


By Dr. Ara Deukmedjian, MD
Board-Certified Neurosurgeon, Deuk Spine Institute
Medically reviewed on January 15, 2026
Medical disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
A C4-C5 disc bulge is a cervical spine condition that affects thousands of people each year, causing neck pain, shoulder discomfort, and arm weakness that can significantly impact daily life. Located between the fourth and fifth cervical vertebrae in your neck, this disc plays a crucial role in supporting head movement while absorbing shock from daily activities. When the disc protrudes beyond its normal boundaries, it can cause inflammation and press on nearby nerves, leading to symptoms ranging from mild discomfort to debilitating pain.
Understanding your diagnosis is essential for making informed decisions about your care. This comprehensive guide will help you navigate the complexities of C4-C5 disc bulges, from recognizing symptoms to understanding all available treatment options. Whether you’re newly diagnosed or seeking alternatives after unsuccessful treatments, this article emphasizes the importance of patient advocacy, thorough condition assessment, and finding the right approach for your specific situation.
Understanding C4-C5 Anatomy and Function
The cervical spine consists of seven vertebrae, labeled C1 through C7, extending from the base of your skull to your upper back. The C4 and C5 vertebrae sit in the mid-cervical region, forming a critical segment that supports your head while enabling the neck’s remarkable range of motion.
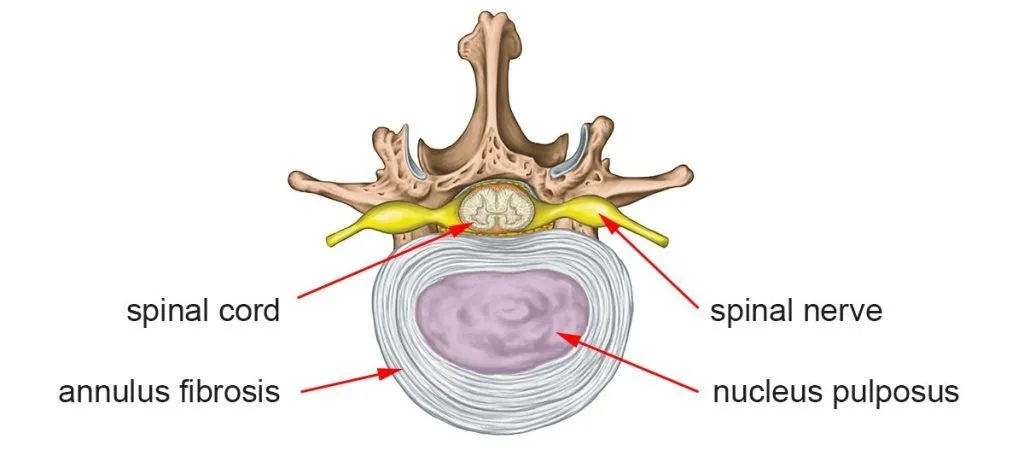
Between C4 and C5 lies an intervertebral disc, a specialized structure that serves multiple functions. This disc acts as a shock absorber during movement, maintains proper spacing between vertebrae to protect nerve roots, allows for smooth neck motion, and distributes mechanical forces evenly across the spine.
Each cervical disc consists of two distinct components working together. The annulus fibrosus is the tough, fibrous outer layer made of collagen fibers arranged in overlapping layers to provide strength and containment. The nucleus pulposus is the soft, gel-like inner core that provides cushioning and distributes compressive forces throughout the disc.1
The C5 Nerve Root Distribution
The C5 nerve root exits the spinal canal between the C4 and C5 vertebrae through an opening called the neural foramen. This nerve root controls specific motor and sensory functions throughout the upper body.
Motor function (C5 myotome) includes the deltoid muscle, which allows shoulder abduction and arm lifting, the biceps muscle for elbow flexion, and the rotator cuff muscles that enable shoulder rotation and stability.
Sensory function (C5 dermatome) provides sensation to the lateral upper arm, the outer shoulder region, and sometimes extends to the thumb side of the forearm.
Understanding this nerve distribution pattern helps explain why a C4-C5 disc bulge produces characteristic symptoms in specific areas of the shoulder and arm. When a bulging disc compresses the C5 nerve root, symptoms follow predictable patterns, allowing accurate diagnosis through careful clinical examination.
What Is a C4-C5 Disc Bulge?
A disc bulge occurs when the outer layer of the intervertebral disc extends beyond its normal boundaries but remains intact. This differs from a disc herniation, where the outer layer tears and the inner material leaks out. Think of it like a tire bulging outward under pressure versus a tire with a puncture.
Types of Disc Pathology
Research has refined our understanding of disc pathology classifications, helping physicians communicate findings and treatment needs more precisely.2
Disc bulge: The entire disc circumference extends beyond the vertebral margins symmetrically. The annulus fibrosus remains intact with no tear. This represents early degenerative changes and may or may not cause symptoms.
Disc protrusion: The nucleus pulposus pushes against a weakened annulus, creating a focal bulge. The base of the protrusion is wider than the displaced portion. The annulus remains unruptured but stretched.
Disc extrusion: The nucleus pulposus breaks through the annulus fibrosus completely. The displaced material remains connected to the parent disc. This typically causes more severe nerve compression.
Disc sequestration: A fragment of disc material completely separates and becomes free-floating. This represents the most severe form of disc displacement. Paradoxically, sequestered fragments may resorb more completely over time as the immune system recognizes them as foreign material.3
Why C4-C5 Develops Problems
While C4-C5 disc bulges are less common than those at C5-C6 or C6-C7, they still affect a significant number of patients. This level experiences considerable mechanical stress during daily activities. The mid-cervical spine serves as a transition zone between the upper and lower cervical regions, making it vulnerable to degenerative changes.
The C4-C5 segment bears substantial weight from the head, estimated at 10-12 pounds in neutral position and increasing to 40-60 pounds with forward head posture. This segment also accommodates significant rotational and flexion-extension movements. The combination of weight-bearing and mobility creates cumulative stress on the disc over time.
C4-C5 Disc Bulge Symptoms
Symptoms from a C4-C5 disc bulge vary significantly depending on the degree of nerve compression, the presence of inflammation, and individual factors. Some people experience dramatic symptoms, while others have minimal discomfort despite significant findings on imaging studies.
Primary Symptoms
Shoulder pain and weakness are the hallmark symptoms of C5 nerve root compression. Many patients describe a deep, aching shoulder pain that doesn’t respond to rest. The deltoid muscle may feel weak, making it difficult to lift the arm away from the body. Tasks like reaching overhead, carrying grocery bags, or lifting children become challenging. Some patients notice their shoulder appears slightly drooped on the affected side due to deltoid weakness.
