
Procedure Not Recommended
Risks, Recurrence Rates & Better Alternatives

⚠️ While Deuk Spine Institute can perform Discectomy, we do not recommend it.
This page explains why — learn the risks before consenting to this procedure.
UNDERSTANDING THE PROCEDURE
While there are legitimate medical reasons, financial incentives and predictable failure rates drive surgical recommendations.
Sharp shooting pain, numbness, and weakness radiating down arms or legs from herniated disc material compressing nerve roots. Discectomy removes the herniated fragment, often providing immediate leg pain relief, but leaves the damaged disc and torn annular tear untreated.
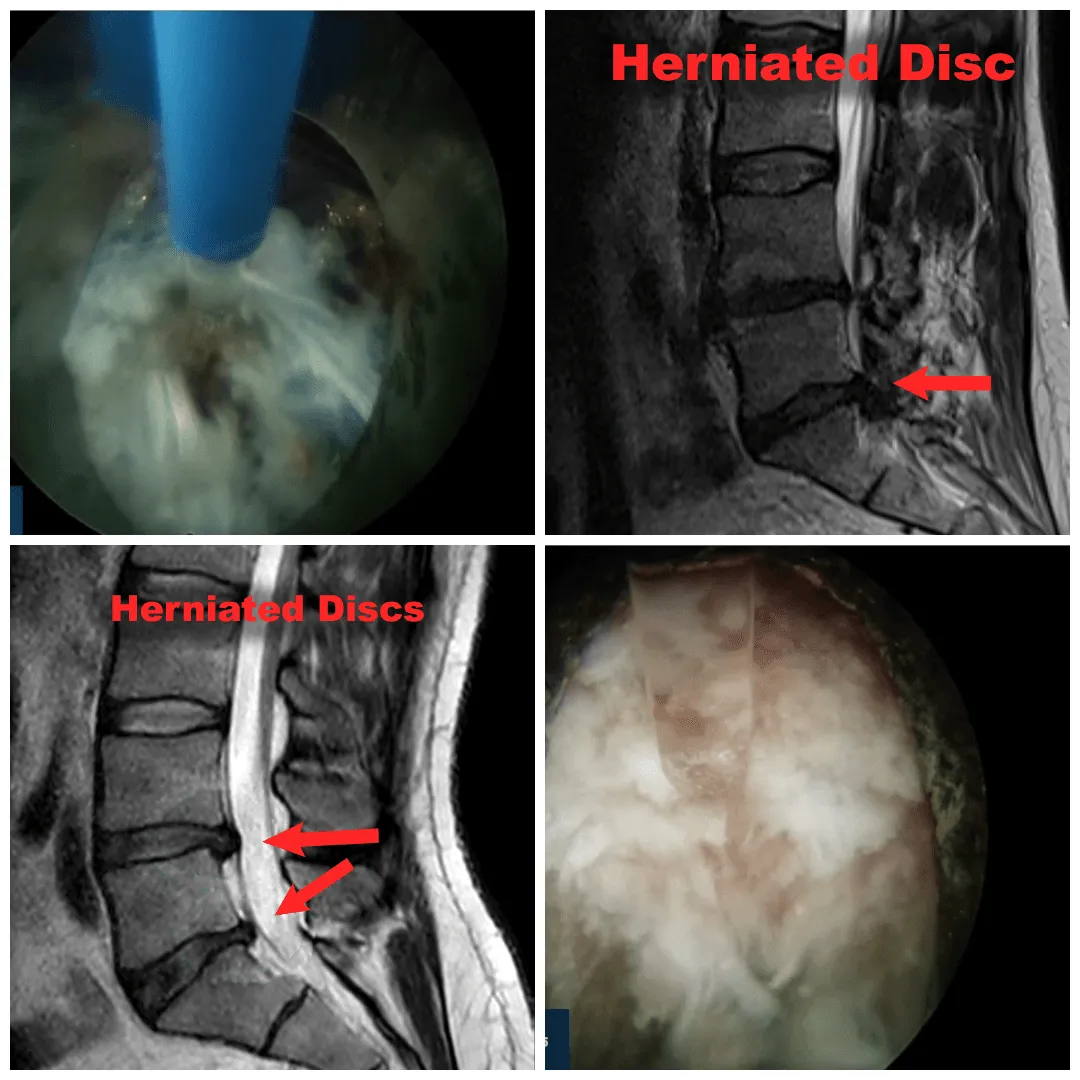
Severe leg pain from herniated disc compressing sciatic nerve roots. While discectomy can eliminate leg pain by removing the herniation, it doesn't repair the hole in the disc wall, leading to 20-30% recurrence rates as new disc material herniates through the same tear.
