Spinal Cord Stimulator masks pain with electrical signals without treating the source. It requires a laminectomy for placement, leads are prone to migration, and patients become dependent on a device for life. Discover safer, minimally invasive alternatives that treat the root cause of pain.
⚠️ While Deuk Spine Institute can perform Spinal Cord Stimulator implantation, we do not recommend it. This page explains why — learn the risks before consenting to this procedure.
Why Do Some Doctors Recommend Spinal Cord Stimulator?
While there are legitimate medical reasons, financial incentives often influence recommendations for this device-dependent procedure.
Medical Reasons Cited
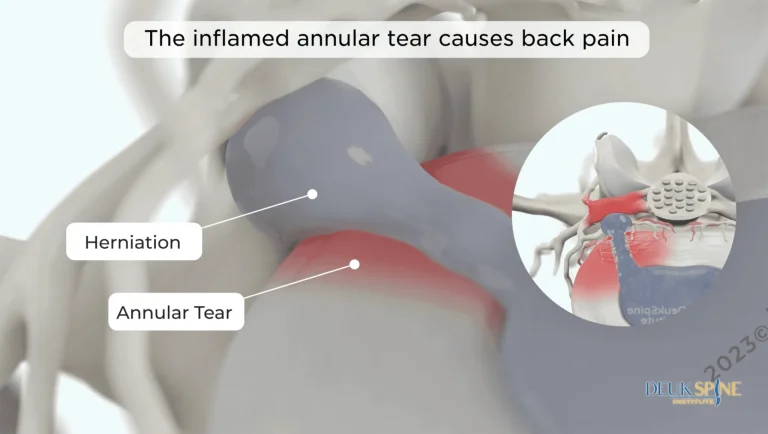
Radiculopathy
Nerve root dysfunction from compressed or pinched nerves. However, SCS masks the pain signal rather than treating the nerve compression itself.
Sciatica
Pain radiating down the leg to the foot from compressed nerves. SCS does not address the herniated disc or nerve compression causing the sciatic pain.
Cauda Equina Syndrome
Poly-radiculopathy from compressed nerves. A rare emergency condition sometimes used to justify SCS for far less severe cases.
Spinal Cord Injury
Pain from compressed or pinched spinal cord. SCS only masks the pain signal without addressing the structural damage causing compression.
Back Pain
General chronic back pain. SCS is often recommended as a last resort, but it never treats the source of pain — only masks it with electrical signals.
Financial Incentives Behind It
Pain Management Doctors Performing Surgery
Pain management doctors are crossing into surgical territory to recommend and perform SCS implantation, often for excessive financial rewards with little benefit to the patient.
High-Paying Procedure ($10K+ Per Surgery)
Among the most profitable procedures per case. Surgeon profits can exceed $10,000 per SCS implantation, creating powerful financial incentive.
Device + Hospital Revenue $50K-$100K+
The expensive implant device, multiple visits for programming and adjustments, trial period, and surgical facility fees drive massive hospital and device manufacturer revenue.
Lifetime Device Dependency
Battery replacements every 5-10 years, lead revisions, reprogramming visits, and device upgrades create a stream of recurring revenue for the lifetime of the patient.
Volume Over Outcomes
Doctors receive the same compensation whether pain resolves or worsens. The system rewards implantation volume, not patient outcomes or pain resolution.