Neck pain and stiffness often accompany nerve root symptoms. The pain typically localizes to the mid-cervical region but may radiate to the base of the skull or between the shoulder blades. Neck stiffness limits rotation and lateral bending, making activities like checking blind spots while driving uncomfortable or impossible. Many patients report that certain neck positions exacerbate symptoms, particularly extension and rotation.
Arm pain and paresthesias manifest as discomfort radiating from the shoulder down the outer arm, sometimes extending to the thumb side of the forearm. Patients describe sensations of pins and needles, numbness, or tingling in the C5 dermatome distribution. Unlike more distal nerve compressions, such as carpal tunnel syndrome, C5 radiculopathy typically spares the hand while affecting the proximal arm.
Biceps weakness and diminished reflexes can occur with more severe nerve compression. The biceps reflex may be reduced or absent on clinical examination. Patients notice difficulty with activities requiring elbow flexion, such as carrying objects or lifting items to shoulder height. Some describe a sensation of their arm feeling “heavy” or fatigued more quickly than normal.
Less Common Symptoms
Some patients experience symptoms that don’t follow the classic pattern. These can include referred pain to the chest wall or upper back, which may be mistaken for cardiac or pulmonary issues, headaches originating from the mid-neck that radiate forward, and sleep disruption due to difficulty finding comfortable positions.
Other uncommon symptoms include difficulty breathing, difficulty swallowing, and atypical neurological symptoms, like vertigo, nausea, and tinnitus.4,5,6 This highlights an important concept: Imaging findings don’t always correlate with symptoms. You can have a disc bulge visible on MRI without pain, or experience significant discomfort with relatively mild imaging findings.
Understanding Your Symptom Pattern
Recognizing patterns in your symptoms can help guide treatment decisions. Note which movements or positions worsen your symptoms, how long symptoms last during episodes, whether symptoms are constant or intermittent, what activities you’ve had to modify or avoid, and how symptoms affect your sleep quality and daily function.
This information becomes invaluable when discussing treatment options with your healthcare provider. It helps distinguish between disc-related pain, muscle strain, facet joint problems, or other cervical spine conditions that may require different treatment approaches.
Causes and Risk Factors
Understanding why disc bulges develop can help you make informed decisions about prevention and treatment. While some risk factors are beyond your control, others can be modified to reduce your risk of progression or recurrence.
Primary Causes of C4-C5 Disc Bulge
Age-related degeneration is the most common underlying cause. As we age, intervertebral discs naturally lose water content through a process called disc desiccation. This causes discs to become thinner, less flexible, and more prone to bulging under normal stresses. Small tears develop in the annulus fibrosus over time, weakening its structure. Research indicates that disc degeneration typically begins in the third or fourth decade of life and progresses gradually.1
Acute trauma can precipitate disc bulges in previously healthy discs or accelerate degeneration in already compromised discs. Motor vehicle accidents, particularly rear-end collisions causing whiplash, place sudden, extreme forces on the cervical spine. Falls that cause the head to snap backward or forward can create immediate disc injury. High-impact sports activities may generate forces that exceed the disc’s tolerance. A 2025 study emphasized that even when initial X-rays and CT scans appear normal after trauma, MRI may reveal significant disc injury and nerve compression, underscoring the importance of appropriate imaging when symptoms suggest nerve involvement.7
Repetitive stress and poor posture create cumulative damage over time. Forward head posture, increasingly common with smartphone and computer use, dramatically increases forces on cervical discs. Occupations requiring repetitive overhead work place chronic stress on the neck. Prolonged static postures, such as desk work without proper ergonomics, maintain sustained loads on discs. Each of these factors individually may seem minor, but their cumulative effect over months and years can lead to disc bulging and symptoms.
Genetic predisposition plays a role that’s increasingly recognized by researchers. Some individuals inherit a tendency toward earlier disc degeneration. If multiple family members experienced cervical disc problems at relatively young ages, genetic factors may contribute to your susceptibility. While you cannot change your genetic inheritance, awareness of family history can motivate earlier adoption of preventive strategies.
Modifiable Risk Factors
Research identifies several risk factors that you can address to potentially slow progression or reduce symptom severity.
Smoking accelerates disc degeneration through multiple mechanisms. Nicotine reduces blood flow to disc tissues, impairing nutrient delivery and waste removal. Smoking increases inflammatory mediators throughout the body, including in spinal tissues. Chronic coughing from smoking creates repetitive jarring forces on the cervical spine. Studies consistently show that smokers experience more severe disc degeneration and poorer treatment outcomes compared to non-smokers.
Obesity and metabolic factors affect disc health. Excess body weight increases mechanical loads on the cervical spine, even though the neck doesn’t directly bear body weight like the lumbar spine. Obesity is associated with systemic inflammation that may affect disc metabolism. Metabolic syndrome and diabetes can impair tissue healing and regeneration. Maintaining a healthy weight through diet and exercise provides multiple benefits for spine health.
A sedentary lifestyle contributes to disc problems. Prolonged sitting, especially with poor posture, maintains sustained compression on cervical discs. Lack of regular movement reduces nutrient flow to disc tissues, which depend on movement for nutrition. Weak neck and shoulder muscles provide less support for the cervical spine, increasing disc stress. Regular exercise, particularly activities that strengthen the neck and improve posture, can help protect disc health.
Occupational and recreational factors create specific risks. Jobs requiring frequent overhead work stress the cervical spine. Occupations involving heavy lifting without proper technique increase the risk of injury. Contact sports and high-impact activities pose an acute injury risk. Even seemingly benign activities, such as prolonged computer work, can contribute to disc problems when performed with poor ergonomics.

The Importance of Accurate Diagnosis
Getting an accurate diagnosis is the foundation for successful treatment. Yet many patients struggle through months or even years of unsuccessful treatments because their condition wasn’t properly assessed initially. Understanding the diagnostic process empowers you to advocate for the thorough evaluation you deserve.
The Clinical Examination
Your diagnostic journey begins with a comprehensive history and physical examination. An experienced physician should spend adequate time understanding your symptoms, including when they started, how they’ve progressed, what makes them better or worse, how they affect your daily activities and work, what treatments you’ve tried and their effectiveness, and whether you have any other medical conditions that might influence treatment.
The physical examination includes specific tests designed to assess nerve function and identify the pain source. The Spurling test involves the examiner extending and rotating your neck toward the symptomatic side while applying downward pressure. Reproduction of arm pain suggests nerve root compression. However, this test should be performed carefully, as it can temporarily worsen symptoms.
Shoulder abduction relief sign: You place your hand on top of your head. If this position relieves your arm symptoms, it suggests nerve root compression that’s temporarily relieved by opening the neural foramen.
Motor strength testing examines specific muscle groups. For C5 function, the examiner tests deltoid strength by having you abduct your arm against resistance, biceps strength through resisted elbow flexion, and shoulder external rotation strength.
Sensory examination assesses for altered sensation in the C5 dermatome distribution along the lateral upper arm and outer shoulder.
