Laminectomy destroys stabilizing spinal structures, requires fusion in 40-50% of cases, and has less than a 20% success rate for eliminating chronic back pain. Discover safer, minimally invasive alternatives.
⚠️ While Deuk Spine Institute can perform Laminectomy, we do not recommend it.
This page explains why — learn the risks before consenting to this procedure.
Highly invasive: large incision and excessive cutting of normal tissues between skin and spine during laminectomy.
Excessive Bleeding
Excessive and unnecessary bleeding during and after surgery from muscle trauma by the surgeon.
Destroys Stabilizing Bones
Destruction of normal stabilizing bones including lamina and spinous process by the surgeon during laminectomy.
1) Destroys Stabilizing Ligaments
Destruction of normal stabilizing bones including lamina and spinous process by the surgeon during laminectomy.
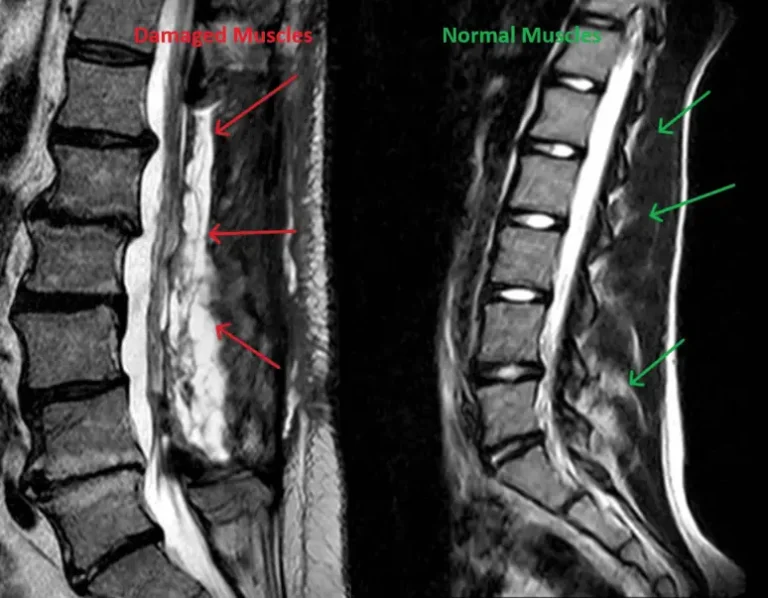
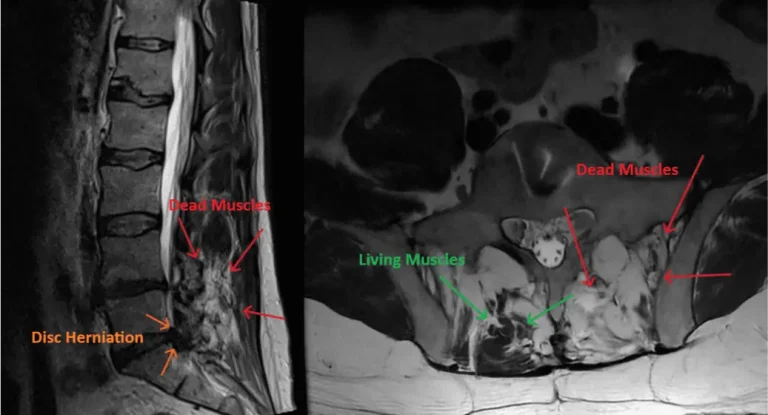
2) Destroys Spinal Muscles
Destruction of normal stabilizing bones including lamina and spinous process by the surgeon during laminectomy.
