

Medical disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
If you’ve been diagnosed with spinal stenosis or a herniated disc and your doctor has recommended a laminectomy, you need to understand something critical: While a laminectomy can be effective for relieving leg pain and neurogenic claudication in some patients, recent research reveals troubling limitations when it comes to treating axial back pain, the kind of pain that originates directly in your lower back.1
Understanding What Laminectomy Actually Treats
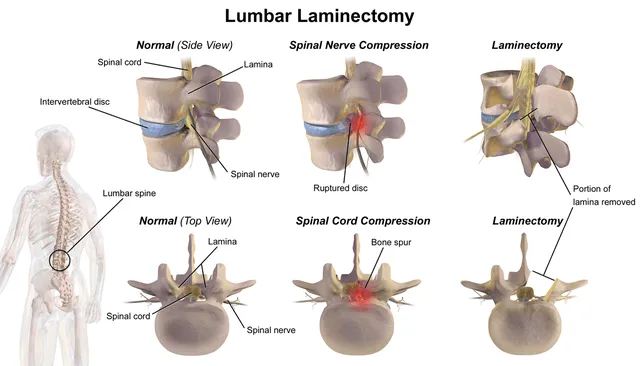
A laminectomy is a decompression surgery where a surgeon removes the lamina, the bony arch covering the spinal canal, to create more space for compressed nerves. The procedure is primarily designed to address nerve compression symptoms like leg pain, numbness, and walking difficulties caused by spinal stenosis. However, it’s important to recognize what a laminectomy doesn’t address: The underlying sources of mechanical back pain itself.
Traditional open laminectomy requires significant muscle disruption, bone removal, and soft tissue trauma. The surgery creates changes in spinal biomechanics that can lead to new problems even when the original nerve compression is successfully treated.
The Research on Laminectomy Back Pain Outcomes
Limited Success Rates
Recent studies paint a sobering picture of laminectomy outcomes. A 2024 study published in Frontiers in Musculoskeletal Disorders found that nearly half of veterans undergoing decompressive laminectomy failed to achieve functional improvement at 12 months post-surgery.2 This high failure rate raises serious questions about patient selection and the procedure’s actual effectiveness for many individuals.
A comprehensive 2015 analysis of 500 laminectomy patients revealed that 14.4% required reoperation within an average of just 3.4 years.3 More concerning, patients who continued experiencing back pain after a laminectomy had a relative risk of reoperation that was 6.14 times higher than those without postoperative back pain. Among patients requiring reoperation, back pain was the most common symptom, affecting 54.17% of these individuals.
The Quality of Evidence Problem
A systematic review examining long-term laminectomy outcomes found only “low-quality evidence” that patients experience significant improvements after surgery.4 After reviewing 12 studies involving 83,492 patients with at least 5 years of follow-up, researchers concluded that the reoperation rate was 14% within 5-10 years. The study emphasized that despite spinal stenosis being a highly prevalent condition, there remains a troubling lack of high-quality evidence supporting the long-term benefits of laminectomy.
Axial Back Pain: The Achilles’ Heel of Laminectomy
One of the most significant limitations of a laminectomy is its inability to effectively treat axial back pain, the deep, achy pain centered in the spinal column itself. Research shows that axial back pain is “not as reliably treated” even with advanced pain management techniques like spinal cord stimulation.5 This is because a laminectomy addresses nerve compression but does nothing to treat the degenerative disc disease, facet joint arthritis, or inflammatory processes that often cause the actual back pain.

The Post-Laminectomy Pain Syndrome Reality
Post-laminectomy syndrome, also known as failed back surgery syndrome (FBSS), affects between 10% to more than 40% of laminectomy patients according to national data.6 For patients undergoing more complex spine surgeries, the failure rate climbs even higher, with 30-46% experiencing continued or new pain after surgery.
Why Laminectomy Fails
Post-laminectomy syndrome develops for numerous reasons:
- Missed pain generators: The most common reason laminectomy fails is that the lesion operated on isn’t actually the source of the patient’s pain. Many patients have multiple spinal issues, and identifying the true pain generator requires expertise and thorough evaluation.
- Epidural fibrosis: Scar tissue formation around nerve roots is a leading cause of persistent pain after a laminectomy. While scarring is a natural part of healing, excessive scar tissue can compress nerves and create new sources of pain.6
- Spinal instability: Removing the lamina and surrounding structures can increase spinal instability, particularly when a laminectomy is performed without fusion. This instability causes ongoing mechanical pain and may accelerate adjacent-segment degeneration.
- Incomplete decompression: Even when surgery addresses the compressed nerve, residual or recurrent disc herniation can cause symptoms to return. Studies show that recurrent disc herniation occurs in 5-10% of patients, most commonly within the first three months after surgery.
