



By Dr. Ara Deukmedjian, MD
Board-Certified Neurosurgeon, Deuk Spine Institute
Medically reviewed on December 24, 2025
Medical disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.
Introduction: Clarifying Common Misconceptions About Disc Conditions
Patients experiencing back or neck pain often receive imaging reports describing either a “bulging disc” or a “herniated disc.” While these terms appear throughout medical literature and diagnostic reports, the clinical distinction between them is frequently overstated. Understanding the true nature of these conditions is essential for making informed decisions about your spinal health and treatment options.
In a general sense, bulging and herniated discs fall under the same category of spinal conditions, though they are anatomically distinct. A bulging disc involves the disc extending beyond its normal space, whereas a herniated disc occurs when the inner material actually breaks through the outer layer. Despite these anatomical differences, the treatment approach is often the same, as both conditions can result in similar levels of discomfort. Because the severity of pain doesn’t always correlate with the type of displacement, distinguishing between these terms is vital for a precise MRI interpretation and for tailoring a recovery plan.
As a board-certified spine surgeon with extensive experience treating thousands of patients with disc-related conditions, I have observed that the key to effective treatment lies not in the diagnostic label but in understanding the underlying pathophysiology, the patient’s specific symptoms, and the most appropriate intervention for their individual case.
The Anatomy of Intervertebral Discs
To properly understand disc conditions, we must first examine the structure and function of intervertebral discs themselves. These remarkable anatomical structures serve as shock absorbers and flexible joints between the vertebrae of the spine, allowing for movement while protecting the spinal cord and nerve roots.
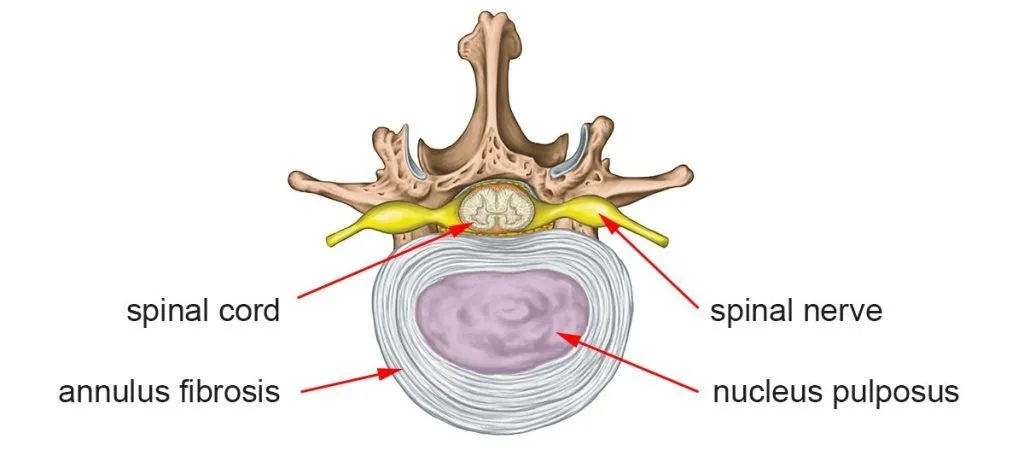
Each intervertebral disc consists of two primary components:
The nucleus pulposus: This gel-like center contains a high concentration of water and proteoglycans, providing the disc with its shock-absorbing properties. In healthy, young adults, the nucleus pulposus may contain up to 80-90% water content.
The annulus fibrosus: This tough outer ring consists of approximately 15-25 concentric layers of collagen fibers, arranged in alternating orientations to provide structural integrity and containment of the nucleus pulposus.
The health and function of these discs depend on several factors, including adequate hydration, proper biomechanics, and the integrity of the surrounding spinal structures. As we age or experience trauma, these discs undergo degenerative changes that can lead to various pathological conditions.