3) Excessive Scar Tissue
Excessive scar tissue forms around the spine and nerves after laminectomy
4) Complications Are Common
Complications are common after laminectomy
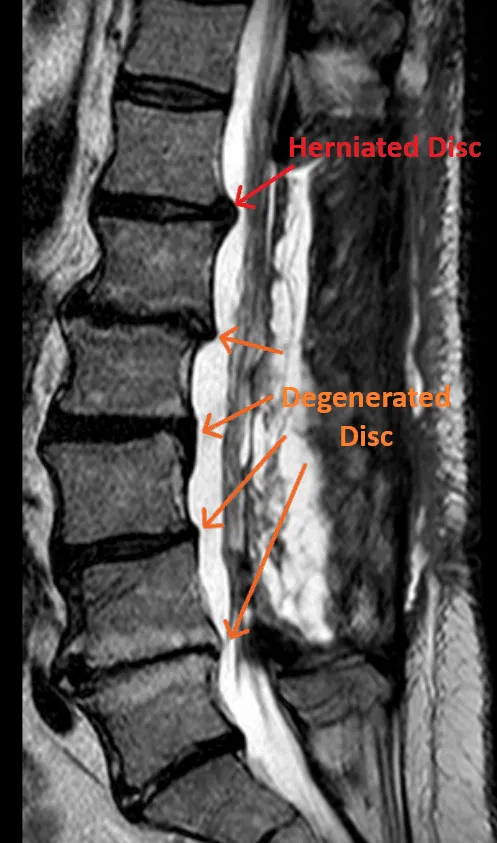
5) Disc Injuries Left Untreated
Disc herniations and degenerated discs are not treated when a laminectomy is performed. They are the most common cause of back and leg pain.
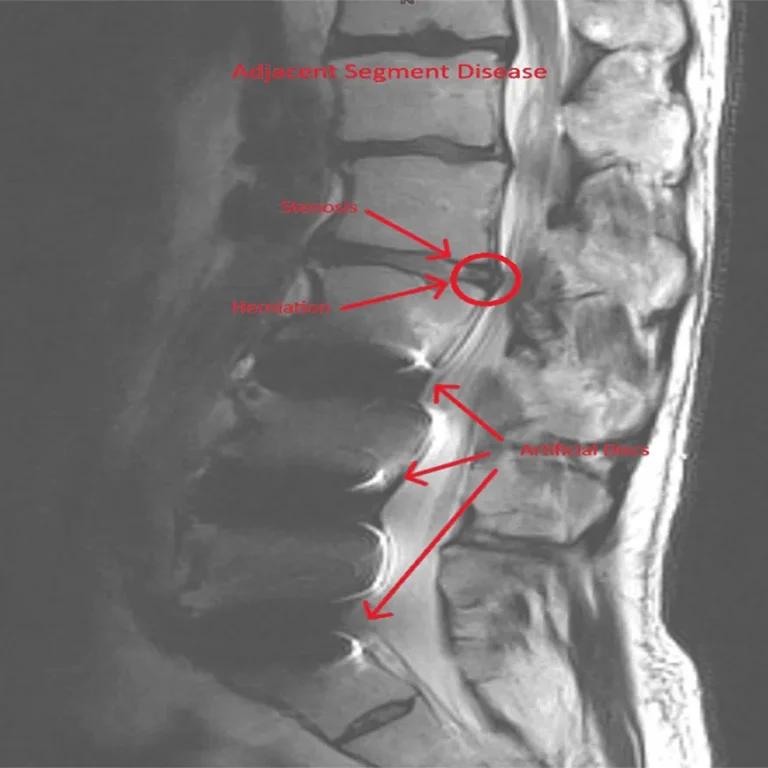
6) Adjacent Segment Disease
Adjacent segment disease is common after laminectomy and requires additional surgery.
7) Stenosis Persists or Returns
Stenosis either persists or reoccurs commonly after laminectomy and will require additional surgery such as Fusion.
Laminectomy does not treat back pain.
8) Severe Post-Operative Pain
Excessive postoperative pain always occurs after laminectomy due to muscle trauma and necrosis (death of muscles). During laminectomy the muscles are torn off the spine by the surgeon in order to get down to the lamina. The dying muscles cause severe postoperative pain that always requires opioid painkillers and muscle relaxers. Opioid painkillers are highly addicting, cause tolerance, abuse and even death from breathing failure.
Back Pain Gets Worse
Back pain becomes worse after laminectomy. Fusion will be recommended.