Reflex testing checks the biceps reflex, which may be diminished or absent with C5 nerve root compression.
Imaging Studies: What They Reveal and Their Limitations
While imaging studies provide crucial information, they must be interpreted in the context of your clinical presentation. Not every disc bulge visible on MRI causes symptoms, and occasionally, significant symptoms exist with minimal imaging findings.
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating disc bulges and nerve compression. MRI provides detailed visualization of soft tissues, including discs, nerve roots, spinal cord, and surrounding ligaments. It can reveal the size and location of disc bulges, the degree of neural foramen narrowing, whether nerve roots are compressed, and the presence of spinal cord compression or changes.
Recent research emphasizes that MRI should be obtained when clinical symptoms suggest nerve compression, even if X-rays appear normal.8 This is particularly important after trauma, where disc injury may be the only significant finding requiring treatment.
X-rays cannot visualize disc bulges directly but provide valuable information about vertebral alignment, disc space height, the presence of bone spurs that might contribute to nerve compression, and overall cervical spine curvature. X-rays serve as an important initial screening tool, helping rule out fractures or severe instability.
CT scans offer excellent bony detail and may be useful when MRI is contraindicated, such as with certain metal implants, for evaluating bony foraminal stenosis that contributes to nerve compression, or for surgical planning when precise visualization of bony anatomy is needed.
Electrodiagnostic studies (EMG/NCS) measure the electrical activity of muscles and nerves. These tests can confirm the presence and severity of nerve root compression, identify which specific nerve root is affected, distinguish cervical radiculopathy from peripheral nerve problems, and assess the chronicity and severity of nerve damage. EMG/NCS testing is particularly valuable when clinical findings or imaging studies are ambiguous.
When Findings Don’t Match Symptoms
One of the most challenging aspects of cervical spine diagnosis is the frequent mismatch between imaging findings and symptoms. Studies consistently show that many people without neck or arm pain have disc bulges visible on MRI. Conversely, some individuals with significant symptoms have relatively minor imaging findings.
This reality underscores the importance of comprehensive clinical correlation. Your symptoms, physical examination findings, and imaging studies must all be considered together. A large disc bulge that doesn’t compress nerve roots or cause inflammation may not require treatment. A smaller disc bulge that directly compresses a nerve root and causes severe radiculopathy likely warrants intervention.
Why a Second Opinion Matters
After two decades of treating cervical spine conditions, I’ve come to believe that seeking a second opinion for spine problems is not just advisable; it’s essential for many patients. The treatment you receive can profoundly impact your quality of life for years to come, making it crucial to explore all your options before committing to any intervention.
The Reality of Treatment Variability
The world of spine treatment includes a remarkably wide range of approaches, philosophies, and available procedures. Not all spine specialists offer the same treatments, and recommendations can vary dramatically depending on whom you consult. Some surgeons primarily perform fusion procedures and may recommend fusion even when motion-preserving alternatives exist. Other specialists focus on pain management and may suggest extensive conservative treatments that delay necessary interventions. Still others offer advanced minimally invasive procedures that many patients never hear about from their initial consultation.
This variability means that the first opinion you receive, while given in good faith, may not represent all available options. A second opinion from a specialist with different training and expertise can reveal treatment possibilities you didn’t know existed.
When to Seek a Second Opinion
Several situations strongly suggest the need for a second opinion. If you’re told that fusion surgery is your only option for a disc bulge without clear spinal instability, seek another perspective. Modern minimally invasive techniques can often address disc problems without fusion. When conservative treatment hasn’t provided adequate relief after 6-12 weeks of appropriate care, it may be time to consider surgical intervention.
If you’re experiencing progressive weakness in your arm or shoulder despite treatment, don’t delay seeking additional evaluation, as prolonged nerve compression can cause permanent damage. When you feel uncertain or uncomfortable about a recommended treatment plan, trust your instincts and seek another opinion. And if your current provider seems rushed, dismissive, or unwilling to thoroughly explain your condition and options, find someone who will take the time to educate and partner with you in decision-making.

What Makes an Opinion Truly “Second”
A meaningful second opinion comes from a provider with different expertise or a perspective from your first consultation. If you saw a surgeon who specializes in fusion procedures, seek a second opinion from a specialist experienced in motion-preserving techniques. If your initial evaluation was performed by a pain management physician, consider consulting a spine surgeon to determine whether definitive treatment might be appropriate. The goal is to gain a complete picture of your options, not simply to hear the same recommendation repeated.
Understanding Your Condition: The Foundation for Advocacy
One of the most important aspects of getting a second opinion is gaining a deeper understanding of your specific condition. Take your MRI images to your consultation, not just the radiology report. Skilled specialists can review images directly and may identify findings that weren’t emphasized in the written report.
Ask specific questions about why you have symptoms, such as:
- What exactly is compressed or inflamed
- What the natural progression of your condition is likely to be without intervention
- What all available treatment options are, what outcomes you can realistically expect from each option
- What risks and recovery timelines are associated with different treatments
Understanding your condition empowers you to make informed decisions rather than simply following recommendations without clarity about the rationale. You become a partner in your care rather than a passive recipient of treatment.
Conservative Treatment Approaches
For most patients with C4-C5 disc bulges, an initial trial of conservative treatment is appropriate and often successful. Research indicates that approximately 75-90% of patients with cervical disc herniations improve with comprehensive conservative care.9 However, the key is “comprehensive” care; not all conservative treatments are equally effective, and the quality of implementation matters significantly.
Physical Therapy and Exercise
Structured physical therapy forms the cornerstone of conservative treatment for many patients. However, not all physical therapy is the same. A qualified therapist specializing in cervical spine conditions should design a program tailored to your specific presentation.
Cervical traction involves a gentle mechanical force that temporarily increases the space in the neural foramen, potentially reducing nerve root compression. A 2024 systematic review examining conservative treatments for lumbar disc herniation found that physical therapy approaches, including traction, showed effectiveness, and similar principles apply to cervical disc conditions.10 Traction can be performed manually by a therapist or using specialized devices. The treatment typically involves intermittent traction sessions of 15-20 minutes.
Strengthening exercises target deep neck flexors, which support proper cervical alignment and reduce disc stress. Exercises include chin tucks performed multiple times daily, neck resistance exercises performed with proper technique, and scapular stabilization exercises to improve posture and reduce neck strain. These exercises work by strengthening the muscles supporting the cervical spine and reducing the load on compromised discs.
Postural training and ergonomic education address the underlying mechanical stresses that may have contributed to your disc problem. Your therapist should evaluate your workspace setup, sleeping positions, and daily activities, then provide specific recommendations for improvement. Even small adjustments in posture and ergonomics can significantly reduce disc stress over time.
Manual therapy involves hands-on techniques to improve neck mobility and reduce muscle tension. Gentle mobilization techniques can be beneficial, though aggressive manipulation should be avoided in the presence of a disc bulge. The goal is to restore normal movement patterns without exacerbating nerve compression.