Understanding Disc Displacement: Bulging Versus Herniation
Bulging Discs: Characteristics and Pathophysiology
A bulging disc represents a condition where the outer boundary of the annulus fibrosus extends beyond its normal anatomical position relative to the adjacent vertebral bodies. This displacement typically occurs circumferentially or over a broad area of the disc’s perimeter, rather than in a localized region.
The development of a bulging disc is generally a gradual process associated with disc degeneration. As the disc loses hydration and the structural integrity of the annulus fibrosus weakens, the disc may flatten and spread outward. This process is often part of the natural aging continuum and may be observed on imaging studies in individuals who experience no symptoms whatsoever.
It is important to recognize that bulging discs are extremely common. Research indicates that disc bulging can be identified on MRI scans in a significant percentage of asymptomatic individuals, with prevalence increasing with age. This finding underscores the critical point that imaging abnormalities do not always correlate with clinical symptoms.
Herniated Discs: Mechanisms and Clinical Significance
A herniated disc, also referred to as a ruptured disc or disc protrusion, occurs when the annulus fibrosus develops a tear or defect, allowing the nucleus pulposus to migrate through this opening. This represents a more focal, typically more acute, pathological process than disc bulging.
Disc herniation can manifest in several forms:
- Protrusion: The nucleus pulposus extends through a tear in the annulus but remains contained by the posterior longitudinal ligament.
- Extrusion: The nuclear material extends through the annulus fibrosus, with the base of the herniation narrower than its dome.
- Sequestration: A fragment of nuclear material completely separates from the parent disc and migrates into the spinal canal.
The clinical significance of a herniated disc often relates to the inflammatory cascade that follows the rupture of the annulus fibrosus. When nuclear material escapes its normal compartment, it triggers an immune response because this material is immunologically privileged under normal circumstances. This inflammation, rather than mechanical compression alone, frequently accounts for the pain and neurological symptoms patients experience.
The Clinical Reality: Why the Distinction Often Matters Less Than You Think
Throughout my career performing advanced spinal procedures, I have consistently observed that the severity of a patient’s symptoms does not reliably correlate with whether their imaging study shows a bulging or herniated disc. Some patients with significant disc herniations experience minimal symptoms, while others with modest disc bulging report debilitating pain.3
This phenomenon occurs because pain generation in disc pathology involves multiple factors beyond simple mechanical displacement. The inflammatory response within the annular tear, chemical irritation of nearby nerve roots, central sensitization of pain pathways, and individual differences in pain processing all contribute to the clinical presentation.
Furthermore, both bulging and herniated discs can produce identical symptom patterns when they result in:
- Chemical irritation of nerve roots through inflammatory mediators
- Mechanical compression of neural structures
- Disruption of normal spinal biomechanics
- Muscle spasm and protective guarding
From a treatment perspective, the management principles remain consistent regardless of the specific diagnostic terminology. Conservative interventions, pain management strategies, and surgical approaches, when indicated, follow similar algorithms based on symptom severity, functional impairment, and response to initial treatment rather than the precise anatomical classification of the disc abnormality.

Etiological Factors: What Causes Disc Degeneration and Displacement
Age-Related Disc Degeneration
The most common cause of both bulging and herniated discs is the natural degenerative process that affects intervertebral discs over time.4 Beginning as early as the second or third decade of life, discs gradually lose water content, and the structural components of both the nucleus pulposus and annulus fibrosus undergo biochemical changes.
This degeneration includes decreased proteoglycan content, alterations in collagen structure, calcification, and reduced cellular viability within the disc tissue. These changes compromise the disc’s ability to withstand mechanical stress and increase susceptibility to injury.
Biomechanical Stress and Repetitive Loading
Occupations and activities that involve repetitive spinal loading, prolonged sitting, frequent bending and twisting, or heavy lifting place excessive stress on intervertebral discs. Over time, this cumulative microtrauma accelerates degenerative changes and increases the risk of both bulging and herniation.
Research has demonstrated that certain occupational groups, including heavy laborers, professional drivers, and individuals who work in sustained awkward postures, face elevated risks of developing symptomatic disc disease.