Spinal Fusion Often Required
Destruction of normal stabilizing bones including lamina and spinous process by the surgeon during laminectomy.
Long Operating Times
Long operating times are needed for laminectomy.
General Anesthesia Required
General intubated anesthesia is needed for laminectomy.
90%+ Need Additional Surgery
Additional surgery will be necessary in over 90% of patients having laminectomy.
Lifetime Pain Management
Most laminectomy patients end up in pain management for years after laminectomy.
DOCUMENTED COMPLICATIONS
What Can Go Wrong?
Graphic Medical Content
Images and videos below contain real surgical procedures and medical imagery.
Permanent nerve damage causing weakness, numbness, or paralysis in extremities.
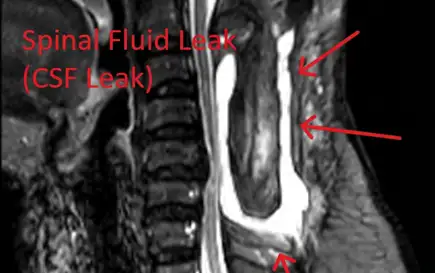
Spinal Fluid Leak
Dural tears leading to cerebrospinal fluid leaks, requiring additional repair surgery.
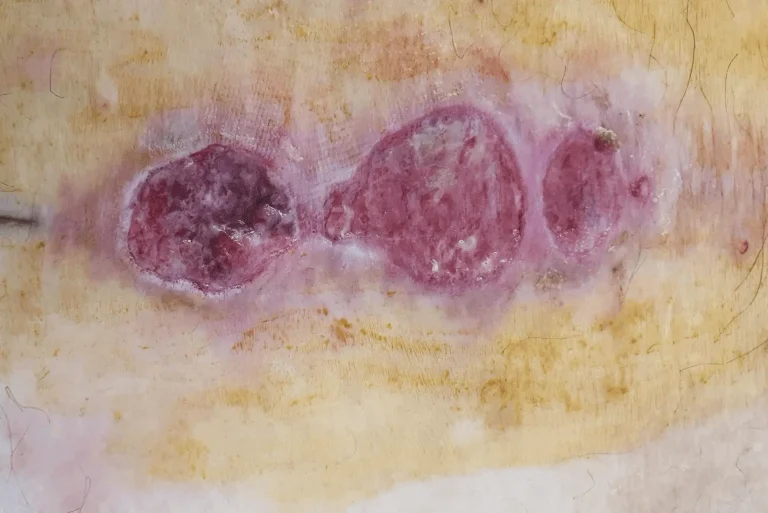
Infection
Post-surgical infection at the incision site or deeper within the spinal structures.
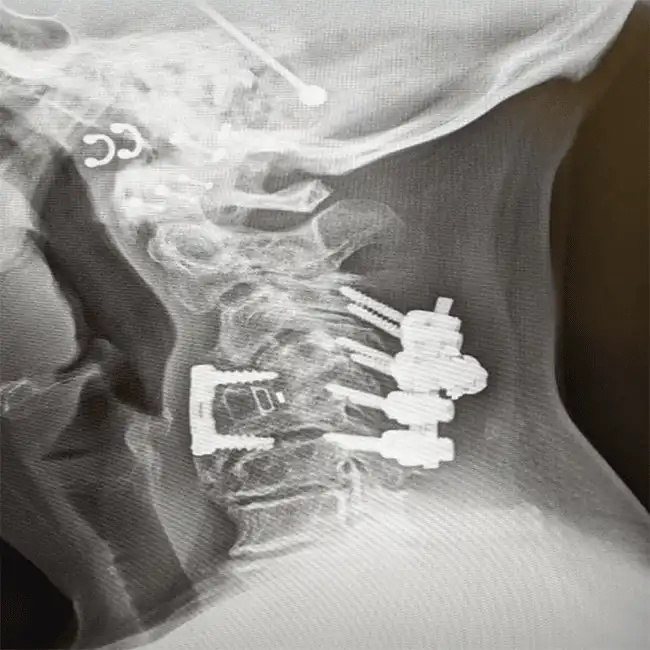
Spinal Instability
Removal of stabilizing structures causes instability requiring fusion with screws and rods.