Medications for Symptom Management
While medications don’t heal disc bulges, they can manage symptoms during the healing process and make physical therapy more tolerable.
Non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen or naproxen reduce inflammation around the compressed nerve root. These medications work by inhibiting inflammatory mediators. However, prolonged use carries risks including gastrointestinal bleeding, cardiovascular effects, and kidney problems. NSAIDs should be used at the lowest effective dose for the shortest duration necessary.
Neuropathic pain medications like gabapentin or pregabalin specifically target nerve pain, which often responds poorly to traditional pain relievers. These medications work by modulating nerve signal transmission. They can be particularly effective for radiating arm pain and paresthesias. Side effects may include drowsiness, dizziness, and weight gain, requiring dose adjustment and monitoring.
Muscle relaxants address painful muscle spasm that often accompanies disc problems. Short-term use can break the cycle of pain and spasm. However, these medications typically cause drowsiness and aren’t suitable for long-term use.
Oral corticosteroids provide more potent anti-inflammatory effects than NSAIDs. A short course of oral steroids may be prescribed for acute severe inflammation. However, steroids carry significant side effects with prolonged use, and evidence for long-term benefit is limited.
Interventional Pain Management
When conservative therapies and medications provide insufficient relief, interventional procedures offer additional options before considering surgery.
Cervical epidural steroid injections deliver corticosteroids directly into the epidural space surrounding the compressed nerve root. The procedure is performed under fluoroscopic guidance to ensure accurate needle placement. Injections can provide temporary relief by reducing inflammation, allowing patients to participate more effectively in physical therapy. However, epidural injections typically provide temporary rather than permanent relief, with benefits lasting weeks to months. Multiple studies show variable success rates, and some patients experience no benefit. Risks include infection, bleeding, nerve injury, and rare but serious complications like spinal cord damage.
Selective nerve root blocks target a specific nerve root with a combination of corticosteroid and local anesthetic. These injections serve both diagnostic and therapeutic purposes. If a selective nerve root block temporarily eliminates your symptoms, it confirms that the targeted nerve root is your pain generator. This information can guide treatment decisions, including surgical planning if conservative measures fail.
Duration and Expectations
How long should you persist with conservative treatment? This depends on several factors, including symptom severity, the rate of improvement, the impact on your daily function, and the presence or absence of neurological deficits.
Most spine specialists recommend 6-12 weeks of comprehensive conservative treatment before considering surgery, provided you’re not experiencing progressive weakness or other alarming signs. However, if symptoms are improving gradually, continuing conservative care for a longer period may be appropriate. Conversely, if you’ve completed an adequate trial of appropriate conservative treatment without meaningful improvement, continuing the same ineffective treatments indefinitely isn’t in your best interest.
It’s important to understand that conservative treatment success doesn’t mean the disc bulge disappears or returns to normal. Rather, it means that inflammation resolves, nerve irritation diminishes, and symptoms improve to an acceptable level even though the underlying structural abnormality may persist. For many patients, this represents a successful outcome that allows them to avoid surgery and maintain good function.
When Conservative Treatment Isn’t Enough
For some patients, conservative treatment doesn’t provide adequate relief. Recognizing when conservative approaches have failed and surgical intervention should be considered, is crucial for preventing permanent nerve damage and unnecessary prolonged disability.

Clear Indications for Surgical Consideration
Progressive motor weakness represents perhaps the most urgent indication for surgical evaluation. If you’re experiencing increasing weakness in your shoulder or arm despite conservative treatment, nerve damage may be progressing. Prolonged compression can lead to permanent muscle atrophy and functional loss that won’t fully recover even after successful decompression. Don’t delay seeking surgical evaluation if the weakness is worsening.
Severe, intractable pain that significantly impairs quality of life warrants surgical consideration when conservative treatments have been exhausted. Pain that prevents sleep, interferes with work, or limits basic daily activities represents more than an inconvenience; it’s a legitimate indication of the need for definitive treatment. Some patients endure months or years of severe pain with conservative treatments that aren’t working, hoping surgery can be avoided. However, this approach can lead to unnecessary suffering and disability.
Failed conservative treatment after an appropriate trial suggests that your condition requires more definitive intervention. If you’ve undergone 8-12 weeks of comprehensive conservative care, including physical therapy, appropriate medications, activity modifications, and possibly epidural injections without meaningful improvement, continuing the same approaches indefinitely makes little sense. This doesn’t mean you’ve failed—it means your condition requires a different treatment strategy.
Cervical myelopathy occurs when the disc bulge compresses the spinal cord rather than just the nerve root. Symptoms may include difficulty with balance and coordination, hand clumsiness affecting fine motor tasks, changes in gait or walking pattern, and, in severe cases, bowel or bladder dysfunction. Myelopathy requires urgent evaluation and typically warrants surgical decompression to prevent permanent spinal cord damage.
The Risk of Delaying Necessary Surgery
While avoiding surgery is often a reasonable goal, unnecessarily delaying surgery when it’s genuinely needed carries risks. Prolonged nerve compression can cause irreversible nerve damage, leading to permanent weakness and sensory loss. Chronic pain can cause central sensitization, where the nervous system becomes hyperreactive to pain signals, making the condition harder to treat even after successful decompression. Extended disability from severe symptoms may result in job loss, financial stress, and significant psychological impact. Muscle atrophy from denervation may not fully recover even after the nerve compression is relieved.
The decision about when conservative treatment has failed, and surgery should be considered, isn’t always clear-cut. This is another reason why second opinions are valuable. An experienced spine specialist can help you weigh the potential benefits of continued conservative care against the risks of delaying surgical intervention.
Surgical Treatment Options
If conservative treatment hasn’t provided adequate relief and surgery becomes necessary, understanding your options is essential. Not all surgical procedures are equal; they vary dramatically in invasiveness, recovery time, long-term outcomes, and impact on spinal function.
Traditional Surgical Approaches
Anterior Cervical Discectomy and Fusion (ACDF) has been the standard surgical treatment for cervical disc problems for decades. The procedure involves accessing the spine through the front of the neck, removing the entire damaged disc, inserting a bone graft or cage to maintain disc height, and fusing the C4 and C5 vertebrae together using a metal plate and screws.
How it works: Through a horizontal incision in the front of the neck, the surgeon moves aside the trachea and esophagus to access the spine. After completely removing the disc, a spacer is inserted between the vertebrae, and hardware is placed to promote solid bony fusion over time.
Recovery: Patients typically spend 1-2 days in the hospital. Complete fusion takes 3-6 months, during which significant activity restrictions apply. Many patients require narcotic pain medications for several weeks after surgery. Return to full activities typically takes 6-12 weeks or longer.