- Adjacent segment disease (ASD): The biomechanical stress doesn’t disappear after a laminectomy; it simply shifts to adjacent spinal levels. Over time, these segments may degenerate more rapidly, leading to new stenosis or herniation that requires additional surgery.
Each of these failure mechanisms traces back to the same root problem: laminectomy operates on the wrong anatomy for most back pain patients. The structural reasons why bone removal misses the actual pain source go deeper than the failure rates alone suggest.
The Problem With Treating Mechanical Back Pain
A critical distinction that many patients, and some surgeons, fail to recognize is the difference between radicular pain (leg pain from nerve compression) and axial back pain (pain originating in the spinal structures themselves). Laminectomy was designed to address the former, not the latter.
Research published in StatPearls notes that in cases of low-grade degenerative spondylolisthesis, recent meta-analyses found no increased risk of instability after laminectomy “especially in patients without predominant symptoms of mechanical back pain.7” This phrasing reveals an important truth: Laminectomy is not indicated for mechanical back pain, yet many patients undergo the procedure expecting it to resolve this type of discomfort.
The Hidden Complications
Beyond the core issue of effectiveness, a laminectomy carries significant risks that can worsen a patient’s condition:
- Intraoperative durotomy (tear in the protective membrane around the spinal cord) occurs in 10% of cases
- Postoperative cerebrospinal fluid leaks develop in 1.6% of patients
- Infection, bleeding, and blood clots remain persistent risks
- Permanent nerve damage can occur during surgery
- Muscle atrophy from surgical disruption affects long-term spinal stability
The muscle damage alone deserves special attention. During a traditional laminectomy, surgeons must dissect through and retract the paraspinal muscles. This trauma leads to muscle atrophy, weakness, and chronic inflammation, all of which contribute to ongoing back pain even when nerve decompression is successful. Research suggests that strengthening exercises targeting these damaged muscles may help reverse atrophy, but the damage has already been done.5
What Recent Research Tells Us About Better Approaches
A 2024 network meta-analysis published in BMC Medicine compared various surgical interventions for lumbar spinal stenosis.8 The study found that while minimally invasive techniques like full-endoscopic laminotomy showed some advantages in terms of reduced muscle damage and faster recovery, the fundamental limitation remains: None of these procedures adequately addresses the underlying causes of discogenic back pain.
The research consistently points to a troubling pattern: laminectomy often trades one set of problems for another. While it may relieve nerve compression symptoms in the short term, it fails to address the underlying degenerative processes that cause back pain and may even worsen them.

The Misalignment of Expectations
Gathering information and setting expectations for outcomes can be difficult, especially as we enter the age of artificial intelligence (AI). A doctor or surgical team might provide a diagnosis and treatment aligned with their specialty and experience. Querying generative AI about what is best for you can result in biased results, depending on the questions asked, your history with the model, which version it is, how it weights new information gathered from the web and its training data (which generally has a cutoff point), and more.
Disparate and sometimes unreliable information can lead to patients having unrealistic expectations for outcomes. Misalignment between patient expectations and realistic surgical outcomes can have deleterious effects on the path chosen and long-term recovery. For example, many patients expect to feel decades younger after back surgery, but this is unrealistic. More importantly, if part of your pain stems from a secondary condition that a specific surgery cannot address, such as degenerative disc disease or facet joint arthritis, you may still experience significant pain after a laminectomy even if the surgery is technically successful.
The Data on Revision Surgery
Perhaps most telling is the data on revision surgery rates. The 2015 study of 500 laminectomy patients found that 44.44% of those requiring reoperation needed decompression plus fusion, while 55.56% needed decompression alone.3 The lifetime risk of requiring fusion surgery after an initial laminectomy was 8.0%, indicating that many patients end up needing more extensive and more risky procedures down the road.
A 2022 study examined the incidence of failed back surgery syndrome across different procedure types and clinical settings.9 The highest rates of FBSS occurred in elderly patients (ages 70-74), those receiving procedures in inpatient settings, and those undergoing multi-level surgery, all common characteristics of traditional laminectomy patients.
Understanding Your Pain Source
Before agreeing to a laminectomy, you need a thorough evaluation to determine whether your pain is truly coming from nerve compression or from other sources that a laminectomy cannot address. Critical questions include:
- Is your primary complaint back pain or leg pain?
- Do you have facet joint arthritis or degenerated discs contributing to your symptoms?
- Is there evidence of spinal instability that might worsen after bone removal?
- Have you exhausted conservative treatment options?
- Do you have realistic expectations about what surgery can and cannot achieve?
Research shows that proper patient selection is crucial for preventing failed back surgery syndrome. Yet the rapidly increasing rates of spinal procedures, combined with financial incentives that favor surgery, can lead to procedures being performed on patients who are unlikely to benefit.