Acute Trauma
While degeneration creates the underlying vulnerability, acute traumatic events often precipitate symptomatic disc herniation. Motor vehicle accidents, falls, sports injuries, and sudden lifting with poor technique can generate forces sufficient to tear the annulus fibrosus and displace nuclear material.
Interestingly, the traumatic event triggering symptoms may be relatively minor in patients with pre-existing degenerative changes. A simple movement, such as bending to pick up a light object, can be the “final insult” that triggers a herniated disc.
Genetic Predisposition
Emerging research has identified genetic factors that influence individual susceptibility to disc degeneration. Variations in genes encoding structural proteins, inflammatory mediators, and matrix-degrading enzymes have been associated with increased risk of disc disease.
Family history studies have demonstrated that first-degree relatives of individuals with disc herniation face substantially higher risks of developing similar conditions, independent of shared environmental factors.
Lifestyle Factors
Several modifiable lifestyle factors contribute to disc pathology:
- Obesity: Excess body weight increases mechanical loading on the spine, particularly in the lumbar region, accelerating degenerative processes.
- Smoking: Tobacco use impairs microvascular circulation to disc tissue, compromising nutrient delivery and waste removal, which accelerates degeneration.
- Physical inactivity: A sedentary lifestyle leads to weakening of the core musculature that normally supports proper spinal mechanics and reduces disc health by decreasing nutrient diffusion.
Searching for Answers Regarding Your Back or Neck Pain?
Upload your recent MRI for a free virtual consultation and MRI review with Dr. Ara Deukmedjian.

Clinical Presentation: Recognizing the Symptoms
Localized Axial Pain
Many patients with disc pathology experience neck or back pain in the region of the affected disc. This axial pain results from inflammation within the disc itself, particularly when annular tears are present. The pain may be constant or intermittent, often worsening with certain positions or activities.
Patients frequently report that sitting, bending forward, or performing twisting movements exacerbates their symptoms. Conversely, lying down or changing positions may provide relief.
Radicular Pain
When disc material displaces posteriorly or posterolaterally, it may affect nerve roots exiting the spinal canal at that level. This produces radicular pain—often described as sharp, shooting, or electric—that follows the distribution of the affected nerve.
In the lumbar spine, this commonly manifests as sciatica, with pain radiating from the lower back through the buttocks and down the leg. Cervical disc pathology may produce brachial neuralgia, with pain extending from the neck into the shoulder, arm, and hand.
It is crucial to understand that radicular pain arises primarily from chemical irritation and inflammation of the nerve root, rather than from simple mechanical compression. This explains why some patients experience severe radicular symptoms despite relatively modest disc displacement on imaging studies.
Neurological Deficits
In addition to pain, disc pathology may produce neurological deficits, including:
- Sensory Changes: Numbness, tingling, or altered sensation in the distribution of the affected nerve root.
- Motor Weakness: Reduced strength in muscles innervated by the compressed or inflamed nerve, potentially affecting specific movements or functional activities.
- Reflex Abnormalities: Diminished or absent deep tendon reflexes corresponding to the affected spinal level.
These neurological findings provide valuable diagnostic information and help localize the level of pathology during clinical examination.
Pain Patterns Based on Spinal Region
- Cervical disc pathology: Neck pain, shoulder pain, arm pain, hand numbness or weakness, and potentially headaches, particularly occipital or suboccipital in distribution.
- Thoracic disc pathology: Mid-back pain, chest wall pain that may be confused with cardiac or pulmonary conditions, and occasionally abdominal pain or lower extremity symptoms if severe central canal stenosis is present.
- Lumbar disc pathology: Lower back pain, buttock pain, leg pain following dermatomal patterns, foot numbness or weakness, and bowel or bladder dysfunction in severe cases of cauda equina syndrome.
30 Causes of Back Pain
Watch this video, where Dr. Ara Deukmedjian, MD, covers the 30 structural causes of back pain. Learn where your pain is originating from.