Outcomes and limitations: While ACDF effectively relieves radicular pain in many cases, it has significant drawbacks. A 2024 study found that fusion carries an 11% risk of adjacent segment disease requiring reoperation, as fusion increases mechanical stress on adjacent disc levels, accelerating their degeneration.11 The fused segment no longer moves, permanently altering cervical biomechanics and reducing overall neck flexibility. Dysphagia, or difficulty swallowing, occurs in 10-50% of patients after ACDF, though symptoms usually improve over time. The fusion may fail to heal properly in 5-10% of cases, potentially requiring revision surgery. Hardware complications, including screw loosening, plate migration, or bone graft collapse, may necessitate additional surgery.
Posterior Cervical Foraminotomy accesses the spine from the back of the neck and involves removing a small portion of the facet joint to enlarge the neural foramen through which the nerve root exits.
How it works: Through an incision at the back of the neck, the surgeon removes bone to decompress the nerve root. This approach may preserve more disc material than anterior approaches and typically doesn’t require fusion.
Potential advantages: The procedure may preserve motion better than fusion, can sometimes be performed using minimally invasive techniques, and has lower rates of swallowing difficulties compared to anterior approaches.
Limitations: The posterior approach isn’t suitable for all types of disc bulges, particularly large central bulges. Traditional open posterior approaches involve significant muscle dissection, leading to considerable postoperative pain. Decompression may be incomplete if the main pathology is anterior to the nerve root.
Artificial Disc Replacement aims to maintain motion at the affected segment while addressing the disc problem. The procedure is similar to ACDF but uses an artificial disc prosthesis instead of fusion.
Theoretical benefits: Preservation of segmental motion, potentially lower risk of adjacent segment disease compared to fusion, and theoretically faster return to activities. However, real-world outcomes are more complex. Device wear and failure can occur over time, sometimes requiring revision surgery. Not all patients are candidates—those with facet joint arthritis, osteoporosis, or prior neck surgery are typically excluded. The artificial disc may not perfectly replicate the mechanics of a natural disc. Some patients develop heterotopic ossification, where abnormal bone growth limits motion despite the artificial disc. The cost is often substantially higher than fusion.
Understanding Surgical Risks and Recovery
All surgical procedures carry inherent risks. For cervical spine surgery, potential complications include infection, bleeding, nerve injury, spinal cord injury, dysphagia, voice changes from nerve injury, hardware complications, and failure to relieve symptoms. The risk of these complications varies depending on the specific procedure, the surgeon’s experience, and patient factors.
Recovery expectations also vary widely. Traditional open procedures typically require longer recovery times, significant postoperative pain management, activity restrictions for months, and risk of prolonged disability from complications. More advanced minimally invasive approaches offer dramatically different recovery experiences, as discussed in the next section.
Deuk Laser Disc Repair®: A Motion-Preserving Alternative
After witnessing the limitations and complications of traditional cervical spine surgery throughout my training and career, I became convinced that a better approach was needed. This led to the development of Deuk Laser Disc Repair® (DLDR), a minimally invasive, motion-preserving procedure that addresses the pathological disc material while leaving healthy structures intact.
A Different Philosophy of Treatment
Traditional cervical spine surgery operates on a simple premise: remove the entire disc and either fuse the vertebrae or insert an artificial disc. This approach has several fundamental flaws. It treats the entire disc as the problem when, in fact, only a small portion is damaged. It permanently alters spinal biomechanics through fusion or artificial implants. It requires significant tissue dissection, leading to prolonged recovery. And it carries a substantial risk of complications, including adjacent segment disease.
DLDR® takes an entirely different approach: Precisely remove only the damaged portion of the disc causing symptoms, leave the healthy disc intact to preserve function, maintain natural spinal motion without fusion or hardware, and minimize tissue trauma through advanced endoscopic techniques.
How Deuk Laser Disc Repair® Works
DLDR® is performed through a tiny 4-7mm incision, so small it can be covered with a simple band-aid. Through this minimally invasive opening, a specialized endoscope provides high-definition visualization of the surgical field.
Using advanced laser technology, only the damaged disc material compressing the nerve root is targeted and removed, typically just 5-10% of the total disc. The laser’s precision allows work around delicate neural structures without the collateral damage inherent in traditional open surgery.
Because most of the disc remains intact and functional, there’s no need for fusion, bone grafts, metal plates, screws, or artificial disc replacement. The natural disc continues to provide cushioning and allow normal motion. The procedure typically takes approximately one hour to perform.
The Science Behind Precision
The key to DLDR®’s success lies in its precision. Traditional surgery requires large incisions, muscle stripping, and significant bone removal to access the problem disc. These approaches are inherently traumatic to surrounding tissues, explaining the prolonged recovery and potential complications.
DLDR® causes minimal tissue disruption through several mechanisms. The endoscope accesses the disc through natural tissue planes. The laser removes only pathological disc material without damaging healthy tissue. No bone removal is required, preserving structural integrity. Surrounding muscles, nerves, and blood vessels remain undisturbed.
This precision directly translates into the patient experience. Because tissues aren’t unnecessarily traumatized, patients typically experience minimal postoperative pain. Most walk out of recovery within an hour and return to work within days rather than months.
Recovery Timeline and Outcomes
One of the most dramatic differences between DLDR® and traditional surgery is the recovery experience.
Day of surgery: Most patients notice significant pain relief as soon as they wake from twilight anesthesia. They leave the recovery room within an hour, typically without significant discomfort. Patients go home the same day with no hospital stay required.
First week: The tiny incision heals within days. Most patients require only over-the-counter pain medication, if anything. Many return to desk work within 3-5 days.
2-4 weeks: Complete healing occurs. Patients can resume most normal activities with minor restrictions depending on their condition. No prolonged physical therapy is needed because the spine’s natural biomechanics have been preserved.
Long-term: Because no fusion was performed, no adjacent segment disease develops. Because no hardware was implanted, no device-related complications occur. Patients maintain a full range of motion in their necks and can expect normal function for decades.
Recent research examining minimally invasive endoscopic approaches for cervical disc pathology has demonstrated excellent outcomes with significantly lower complication rates than traditional open procedures.12 An earlier study found that endoscopic cervical discectomy provided pain relief similar to that of traditional ACDF while preserving motion and reducing surgical complications.13
Benefits Beyond Pain Relief
The advantages of DLDR® extend far beyond simply relieving symptoms.
Preservation of natural anatomy: Because we’re not removing the entire disc or fusing vertebrae, the normal anatomy and biomechanics of the cervical spine remain intact. This preservation of natural function is perhaps the most significant long-term benefit.
No hardware complications: Without metal plates, screws, or artificial discs, there are no hardware-related complications. You won’t set off metal detectors, and you’ll never need hardware removal surgery.
Minimal scarring: The 4-7mm incision heals with virtually no visible scar. Most patients forget which side of their neck the incision was on within a few months.