Rare condition where massive disc herniation compresses multiple nerve roots, causing loss of bowel/bladder control. This true emergency represents less than 1% of cases, yet surgeons often reference it to create false urgency for routine sciatica.
Canal narrowing from disc herniation contributing to nerve compression. Often cited as justification for discectomy even when symptoms could be managed with less invasive approaches.
Discectomy takes only 45-90 minutes but generates $3,000-$8,000 in surgeon fees and $15,000-$40,000 total charges. A surgeon performing 3 discectomies daily can generate $20,000-$25,000 in personal income.
Immediate leg pain relief leads to initial patient satisfaction, masking the underlying problem: the torn disc continues degenerating, back pain persists, and 20-30% experience recurrent herniations requiring repeat surgery.
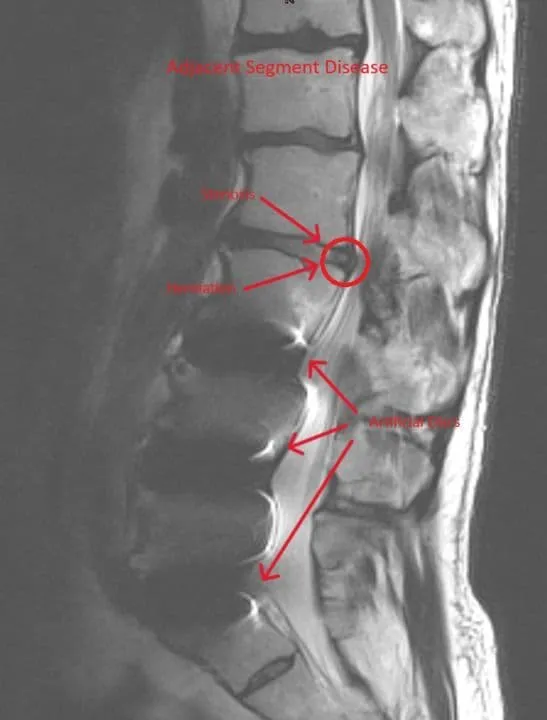
Because discectomy removes disc material without repairing the annular tear, the same disc commonly herniates again. Patients may undergo 2-3 discectomies over several years, each generating full reimbursement. Recurrent patients comprise 30-40% of surgical volume.
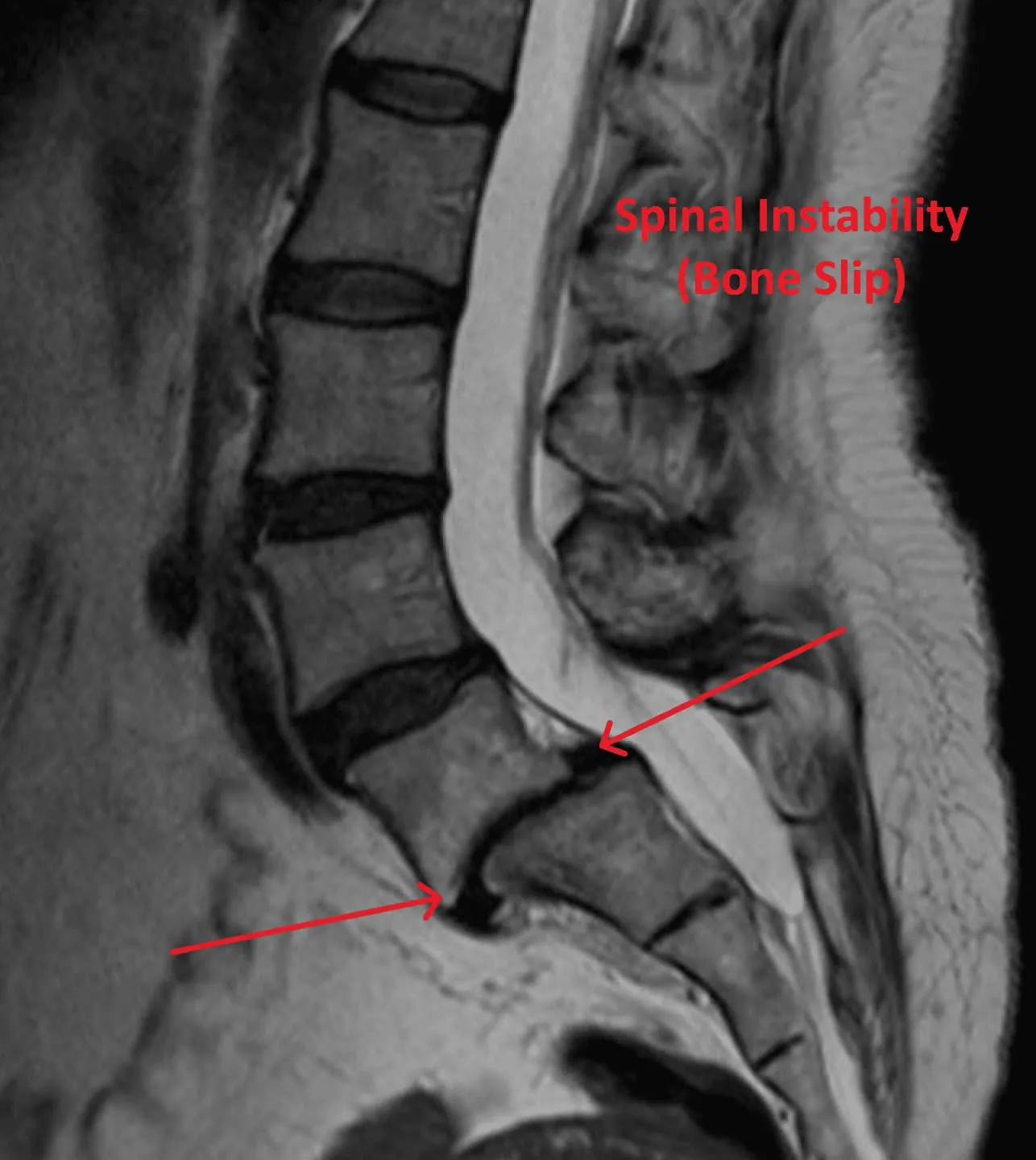
When multiple discectomies fail or the disc collapses, surgeons recommend fusion as the 'definitive solution.' Discectomy to repeat discectomy to fusion represents a predictable revenue stream, plus epidural scar tissue creates chronic pain requiring lifelong pain management.
THE SURGICAL PROCESS
The videos below contain real surgical footage. Viewer discretion is advised.