Diagnostic Evaluation: Advanced Imaging and Clinical Assessment
Clinical Examination
The diagnostic process begins with a comprehensive clinical evaluation, including detailed medical history, symptom characterization, physical examination with neurological testing, and assessment of functional limitations.
During examination, I evaluate spinal range of motion, palpate for areas of tenderness or muscle spasm, perform provocative maneuvers to reproduce symptoms, and conduct a thorough neurological assessment, including strength testing, sensory examination, and reflex evaluation.
Magnetic Resonance Imaging (MRI)
MRI represents the gold standard for imaging intervertebral discs and surrounding soft tissues. This modality provides excellent visualization of disc morphology, the presence and extent of bulging or herniation, neural compression, inflammatory changes, and other associated pathology such as facet joint arthropathy or spinal stenosis.1
However, it is essential to interpret MRI findings in the context of clinical symptoms. As previously noted, disc abnormalities on MRI are common in asymptomatic individuals, and the presence of imaging findings does not automatically indicate that these findings are the source of a patient’s pain.5
Complementary Imaging Studies
Radiographs (X-rays) help assess spinal alignment, detect instability, evaluate disc space height, and identify bony abnormalities or arthropathy.
CT scans may be utilized when detailed bony anatomy assessment is needed or when an MRI is contraindicated.
CT myelography involves injecting contrast material into the spinal canal, providing detailed visualization of neural compression when an MRI cannot be performed.
Electrodiagnostic Studies
Electromyography and nerve conduction studies can be valuable when clinical findings suggest nerve root involvement, helping to confirm nerve dysfunction, localize the affected nerve root level, differentiate radiculopathy from peripheral neuropathy, and provide prognostic information on nerve recovery potential.
Conservative Management: Non-Surgical Treatment Approaches
For the majority of patients with bulging or herniated discs, conservative treatment represents the appropriate initial approach. Many disc-related symptoms improve significantly with non-surgical interventions over weeks to months.
Activity Modification and Physical Therapy
Structured physical therapy programs focus on core strengthening exercises, flexibility and range-of-motion work, postural training and body mechanics education, and a graduated return to functional activities.
Evidence supports that directed exercise therapy can improve outcomes for patients with disc-related pain, though the specific exercise prescription should be individualized based on the patient’s symptoms and functional limitations.
Pharmacological Management
Medical management may include non-steroidal anti-inflammatory drugs to reduce inflammation and pain, muscle relaxants for associated muscle spasm, neuropathic pain medications for radicular symptoms, and short courses of oral corticosteroids for acute inflammatory episodes.
Opioid analgesics should be used judiciously and only for short-term management of severe acute pain, given the well-documented risks of dependence and limited long-term efficacy.
Interventional Pain Management
Epidural steroid injections can deliver anti-inflammatory medication directly to the affected nerve root region, potentially providing temporary relief and facilitating participation in rehabilitation. However, these injections provide symptomatic relief rather than addressing the underlying structural pathology.
Selective nerve root blocks may serve both diagnostic and therapeutic purposes, helping to confirm which nerve root is generating symptoms.
The Role and Limitations of Conservative Treatment
While many patients experience satisfactory improvement with conservative management, these approaches have important limitations. They do not repair damaged disc tissue, may provide only temporary symptom relief, and do not address the structural cause of nerve irritation. For patients who fail to achieve adequate improvement with conservative measures over an appropriate trial period, more definitive treatment may be warranted.2
Surgical Intervention: When and Why Surgery Becomes Necessary
Indications for Surgical Treatment
Surgical intervention for disc pathology may be indicated when:
- Conservative treatment has failed to provide adequate relief after an appropriate trial period (typically three to six months)
- Progressive neurological deficits are present, indicating ongoing nerve damage
- Severe symptoms significantly impair quality of life and functional capacity
- Cauda equina syndrome develops (a surgical emergency requiring immediate decompression)
- The patient has recurrent episodes of debilitating symptoms despite optimal conservative management
Limitations of Traditional Surgical Approaches
Conventional spine surgery for disc pathology has traditionally involved procedures such as:
- Discectomy and Microdiscectomy: Removal of herniated disc material compressing neural structures. While this can relieve acute radicular symptoms, it does not address the damaged disc itself and may increase the risk of recurrent herniation.