Why Traditional Laminectomy Persists Despite Poor Outcomes
Traditional open laminectomy remains one of the most common spine procedures despite accumulating evidence of its limitations. The reasons are complex and troubling. As detailed in discussions of spinal fusion risks, the spine surgery industry is driven by powerful financial incentives that favor invasive procedures, even when less invasive alternatives might better serve patients.10
The device companies, hospitals, and surgeons all benefit financially from traditional open procedures that require longer operating times, more extensive hardware, and higher reimbursement rates. This creates a system in which patient outcomes sometimes take a back seat to economic considerations.
Alternative Approaches: Minimally Invasive Techniques
Given the substantial limitations of traditional laminectomy for treating back pain, patients need to know about alternatives that address the actual source of pain rather than just creating more space for nerves. Procedures that preserve spinal anatomy while treating disc pathology and inflammation offer a fundamentally different approach.
The key difference is specificity: Instead of removing bone and hoping that decompression will somehow resolve pain, advanced minimally invasive techniques can directly treat the herniated disc tissue, annular tears, and inflammatory processes that cause back pain in the first place. These approaches preserve the spine’s stabilizing structures rather than removing them, reducing the risk of long-term complications such as adjacent segment disease.
What You Should Do If a Laminectomy Has Been Recommended
If a surgeon has recommended a laminectomy for your back pain, take these critical steps:
- Get a second opinion: Seek evaluation from a spine specialist who offers a full range of treatment options, not just traditional surgery. Many patients discover they have alternatives they were never told about.
- Question the diagnosis: Ask specifically whether your pain is coming from nerve compression or from disc degeneration, facet arthritis, or other sources that a laminectomy won’t address.
- Understand the evidence: Ask your surgeon about their success rates specifically for patients with your condition. Request data on long-term outcomes, not just short-term symptom relief.
- Consider conservative treatment: Physical therapy, anti-inflammatory medications, and targeted injections should be exhausted before moving to irreversible surgery.
- Explore minimally invasive options: Advanced endoscopic techniques can often achieve decompression while preserving spinal anatomy and reducing complications.
Take Control of Your Spine Health with a Second Opinion
At Deuk Spine Institute, we believe patients deserve better than traditional approaches that often fail to deliver lasting relief. That’s why we recommend starting with a thorough evaluation to accurately identify your pain sources before considering any surgical intervention.
Schedule your free MRI review and consultation to get a second opinion from specialists who can explain all your treatment options, not just traditional surgery. Our team will review your imaging, discuss your symptoms, and help you understand whether you’re truly a candidate for surgery or if less invasive alternatives might better serve your needs.
Don’t let outdated procedures and inadequate evaluation lead you down a path that research shows fails nearly half the time. Get the comprehensive assessment you deserve and make an informed decision about your spine health.
Frequently Asked Questions
-
Does a laminectomy relieve back pain or just leg pain?
Laminectomy is primarily designed to relieve leg pain, numbness, and walking difficulties caused by nerve compression, not axial back pain that originates in the spine itself. Research shows that axial back pain is “not as reliably treated” by laminectomy because the procedure doesn’t address the underlying causes of mechanical back pain, such as degenerative disc disease, facet joint arthritis, or inflammatory processes. Studies indicate that nearly half of patients fail to achieve functional improvement after a laminectomy, with back pain being the most common persistent symptom requiring reoperation.
-
What is post-laminectomy syndrome, and how common is it?
Post-laminectomy syndrome, also called failed back surgery syndrome, occurs when patients continue experiencing pain or develop new pain after laminectomy surgery. Data show this affects between 10% to more than 40% of laminectomy patients. The syndrome develops due to several factors, including incorrect initial diagnosis, epidural fibrosis (scar tissue formation), spinal instability from bone removal, incomplete decompression, and adjacent segment disease. Patients with post-laminectomy syndrome have a relative risk of requiring reoperation that is 6.14 times higher than those without postoperative back pain.
-
What are the alternatives to a laminectomy for treating back pain?
Before considering a laminectomy, patients should exhaust conservative treatments, including physical therapy, anti-inflammatory medications, and targeted injections. For surgical candidates, advanced minimally invasive endoscopic techniques can achieve nerve decompression while preserving spinal anatomy and reducing complications. The most important step is getting a comprehensive evaluation to accurately identify whether your pain stems from nerve compression (which laminectomy addresses) or from disc degeneration, annular tears, or facet arthritis (which laminectomy cannot fix). A second opinion from a spine specialist who offers a full range of treatment options can help you understand all your alternatives.
-
Sources
1: Laminectomy Invasive Spine Surgery For Stenosis
3: https://pmc.ncbi.nlm.nih.gov/articles/PMC4431053/
4: https://pmc.ncbi.nlm.nih.gov/articles/PMC9473837/
5: https://now.aapmr.org/post-laminectomy-pain/
6: https://www.ncbi.nlm.nih.gov/books/NBK539777
7: https://www.ncbi.nlm.nih.gov/books/NBK542274/
8: https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-024-03653-z