A 1-3 inch incision is made along the spine to access the herniated disc level.
The tough connective tissue covering the spine muscles is cut and removed.
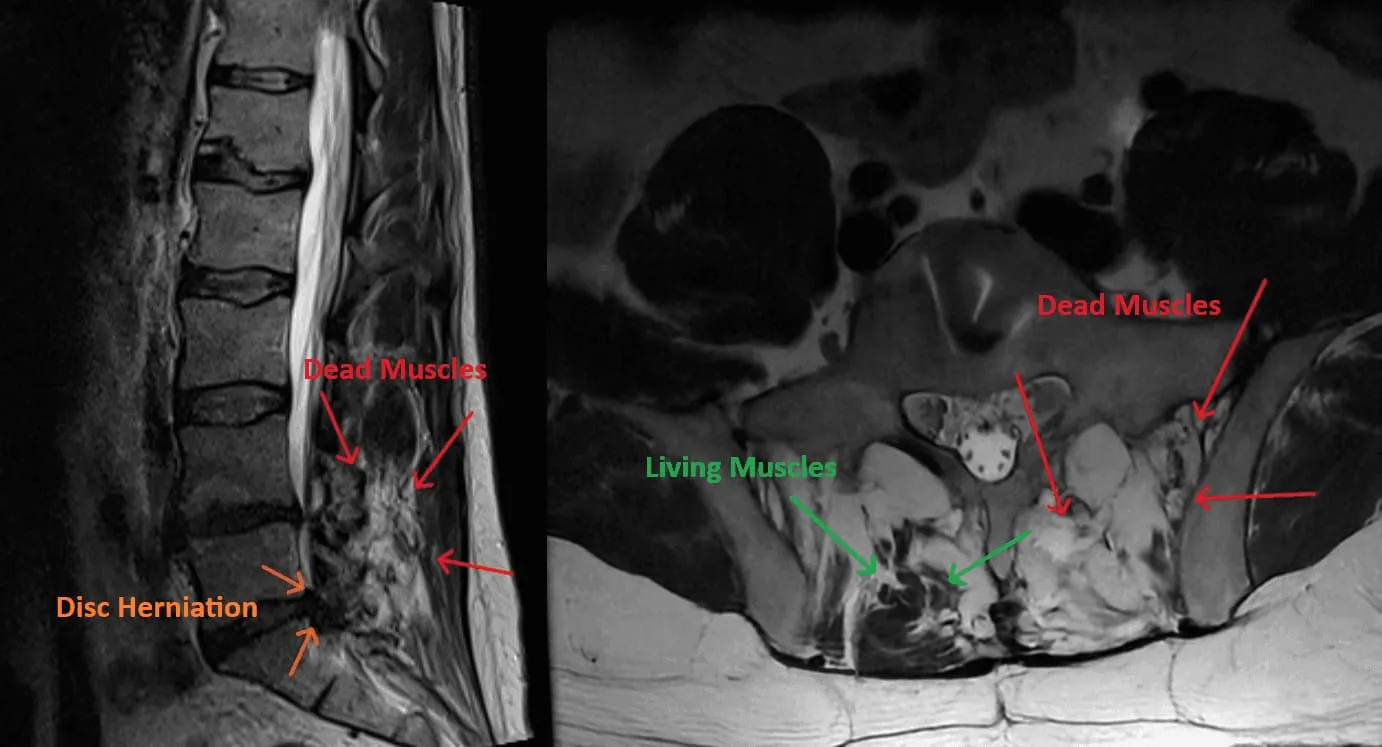
Spinal muscles are stripped from the bone to expose the vertebral structures.
The bony protrusion and supporting ligaments are cut away to create access to the spinal canal.
Part of the lamina is removed to access the disc and nerve roots beneath.
Facet joints that provide spinal stability are partially or fully destroyed to reach the disc.
The compressed nerve root is retracted to the side, risking permanent nerve damage.
A hole is cut in the outer disc wall (annulus fibrosus) to access the herniated material inside.
Herniated disc material is removed with forceps, but the torn annulus is left unrepaired, leading to recurrence.
CRITICAL RISKS
20 documented reasons with supporting images and surgical footage.
Images and videos below contain real surgical procedures and medical imagery.








DOCUMENTED COMPLICATIONS
Images and videos below contain real surgical procedures and medical imagery.

Permanent nerve damage causing weakness, numbness, or paralysis from retraction during disc removal.

Post-surgical infection at the incision site or within the disc space (discitis), requiring IV antibiotics or reoperation.

20-30% recurrence rate as disc material herniates through the same untreated annular tear, requiring repeat surgery.

Stenosis persists or reoccurs commonly after discectomy, requiring additional decompression surgery.
WHAT WE RECOMMEND INSTEAD