No narcotics needed: The procedure is so precise that postoperative narcotic pain medication is typically unnecessary. This is increasingly important given the opioid crisis and the risks of long-term narcotic use.
Proven outcomes: DLDR® has been published in peer-reviewed medical literature documenting its safety and effectiveness.14 This isn’t experimental; it’s an established, proven procedure with excellent long-term results and a 99.6% success rate in eliminating disc-related pain with zero surgical complications.
Who Benefits from DLDR®
DLDR® effectively treats most cases of C4-C5 disc bulge, including contained disc bulges with nerve root compression, disc protrusions causing radicular symptoms, broad-based bulges with focal areas of nerve compression, failed conservative treatment with persistent symptoms, and annular tears with associated inflammation.
The best way to determine if you’re a candidate is to have your MRI reviewed by our team. You can upload your imaging studies through our secure portal for a complimentary review and virtual consultation.
Get Your Free Consultation and MRI Review

Patient Perspectives: Real Recovery Stories
Understanding treatment options through research and medical explanations is important, but hearing from real patients who have walked this path can provide an invaluable perspective. Here are experiences from patients who faced cervical disc problems and chose minimally invasive treatment.
Military Veteran’s Journey to Motion-Preserving Surgery
A veteran from California with herniations at C5-C6 and C6-C7 came to our facility after being told he needed both discs replaced with artificial implants. He described the proposed procedure as “putting tank treads on my car”—fundamentally changing his spine’s structure and function.
After reviewing his MRI, we determined he was an excellent candidate for DLDR® instead. We performed the procedure on the affected areas, removing only the damaged disc material while preserving the healthy portions. He reported feeling a sense of ease he hadn’t felt in over 10 years. Read more about his experience.
His story illustrates an important point: the first recommendation you receive may not represent all available options. He traveled across the country to explore alternatives to the hardware-heavy approach initially recommended, and that second opinion completely changed his treatment trajectory.
When Prior Surgery Doesn’t Solve the Problem
Another patient came to us after undergoing traditional fusion surgery that failed to provide adequate relief. She experienced 90% of her neck pain returning within months of her initial procedure. When she sought our evaluation, we found that the fusion hadn’t addressed all of the pathology and that an adjacent segment had developed problems.
Using DLDR®, we were able to address the remaining disc pathology without performing another fusion. Within 24 hours, she reported 90% pain relief—a dramatic improvement from her prior surgery experience. Read her full testimonial.
Her experience demonstrates that even after failed traditional surgery, motion-preserving alternatives can still provide relief. Many patients assume that once they’ve had one neck surgery, their options become increasingly limited. In reality, advanced minimally invasive techniques can often salvage situations where traditional approaches haven’t worked.
These patient stories reinforce the central message of this article: taking the time to understand your condition thoroughly, seeking second opinions when appropriate, and exploring all available treatment options can make the difference between years of ongoing problems and complete symptom resolution.
Living with a C4-C5 Disc Bulge: Practical Strategies
While pursuing definitive treatment for your C4-C5 disc bulge, implementing practical strategies can help you manage symptoms and potentially prevent worsening. These recommendations are based on biomechanical principles and clinical experience with thousands of patients.

Sleep Position and Pillow Selection
Poor sleeping positions can significantly aggravate cervical disc problems. Proper sleep ergonomics is essential for symptom management.15
Back sleeping (optimal): This position maintains neutral spinal alignment and evenly distributes weight. Use a pillow that supports the natural curve of your neck without propping your head too high. The goal is to keep your head in line with your spine. Consider a cervical contour pillow designed to support your neck’s natural curve.
Side sleeping (acceptable with proper support): If you prefer side sleeping, use a pillow that fills the space between your ear and the mattress, keeping your head level with your spine. A pillow between your knees can improve overall spinal alignment.
Stomach sleeping (avoid completely): This position forces your neck into prolonged rotation and extension, placing maximum stress on cervical discs and facet joints. This is the worst possible position for cervical disc problems and should be avoided entirely.
Ergonomics and Posture
Modern life, particularly desk work and smartphone use, places significant stress on the cervical spine. Proper ergonomics can reduce this burden substantially.16
Workstation setup: Position your computer monitor at eye level, approximately 20-26 inches from your eyes. Keep your keyboard and mouse at elbow height to avoid shoulder elevation. Use a chair with proper lumbar support and armrests to reduce neck strain. Take breaks every 30 minutes to stand, stretch, and change positions.
Smartphone use: The average human head weighs 10-12 pounds in neutral position, but can exert 40-60 pounds of force on the cervical spine when tilted forward to look at a phone. Bring your phone to eye level rather than dropping your head down. Limit prolonged smartphone use when possible.
Driving: Adjust your seat and steering wheel to maintain an upright posture. Use your rearview mirrors properly so you don’t need to turn your head excessively. Consider using a lumbar roll to support your lower back, which can indirectly improve your neck posture.
Exercise and Physical Activity
Appropriate exercise can be beneficial, but choosing the right activities is crucial.
Recommended activities: Walking provides low-impact cardiovascular exercise that doesn’t stress the neck. Gentle yoga with poses that promote flexibility without excessive neck extension can be helpful. Swimming, particularly freestyle and backstroke (avoiding butterfly and breaststroke, which require repetitive neck extension), offers excellent exercise. Stationary cycling provides cardiovascular benefits with minimal neck stress.
Neck-specific exercises: Chin tucks gently strengthen deep neck flexors by drawing your chin back, not down. Scapular squeezes pull the shoulder blades together to strengthen postural muscles. Side bending involves gentle lateral neck movements to maintain mobility. Isometric strengthening uses resistance against hand pressure in multiple directions without moving.
Activities to avoid: High-impact activities like running or contact sports should be avoided. Overhead work or exercises place excessive stress on the cervical spine. Heavy weight lifting, especially overhead presses, can exacerbate symptoms. Activities requiring prolonged neck extension, like painting ceilings, should be minimized.
What to Avoid
Certain activities and positions can significantly worsen symptoms of a C4-C5 disc bulge.
Prolonged static postures: Holding your neck in any position for extended periods increases disc pressure. This includes reading in bed, watching television while reclined, or working on a laptop without proper ergonomics.
Heavy lifting: Avoid lifting anything over 10-15 pounds during the acute phase. When you must lift, use proper technique: bend at the knees, keep the object close to your body, and avoid twisting motions.
Sudden movements: Quick, jerking neck movements can exacerbate symptoms or cause additional disc injury. Move deliberately and avoid sudden twisting or whipping motions.
Vibration exposure: Prolonged exposure to vibration, such as operating heavy machinery or riding in vehicles on rough roads, can aggravate disc problems.