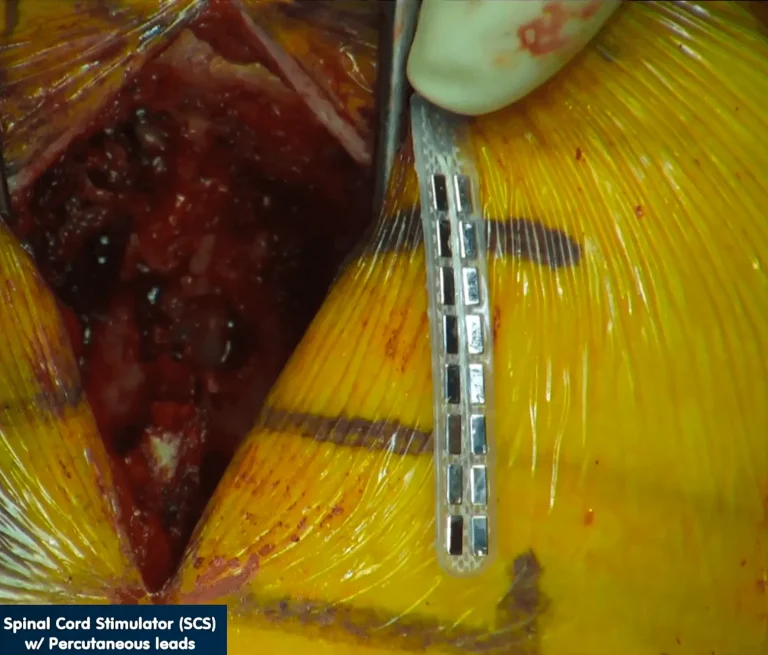
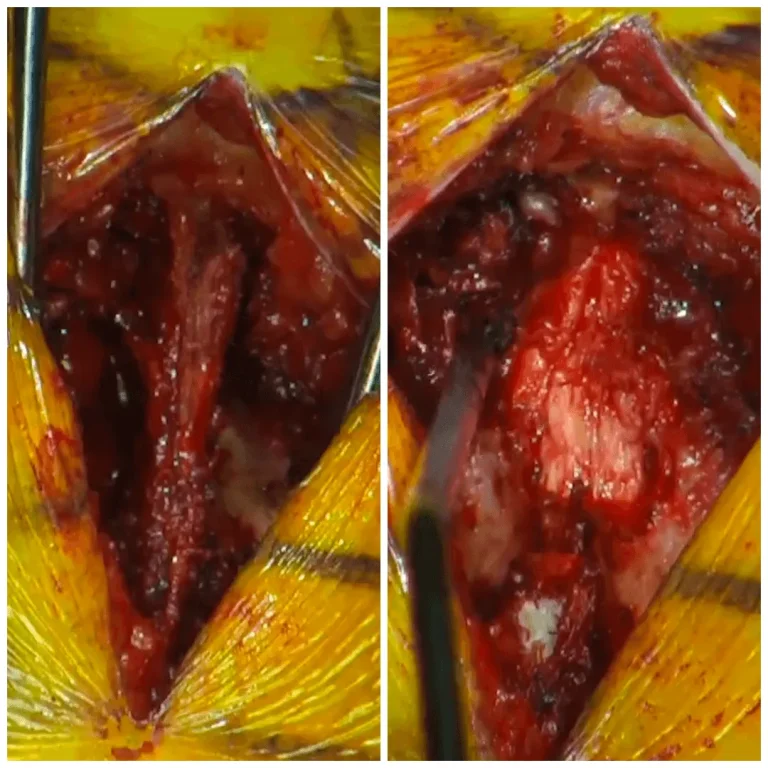
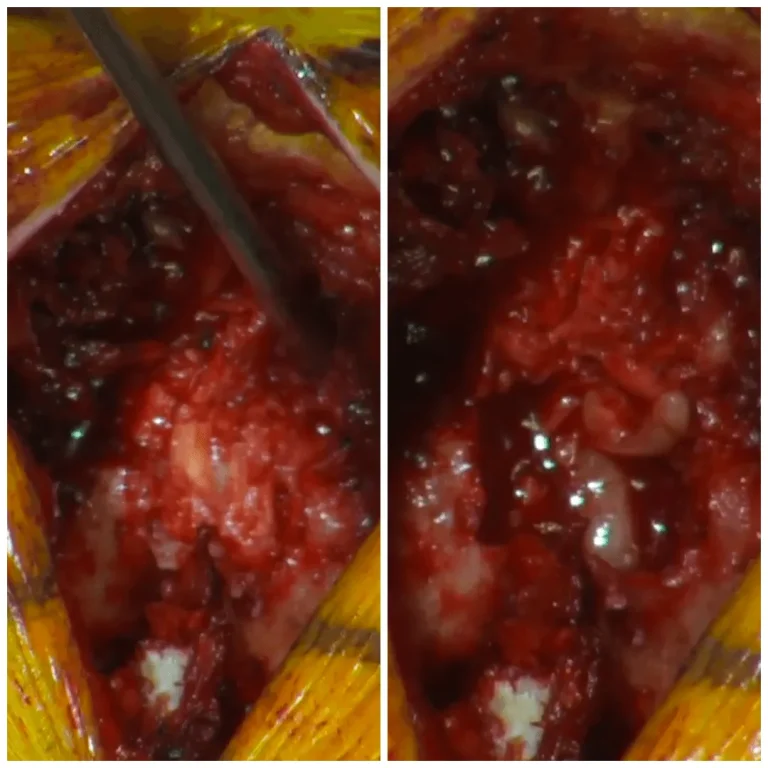
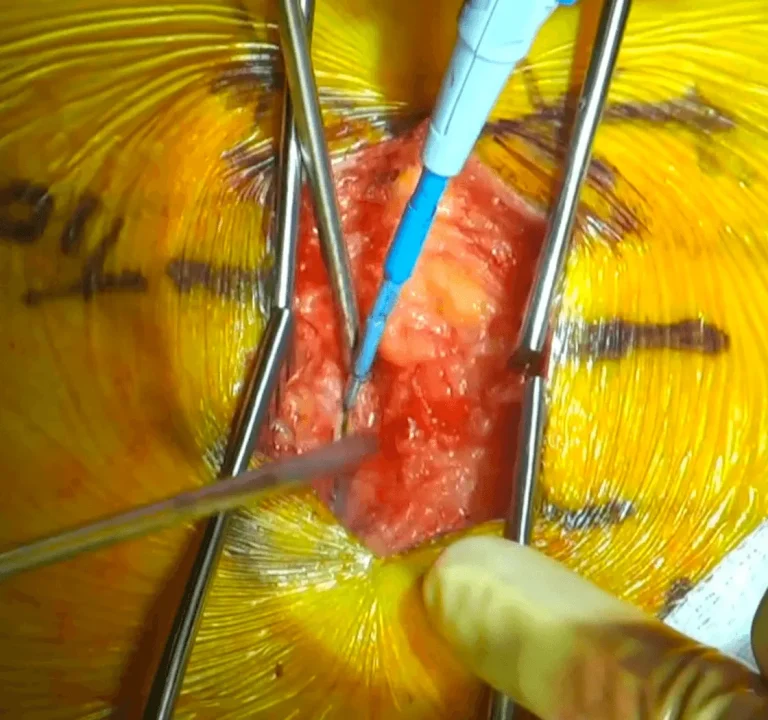