Instead of removing disc material and leaving the annular tear untreated, Deuk Laser Disc Repair® uses endoscopic technology and laser precision to seal the torn annulus and repair the damaged disc — through an incision smaller than a fingernail.
Your disc material remains intact. No tissue removal, no structural damage, no weakening of the spinal segment.
Laser technology directly seals the annular tear — the actual source of herniation and inflammation that discectomy leaves completely untreated.
Outpatient procedure under light sedation. Walk out the same day — no hospital stay, no intubation, no opioids required.
95% patient satisfaction, 0.01% complication rate, and over 1,300 successful procedures performed by Dr. Deukmedjian.
Feature
Discectomy
Deuk Laser Disc Repair®
Procedure Type
❌ Invasive, removes disc material
✅ Minimally invasive, endoscopic
Incision Size
❌ 1–3 inches
✅ Less than 1/4 inch
Anesthesia
❌ General (intubated)
✅ Light IV sedation
Disc Treatment
❌ Removes disc fragments, doesn’t repair tear
✅ Laser seals annular tear and repairs disc
Bone Removal
❌ Yes — partial laminectomy required
✅ None
Hospital Stay
❌ 1–2 days inpatient
✅ Outpatient — go home same day
Recovery Time
❌ 4–6 weeks
✅ Days
Recurrence Rate
❌ 20–30% reherniation rate
✅ Rarely needed
Success Rate
❌ Initial relief fades — many need fusion
✅ 95% patient satisfaction
Repeat Surgery
❌ 90%+ need additional surgery
✅ Rarely needed
A BETTER ALTERNATIVE
Minimally invasive, outpatient procedure with a 0.01% complication rate and 95% patient satisfaction. No bone removal. No disc removal. Same-day recovery.
Patient Satisfaction
Complication Rate
Procedure Time