Stress Management and Sleep Quality
Chronic pain creates stress, and stress can amplify pain perception, creating a vicious cycle. Implementing stress management strategies can help break this pattern. Mindfulness meditation and relaxation techniques reduce muscle tension and pain perception. Cognitive behavioral therapy helps develop healthy coping strategies for chronic pain. Maintaining social connections and engaging in enjoyable activities within your limitations can help preserve mental health. Adequate sleep is essential for healing and pain management, though pain often disrupts sleep.
Key Takeaways
C4-C5 disc bulge is a common cervical spine condition that can significantly impact quality of life, but understanding your diagnosis and exploring all treatment options empowers you to make informed decisions about your care.
- The C4-C5 segment is located in the mid-cervical spine and is subject to substantial mechanical stress during daily activities. When the disc bulges and compresses the C5 nerve root, characteristic symptoms develop: shoulder pain and weakness, radiating arm pain, sensory changes in the lateral upper arm, and neck stiffness with limited range of motion.
- Recent research continues to advance our understanding of optimal treatment approaches. Approximately 75-90% of patients improve with comprehensive conservative treatment, including physical therapy, appropriate medications, and activity modifications. However, those who don’t respond within 8-12 weeks or who develop progressive weakness should consider more definitive intervention.
- The importance of accurate diagnosis cannot be overstated. Not all disc bulges cause symptoms, and not all arm pain originates from disc problems. Comprehensive clinical correlation between your symptoms, physical examination findings, and imaging studies is essential for appropriate treatment planning.
- Seeking a second opinion represents an act of self-advocacy, not distrust of your initial provider. The spine treatment landscape includes numerous approaches with vastly different implications for your long-term health. Getting multiple perspectives ensures you understand all available options before committing to any intervention.
- If conservative treatment hasn’t worked for you, surgical options range from traditional fusion procedures to advanced motion-preserving techniques. Traditional approaches like ACDF permanently alter spinal mechanics through fusion, carry risks of adjacent segment disease, and require lengthy recovery periods. Modern minimally invasive techniques, particularly Deuk Laser Disc Repair®, offer superior alternatives: precise removal of only damaged disc material, preservation of healthy disc structure and natural motion, proven 99.6% success rate with zero surgical complications, same-day outpatient procedure with recovery measured in days, and no need for fusion, hardware, or long-term activity restrictions.
- Perhaps most importantly, don’t accept unnecessary suffering or disability. While avoiding surgery when possible is often reasonable, unnecessarily delaying surgery when genuinely needed carries risks, including irreversible nerve damage, chronic pain sensitization, and prolonged disability. Your quality of life matters, and effective treatment options exist when conservative approaches aren’t working.
- If you’ve been diagnosed with a C4-C5 disc bulge, consider uploading your MRI images for a complimentary expert review and virtual consultation. Understanding all of your options is the first step toward finding the treatment approach that’s right for you.
Frequently Asked Questions (FAQs)
Q: What are the symptoms of a C4-C5 disc bulge?
A: C4-C5 disc bulge typically causes compression of the C5 nerve root, producing a characteristic pattern of symptoms. The hallmark symptom is shoulder pain and weakness, particularly affecting the deltoid muscle. This manifests as difficulty lifting your arm away from your body, reduced shoulder strength, and a deep aching pain in the shoulder region.
Additional symptoms include radiating pain down the outer arm, sometimes extending to the thumb side of the forearm; numbness and tingling in the C5 dermatome distribution, affecting the lateral upper arm and outer shoulder; biceps weakness, making it difficult to bend your elbow against resistance; and diminished biceps reflex on clinical examination.
Many patients also experience neck pain and stiffness that limits rotation and extension. Symptoms often worsen with certain neck positions and may interfere with sleep. Unlike more distal nerve compressions, C4-C5 problems typically affect the proximal arm and shoulder while sparing the hand.
It’s important to note that imaging findings don’t always correlate with symptoms. You can have a disc bulge visible on MRI without pain, or experience significant discomfort with relatively mild imaging findings. This is why clinical correlation between symptoms, examination findings, and imaging studies is essential for accurate diagnosis.
Q: How is a C4-C5 disc bulge treated?
A: Treatment for C4-C5 disc bulge follows a stepwise approach, starting with conservative care and progressing to surgical intervention if needed.
Conservative treatment (typically tried first for 8-12 weeks): Physical therapy, including cervical traction, strengthening exercises, and postural training, forms the foundation. A 2024 systematic review found that comprehensive physical therapy approaches were effective for disc conditions.10 Medications, including NSAIDs, neuropathic pain medications, and sometimes short courses of oral corticosteroids, help manage symptoms. Activity modifications and ergonomic adjustments reduce disc stress. Interventional procedures like epidural steroid injections may be considered if initial treatments don’t provide adequate relief.
Surgical treatment (when conservative approaches fail): Traditional options include anterior cervical discectomy and fusion, which permanently fuses vertebrae together, or posterior foraminotomy to decompress the nerve root. However, these procedures have significant limitations, including loss of motion, risk of adjacent segment disease, and prolonged recovery.
Advanced minimally invasive options, such as Deuk Laser Disc Repair®, offer motion-preserving alternatives. This procedure removes only the damaged portion of the disc while preserving healthy tissue, maintains natural spinal motion without fusion or hardware, provides same-day outpatient treatment with recovery in days rather than months, and has a proven 99.6% success rate in eliminating disc-related pain with zero surgical complications.
The key is matching treatment to your specific situation based on symptom severity, duration, functional impact, and response to conservative care. If conservative treatment hasn’t worked after an appropriate trial, don’t delay seeking surgical evaluation.
Q: Can a C4-C5 disc bulge heal on its own?
A: Yes, many C4-C5 disc bulges can improve significantly without surgical intervention, though it’s important to understand what “healing” means in this context. Research indicates that patients can experience substantial improvement with appropriate conservative treatment.17
The natural history involves several mechanisms. First, acute inflammation around the nerve root subsides over time, reducing pain even if compression persists. Second, the immune system can gradually resorb some herniated disc material, particularly with disc extrusions and sequestrations where material has escaped beyond the disc boundaries.3 Third, the nervous system can adapt to chronic compression through neuroplastic mechanisms. Fourth, the disc may gradually desiccate and retract somewhat from neural structures.
However, “healing” doesn’t mean the disc returns to its pre-injury state. Once the annulus fibrosus develops tears or weakness, permanent structural changes typically persist. While symptoms may resolve, the underlying disc degeneration remains. This is why some patients experience recurrent symptoms months or years later.
Key factors influencing whether conservative treatment will succeed include the size and type of disc pathology, the degree of nerve compression, the presence of spinal canal stenosis, your age and overall health, and adherence to treatment recommendations.
If symptoms persist beyond 6-12 weeks of comprehensive conservative treatment, or if progressive weakness develops, surgical evaluation is warranted. Modern minimally invasive procedures can provide definitive resolution when conservative approaches fail, without the extensive recovery and complications of traditional surgery.
