occur. Once at the spine, they remove the damaged disc and replace it with an artificial disc designed to mimic natural movement.
Recovery Time
Hospital stay: 2-3 days before returning home
Immediate mobility: Walking within 24 hours of surgery
Full mobility: No new bone needs to heal, so full mid-section mobility possible
Return to work: After first 6 weeks
Activity restrictions: Avoid movements causing back hyperextension
Physical therapy: Typically prescribed
Benefits of Artificial Disc
Pain relief: Removes problematic disc causing pain between vertebrae
Improved range of motion: Each vertebra maintains independent movement freedom
Reduced pressure: Relieves stress on adjacent discs
Risks of Artificial Disc
Dislocation: Artificial disc may become dislodged between vertebrae
Infection: Can occur in days following placement
Implant loosening: Weakening wear over time may require additional procedures
Bleeding, infection, blood clots: Standard surgical risks
Blood vessel injury: Large blood vessels can be damaged, potentially requiring leg amputation
Bowel injuries: May require bowel surgery; scar tissue can cause life-threatening blockages
Paradoxical fusion: Many artificial disc surgeries cause fusion of spinal bones due to severe implantation trauma
Important Considerations for Anesthesia During Surgery
It's essential to consider all factors when receiving anesthesia during surgery. Discuss these questions with your anesthesiologist:
Medical History:
- Do you have high blood pressure?
- Do you have a history of complications with anesthesia medications (Propofol, Fentanyl, Tramadol)?
- Are you on blood thinners (including natural ones like turmeric, fish oil, ginkgo biloba)?
Current Medications:
- Are you taking any supplements?
- What prescription medications are you currently taking?
Sleep and Breathing:
- Do you have sleep apnea or use a CPAP machine?
- Do you have any breathing problems?
Family History:
- What is your family history of malignant hyperthermia (a rare but serious reaction to anesthesia)?
Always consult with your doctor and anesthesiologist before undergoing any type of anesthesia. At Deuk Spine Institute, you'll find experts invested in you, answering all questions you may have.
Managing Pain During Recovery
Pain associated with back surgery may be a significant concern during your recovery. You may know others who complained about severe pain after their surgery.
This doesn't mean you'll have pain after your surgery.
The success of your surgery and any discomfort you feel afterward depends largely on:
The type of back surgery performed: Minimally invasive procedures cause dramatically less trauma and pain than traditional open surgeries
The surgeon's skill and technique: Experienced surgeons cause less collateral damage
The level of post-operative care: Comprehensive pain management protocols and proper follow-up
Your overall health: Pre-existing conditions affect recovery
Pain Management at Deuk Spine Institute
Deuk Spine Institute is a premier concierge spine surgery clinic and outpatient surgical center specializing in minimally invasive surgical techniques and comprehensive spine treatments designed to cure back and neck pain.
After receiving surgery at Deuk Spine Institute, patients are up and walking within one hour.
The key difference is that truly minimally invasive procedures like Deuk Laser Disc Repair cause minimal tissue trauma, eliminating the severe postoperative pain associated with traditional fusion, laminectomy, or open discectomy.
Frequently Asked Questions
Q: How do I know if I really need back surgery or if I should try more conservative treatment?
A: Surgery should be considered when comprehensive conservative treatment has been exhausted (typically 6-12 weeks of appropriate care including physical therapy, medications, and activity modifications) without adequate improvement, you're developing progressive neurological deficits (increasing weakness or numbness), severe pain significantly impacts your quality of life despite appropriate treatment, or you have emergency symptoms like cauda equina syndrome. However, timing matters. A 2024 study found that longer symptom duration before surgery correlates with worse outcomes. This doesn't mean rush into surgery, but don't unnecessarily delay once conservative care has clearly failed. Get a second opinion from a surgeon experienced in both conservative and surgical management to ensure you're making the right decision for your specific situation.
Q: What's the difference between "minimally invasive" surgery and truly minimally invasive procedures like Deuk Laser Disc Repair?
A: Many procedures marketed as "minimally invasive" still use 1-2 inch incisions, remove significant amounts of bone and tissue, and sometimes include fusion with hardware. True minimally invasive surgery, like Deuk Laser Disc Repair, uses a 4-7mm incision (about the size of a pencil eraser), removes no bone, cuts no muscle, places no hardware, and preserves natural spinal motion. The difference in recovery is dramatic: traditional "minimally invasive" fusion still requires months of recovery, while Deuk Laser Disc Repair allows patients to walk out within an hour and return to normal activities within days. When evaluating "minimally invasive" claims, ask specific questions about incision size, whether bone is removed, whether fusion is performed, and whether hardware is used. The answers will reveal how truly minimally invasive the procedure actually is.
Q: Why did my doctor recommend fusion when I've heard there are motion-preserving alternatives?
A: There are several possible reasons your doctor recommended fusion. First, fusion is sometimes genuinely necessary for conditions involving structural instability, high-grade spondylolisthesis, severe deformity, or fractures. Second, many spine surgeons were trained primarily in fusion techniques and may not be familiar with advanced motion-preserving procedures like Deuk Laser Disc Repair®. Endoscopic spine surgery and laser disc repair require specialized training beyond a standard spine fellowship. Third, financial incentives favor fusion because it generates significantly more revenue than minimally invasive alternatives. Fourth, institutional conservatism means large academic centers often continue performing traditional procedures despite evidence supporting newer alternatives. The key is getting a second opinion from a surgeon trained in both fusion and motion-preserving techniques who can objectively assess which approach is best for your specific condition. If your surgeon becomes defensive when you ask about alternatives or discourages second opinions, that's a significant red flag.
Q: How can I tell if a surgeon is really qualified to perform the back surgery they're recommending?
A: Verify several key credentials and markers of expertise. First, confirm board certification in neurosurgery or orthopedic spine surgery through the American Board of Medical Specialties website. Second, search PubMed or Google Scholar for the surgeon's name alongside the procedure they're recommending. Legitimate specialists publish peer-reviewed research on their techniques and outcomes. Third, ask how many of the specific procedure they've performed. Hundreds or thousands of cases indicate true specialization, not just occasional performance. Fourth, request their personal complication rates and patient outcomes data, not just general statistics. Fifth, check if they're affiliated with accredited surgical facilities and reputable medical institutions. Sixth, read patient reviews carefully, looking for patterns in feedback rather than isolated comments. At Deuk Spine Institute, Dr. Deukmedjian has published multiple peer-reviewed studies documenting his laser technique with a 99.6% success rate and zero complications across over 2,000 procedures. This level of documentation and transparency should be the standard, not the exception.