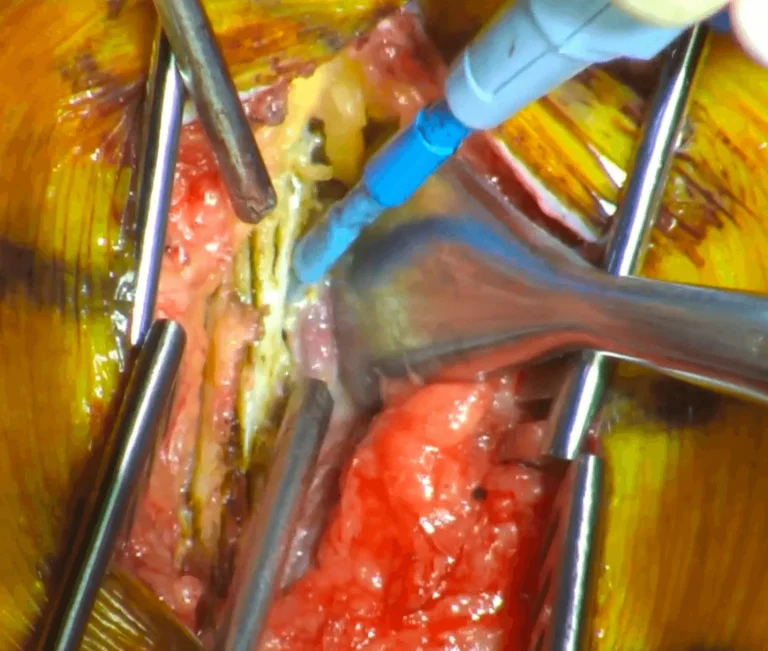
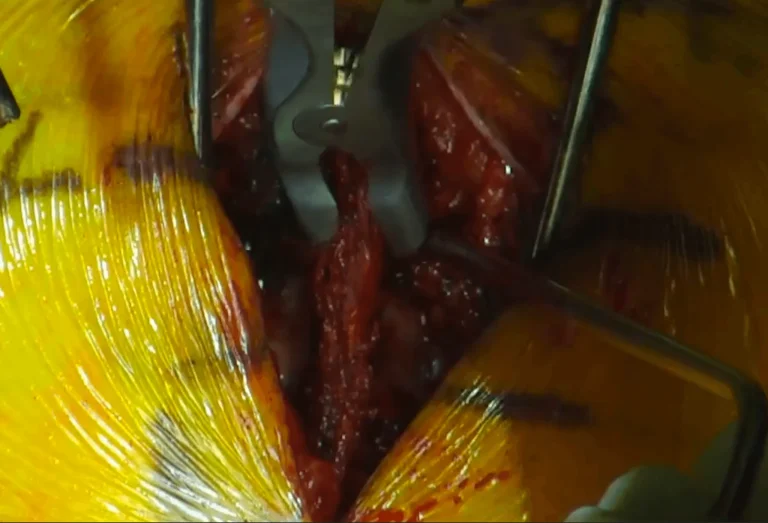
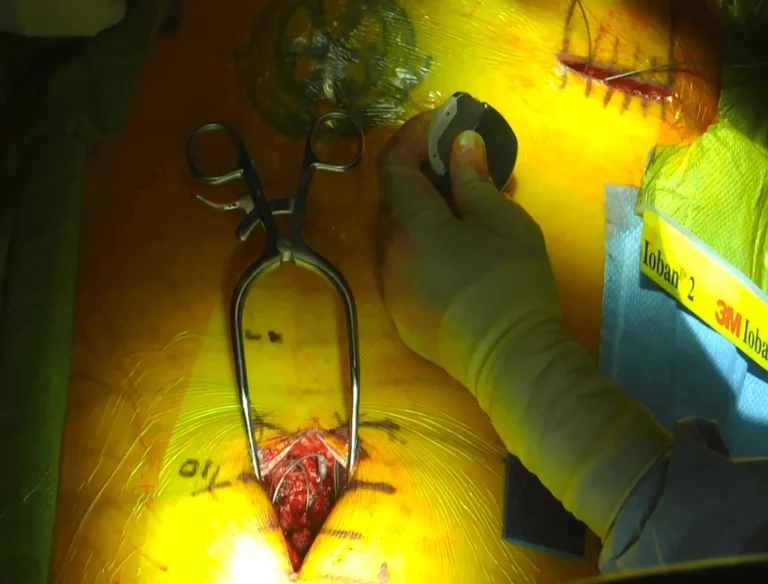
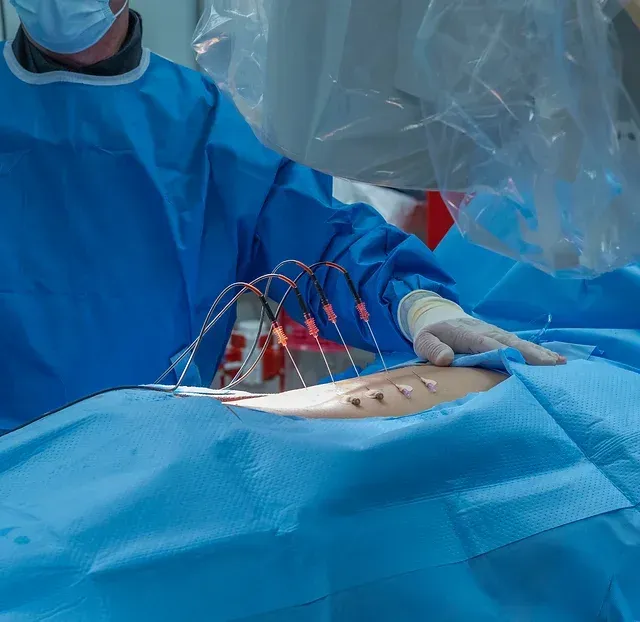
THE SURGICAL PROCESS
How Is Spinal Cord Stimulator Performed?
Graphic Surgical Content
The videos below contain real surgical footage. Viewer discretion is advised.