Q: How long does it take to recover from C4-C5 disc bulge surgery?
A: Recovery time varies dramatically depending on which surgical procedure is performed.
Traditional fusion surgery (ACDF): Patients typically spend 1-2 days in the hospital. Complete bone fusion takes 3-6 months. Most patients need narcotic pain medications for several weeks after surgery. Return to desk work typically takes 4-6 weeks, with return to physical labor requiring 3-6 months. Activity restrictions apply throughout the fusion period, and physical therapy is usually required for months.
Traditional posterior foraminotomy: Hospital stays of 1-2 days are common. Recovery to normal activities typically takes 8-12 weeks. Postoperative pain from muscle dissection can be significant. Physical therapy is usually needed during recovery.
Advanced minimally invasive procedures (Deuk Laser Disc Repair®): The contrast is dramatic. Same-day outpatient procedure with no hospital stay required. Most patients experience immediate relief from arm pain. Return to desk work within 3-5 days. Complete healing within 2-3 weeks. No prolonged activity restrictions. No need for extensive physical therapy.
Recent research examining minimally invasive endoscopic approaches has demonstrated significantly shorter recovery times than traditional open procedures, while maintaining equivalent or superior clinical outcomes.12
The difference stems from the fundamental approach. Traditional surgeries involve significant tissue trauma, bone removal, and often permanent alteration of spinal anatomy. Minimally invasive endoscopic approaches work through tiny incisions, preserve healthy tissue, maintain normal biomechanics, and cause minimal trauma to surrounding structures.
Q: What is the difference between a disc bulge and a disc herniation?
A: While these terms are sometimes used interchangeably in casual conversation, they describe slightly different stages of disc pathology with important implications for treatment.
Disc bulge: The entire disc circumference extends symmetrically beyond the vertebral margins. The annulus fibrosus (outer layer) remains intact with no tear. The nucleus pulposus (inner gel) hasn’t escaped. This represents early degenerative changes and may or may not cause symptoms. Treatment typically starts with conservative approaches.
Disc herniation (includes protrusion, extrusion, and sequestration): The annulus fibrosus has torn or ruptured. The nucleus pulposus pushes through the weakened or torn annulus. The herniated material may cause inflammation in and around the disc, including nerve roots. Symptoms tend to be more severe than simple bulges. Treatment approaches are similar but may progress to surgery sooner if symptoms are severe.
Q: Should I get a second opinion for my C4-C5 disc bulge?
A: Yes, getting a second opinion is highly advisable for anyone diagnosed with a cervical disc bulge, particularly if surgery has been recommended. Here’s why.
Treatment variability is substantial: The spine treatment landscape includes diverse approaches with dramatically different implications. Some surgeons primarily perform fusion procedures and may recommend fusion even when motion-preserving alternatives exist. Other specialists focus on pain management and may suggest extensive conservative treatments that delay necessary interventions. Still others offer advanced minimally invasive procedures that many patients never hear about from their initial consultation.
Second opinions reveal options: Many patients discover treatment options they didn’t know existed when consulting with a specialist with different training and expertise. A meaningful second opinion comes from a provider with different capabilities than your first consultation—if you saw a fusion surgeon, seek an opinion from a motion-preservation specialist.
The stakes are high: Cervical spine surgery can profoundly impact your quality of life for years or decades. Fusion permanently alters neck mechanics and carries risks of adjacent segment disease. Some patients undergo unnecessary surgery for conditions that could have improved with continued conservative care. Other patients endure prolonged unnecessary suffering when effective treatment exists.
Getting timely second opinions helps ensure you receive appropriate treatment before prolonged nerve compression causes permanent damage.
At Deuk Spine Institute, we offer complimentary MRI reviews and virtual consultations with no cost or obligation. You can upload your imaging studies through our secure portal to receive an expert assessment. Many patients who thought fusion was their only option discovered they were candidates for motion-preserving procedures that offered superior outcomes with dramatically faster recovery.
Q: Will I need to avoid certain activities with a C4-C5 disc bulge?
A: Activity modification is an important component of managing C4-C5 disc bulge, particularly during the acute phase. However, the goal is strategic modification that facilitates healing, not complete avoidance of all activities.
Activities to avoid or minimize: Heavy lifting over 10-15 pounds during the acute phase places excessive load on the cervical spine. Overhead work or exercises stress the neck in extension. High-impact activities like running or contact sports create jarring forces. Prolonged static postures, especially with forward head position, maintain sustained disc compression. Sudden jerking movements can exacerbate symptoms or cause additional injury.
Activities you can typically continue: Walking provides excellent low-impact cardiovascular exercise. Light household chores with proper body mechanics are usually fine. Desk work with an appropriate ergonomic setup can continue. Gentle yoga, avoiding extreme neck positions, may be helpful. Swimming, particularly freestyle and backstroke, is a good form of exercise.
Activity progression: As symptoms improve with treatment, activities can gradually be resumed. The key is listening to your body and avoiding movements that reproduce symptoms. If an activity causes increased pain that persists beyond the activity itself, it’s too much too soon.
Long-term considerations: If you undergo conservative treatment with symptom resolution, you may be able to return to most normal activities with appropriate precautions. If you undergo successful minimally invasive surgery like DLDR®, you can typically return to full activities within weeks with no long-term restrictions since natural spinal mechanics are preserved.
If you undergo traditional fusion surgery, some activity restrictions may be permanent. Fusion eliminates motion at the treated segment, and activities requiring extensive neck mobility or high-impact forces may need to be limited to protect adjacent levels from accelerated degeneration.
The bottom line is that activity modifications should be individualized based on your specific condition, symptoms, and treatment approach. A qualified healthcare provider can help you develop an appropriate activity plan that facilitates healing while maintaining fitness and function.
Sources
1: https://pubmed.ncbi.nlm.nih.gov/20404946/
2: https://pubmed.ncbi.nlm.nih.gov/24768732/
3: https://pubmed.ncbi.nlm.nih.gov/28072796/
4: https://pmc.ncbi.nlm.nih.gov/articles/PMC4522454/
5: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)32027-4/
6: https://pmc.ncbi.nlm.nih.gov/articles/PMC6690080/
7: https://pmc.ncbi.nlm.nih.gov/articles/PMC12113928/
8: https://pubmed.ncbi.nlm.nih.gov/23963016/
10: https://pmc.ncbi.nlm.nih.gov/articles/PMC12242731/
11: https://deukspine.com/blog/neck-surgery-c5-c6-c7-recovery-time-and-advantages
12: https://www.mdpi.com/2077-0383/13/7/2122
13: https://jss.amegroups.org/article/view/4838/
14: https://pmc.ncbi.nlm.nih.gov/articles/PMC3683169/
15: https://deukspine.com/blog/best-sleeping-positions-pillows-neck-pain-relief
16: https://deukspine.com/blog/best-office-chairs-for-herniated-disc