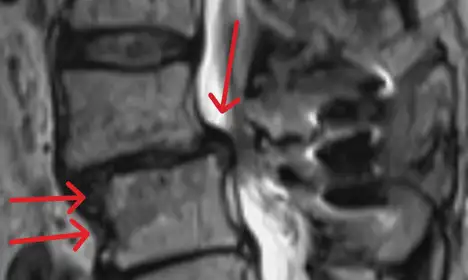
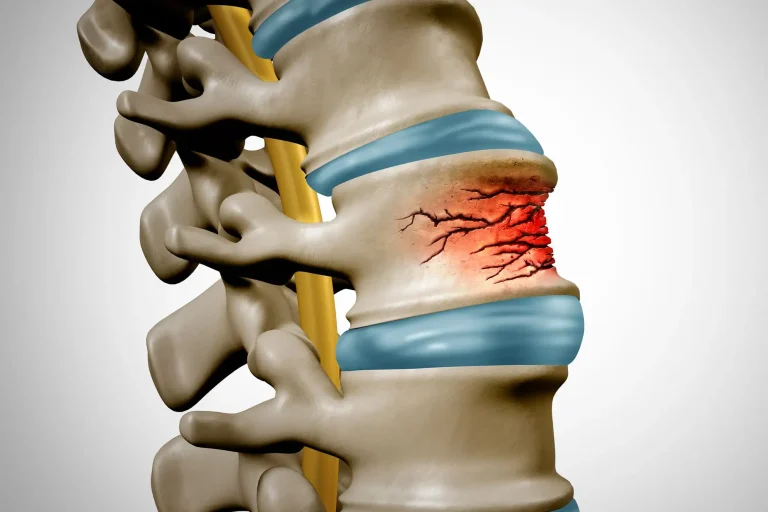
Fractured Vertebrae
Weakened spine from bone removal can lead to vertebral fractures and collapse.
Residual Stenosis
Stenosis persists or reoccurs commonly after laminectomy, requiring additional surgery.
WHAT WE RECOMMEND INSTEAD
Deuk Laser Disc Repair®: A Safer, Proven Alternative
Instead of destroying your spine’s stabilizing structures, Deuk Laser Disc Repair® uses endoscopic technology and laser precision to treat the actual source of pain — the damaged disc — through an incision smaller than a fingernail.
No Bone Removal
Your spine’s stabilizing structures remain completely intact. No lamina, spinous process, or facet joint destruction.
Treats the Root Cause
Laser technology directly repairs the damaged disc — the actual source of 85% of chronic back pain that laminectomy ignores.
Same-Day Recovery
Outpatient procedure under light sedation. Walk out the same day — no hospital stay, no intubation, no opioids required.
Proven Results
95% patient satisfaction, 0.01% complication rate, and over 1,300 successful procedures performed by Dr. Deukmedjian.
Feature
Laminectomy
Deuk Laser Disc Repair®
Procedure Type
❌ Highly invasive, open surgery
✅ Minimally invasive, endoscopic
Incision Size
❌ 3–6 inches
✅ Less than 1/4 inch
Anesthesia
❌ General (intubated)
✅ Light IV sedation
Bone Removal
❌ Yes — lamina & spinous process
✅ None
Treats Disc Injury
❌ No — disc left untreated
✅ Yes — laser repairs the disc
Hospital Stay
❌ 1–3 days inpatient
✅ Outpatient — go home same day
Recovery Time
❌ 6–12 weeks
✅ Days
Complication Rate
❌ High — frequent complications
✅ 0.01%
Success Rate
❌ Less than 20%
✅ 95% patient satisfaction
Repeat Surgery
❌ 40–50% need fusion in 5 years
✅ Rarely needed
A BETTER ALTERNATIVE
Deuk Laser Disc Repair®
Minimally invasive, outpatient procedure with a 0.01% complication rate and 95% patient satisfaction. No bone removal. No muscle destruction. Same-day recovery.