Permanent nerve or spinal cord damage causing weakness, numbness, or paralysis in extremities.
Spinal Fluid Leak
Dural tears during lead placement leading to cerebrospinal fluid leaks, requiring additional repair surgery.
Infection
Including meningitis, spinal epidural abscess, osteomyelitis, and discitis from implanted hardware.
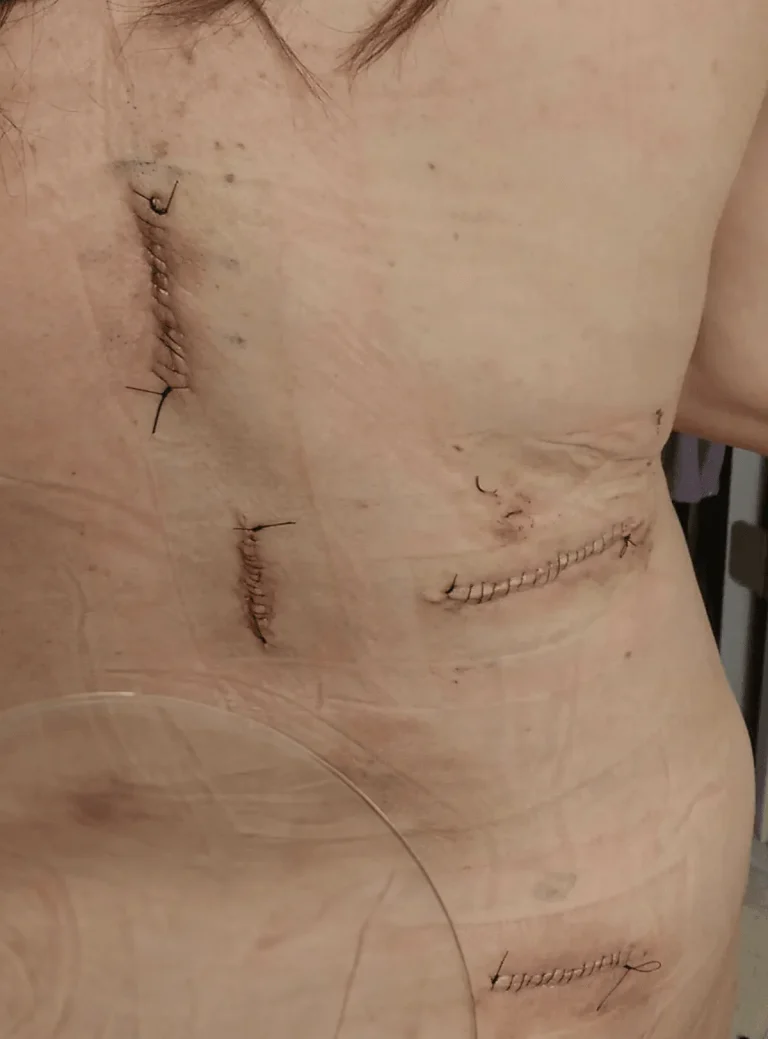
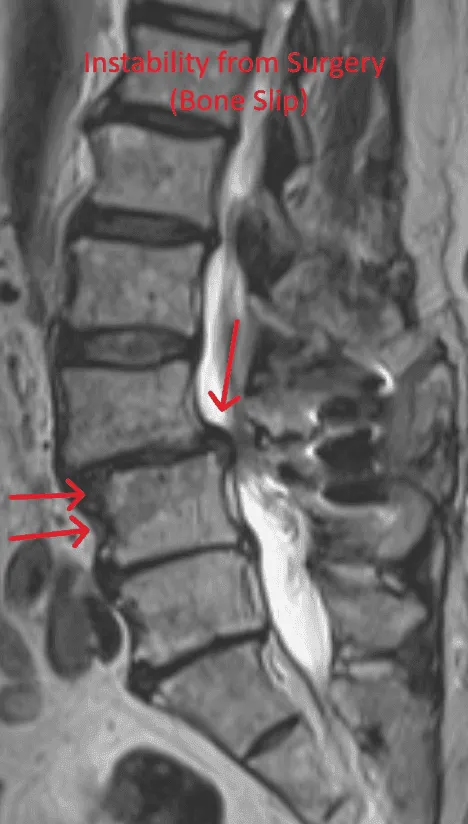
Spinal Instability
Laminectomy during placement removes stabilizing structures, causing instability requiring fusion with screws and rods.