- Laminectomy: Removal of laminar bone to decompress neural elements. This procedure alters spinal anatomy and may contribute to instability.
- Spinal Fusion: Elimination of motion at the affected spinal segment through bone grafting and instrumentation. Fusion procedures sacrifice normal spinal mobility, alter biomechanics of adjacent segments (potentially accelerating adjacent level degeneration), involve substantial surgical trauma and recovery time, and carry significant risks including nonunion, instrumentation failure, and persistent pain.
Deuk Laser Disc Repair®: A Paradigm Shift in Treatment
At Deuk Spine Institute, we have pioneered an advanced approach that fundamentally differs from traditional spine surgery. The Deuk Laser Disc Repair® procedure represents a minimally invasive solution that addresses the pathophysiology of disc pain while preserving spinal anatomy and function.
This innovative technique utilizes precision laser technology to remove the obstructing nuclear material responsible for mechanical compression and chemical irritation, treating the underlying disc pathology.
The procedure offers several distinct advantages:
- Preservation of spinal motion: Unlike fusion procedures, Deuk Laser Disc Repair® maintains the spine’s natural flexibility and biomechanics.
- Minimal tissue disruption: The minimally invasive approach reduces surgical trauma, minimizes blood loss, and preserves important anatomical structures.
- Faster recovery: Patients typically experience significantly shorter hospital stays and recovery times than with traditional open spine surgery.
- Reduced complication rates: The refined technique and preservation of normal anatomy reduce the risk of surgical complications.
- Treatment of the root cause: Rather than simply removing herniated material, the procedure addresses the underlying disc degeneration and promotes healing.
- Same treatment for both conditions: Because bulging and herniated discs require the same therapeutic approach to address pain generation and structural pathology, this procedure is equally effective for both conditions.
Most importantly, clinical outcomes demonstrate that patients undergoing Deuk Laser Disc Repair® experience durable pain relief and functional improvement with an excellent safety profile. The procedure provides a definitive solution for patients who have not achieved satisfactory results with conservative treatment, without the drawbacks and risks associated with more invasive surgical alternatives.
How it Works
See firsthand, how our minimally invasive procedure helps patients find relief.
Prevention Strategies and Long-Term Spinal Health
Ergonomic Considerations
Proper workplace ergonomics, including appropriate desk and chair height, proper computer monitor positioning, regular postural changes, and supportive seating, can reduce cumulative spinal stress.
Physical Conditioning
Maintaining strong core musculature through targeted exercises provides dynamic support for the spine and reduces disc loading. A balanced fitness program should include cardiovascular conditioning, resistance training for core and supporting muscles, and flexibility exercises.
Body Mechanics
Using proper lifting techniques, avoiding prolonged static postures, and employing good body mechanics during daily activities can minimize excessive disc stress.
Weight Management
Maintaining a healthy body weight reduces biomechanical loading on the spine and decreases systemic inflammation that may contribute to disc degeneration.
Smoking Cessation
Discontinuing tobacco use can improve disc nutrition through enhanced microvascular circulation and reduces systemic inflammation.
Prognosis and Outcomes: What to Expect
Natural History
Many patients with disc-related symptoms experience gradual improvement with conservative treatment over weeks to months. However, outcomes vary considerably among individuals based on factors such as the specific nature and severity of disc pathology, the presence of complicating factors, patient age and overall health, and adherence to treatment recommendations.
Surgical Outcomes
For patients who require surgical intervention, outcomes depend on appropriate patient selection, the specific procedure performed, the surgeon’s expertise, and postoperative rehabilitation.