Fractured Vertebrae
Weakened spine from bone removal during placement can lead to vertebral fractures and collapse.
Residual Stenosis
Stenosis persists or reoccurs after SCS placement, requiring additional surgical intervention.
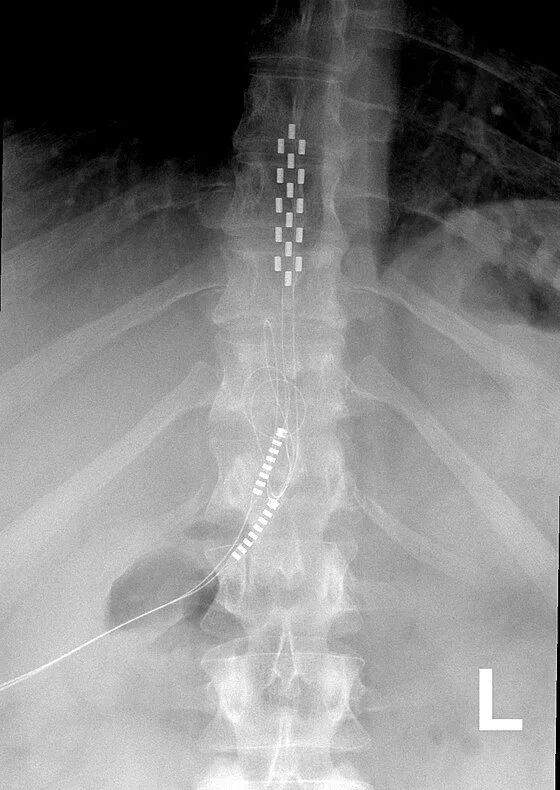
Lead Migration
Implanted leads shift from their original position, causing loss of pain relief and requiring revision surgery.
Scarring Within the Spine
Excessive scar tissue forms around the spinal cord and nerves, causing chronic pain and nerve dysfunction.
Paralysis
Lead placement on the spinal cord carries risk of permanent paralysis from cord damage during surgery.
WHAT WE RECOMMEND INSTEAD
Deuk Laser Disc Repair®: A Safer, Proven Alternative
Instead of masking pain with electrical signals, Deuk Laser Disc Repair® uses endoscopic technology and laser precision to treat the actual source of pain — the damaged disc — through an incision smaller than a fingernail. For piriformis-related pain, Deuk Piriformis Release offers targeted relief, and Deuk Plasma Rhizotomy® addresses facet joint pain without hardware or device dependency.
No Device Dependency
Treats the source of pain directly — no permanent implant, no leads, no generator, no battery replacements for life.
Treats Root Cause
Laser technology directly repairs the damaged disc — the actual source of pain that SCS merely masks with electrical signals.
Same-Day Recovery
Outpatient procedure under light sedation. Walk out the same day — no hospital stay, no intubation, no opioids required.
Proven Results
95% patient satisfaction, 0.01% complication rate, and over 1,300 successful procedures performed by Dr. Deukmedjian.
Feature
Spinal Cord Stimulator
Deuk Laser Disc Repair®
Approach
❌ Masks pain with electrical signals
✅ Treats the source of pain
Procedure
❌ Invasive — requires laminectomy
✅ Minimally invasive, endoscopic
Hardware
❌ Permanent implant (leads + generator)
✅ None
Incision Size
❌ Two large incisions
✅ Less than 1/4 inch
Anesthesia
❌ General (intubated)
✅ Light IV sedation
Hospital Stay
❌ 1-3 days inpatient
✅ Outpatient — go home same day
Recovery Time
❌ 4-8 weeks
✅ Days
Device Dependency
❌ Lifetime — battery replacements required
✅ None
Complication Rate
❌ High — lead migration, paralysis risk
✅ 0.01%
Success Rate
❌ Variable — many end in pain management
✅ 95% patient satisfaction
A BETTER ALTERNATIVE
Deuk Laser Disc Repair®
Minimally invasive, outpatient procedure with a 0.01% complication rate and 95% patient satisfaction. No implants. No device dependency. Same-day recovery.