At Deuk Spine Institute, we have achieved exceptional outcomes with our minimally invasive Deuk Laser Disc Repair® procedure. The vast majority of patients experiencing significant pain relief, functional improvement, and high satisfaction rates. Our surgical guarantee reflects our confidence in this approach and our commitment to patient outcomes.
Long-Term Considerations
Spinal health requires ongoing attention even after successful treatment. Continued attention to ergonomics and body mechanics, maintenance of physical conditioning, weight management, and regular follow-up care contribute to long-term success and minimize the risk of developing problems at other spinal levels.
Find Relief. Get Answers. Live Pain-Free.
Recommended for a Fusion? Schedule your FREE Virtual Consultation and MRI Review with Dr. Deukmedjian today.
Free MRI consultation and review
FAQs
Q: Can I have both a bulging disc and a herniated disc simultaneously?
A: Yes, it is entirely possible to have multiple disc abnormalities at different spinal levels, or even at the same level. MRI studies frequently reveal multilevel disc degeneration with varying degrees of bulging or herniation. However, not all imaging abnormalities produce symptoms. During the clinical evaluation, we correlate imaging findings with your specific symptoms and physical examination findings to determine which disc pathology is clinically significant and warrants treatment. Many patients have incidental disc findings that are unrelated to their presenting complaints and do not require intervention.
Q: How long does it take to recover from disc-related pain?
A: Recovery timelines vary considerably depending on the severity of disc pathology, the selected treatment approach, and individual patient factors. With conservative treatment, many patients experience meaningful improvement within six to twelve weeks, though complete resolution may require several months. For patients undergoing Deuk Laser Disc Repair, recovery is typically much faster than with traditional spine surgery. Most patients are ambulatory within hours of the procedure, discharged within 23 hours, and able to return to light activities within days to weeks. Full recovery and return to unrestricted activities generally occur within several weeks to a few months, which represents a substantial advantage over conventional surgical approaches requiring months of recovery.
Q: Is it possible to prevent disc problems from developing?
A: While we cannot completely prevent age-related disc degeneration, which represents a normal aspect of aging, we can significantly reduce the risk of symptomatic disc problems through lifestyle modifications. Maintaining a healthy body weight, engaging in regular exercise that strengthens core musculature, practicing proper ergonomics and body mechanics, avoiding tobacco use, and addressing any underlying conditions that may affect spinal health all contribute to disc preservation. For individuals with existing disc degeneration, these measures become even more critical to prevent progression and minimize the risk of developing symptomatic bulging or herniation. Early intervention with appropriate conservative care when symptoms first develop may also prevent progression to more severe disc pathology.
Q: When should I seek medical evaluation for back or neck pain?
A: You should seek prompt medical evaluation if you experience severe pain that does not improve with rest and over-the-counter medications, pain accompanied by neurological symptoms such as numbness, tingling, or weakness in your extremities, bowel or bladder dysfunction (which may indicate cauda equina syndrome requiring emergency treatment), pain following significant trauma such as a fall or motor vehicle accident, or pain accompanied by unexplained fever or weight loss. For less severe symptoms, it is reasonable to try conservative measures such as activity modification and over-the-counter anti-inflammatory medications for several days to a few weeks. However, if your symptoms persist beyond this period, worsen progressively, or significantly impact your quality of life and functional abilities, professional evaluation is warranted to determine the underlying cause and an appropriate treatment strategy.
TLDR: An Expert Perspective on Disc Health
The distinction between bulging and herniated discs, while anatomically relevant, often holds less clinical significance than commonly assumed. Both conditions represent points along the continuum of disc degeneration, and both can produce similar symptoms through comparable pathophysiological mechanisms. The severity of pain and functional impairment does not reliably correlate with whether imaging reveals a bulge or a herniation.
What matters most is accurate diagnosis through comprehensive clinical evaluation, correlated with advanced imaging; appropriate treatment selection based on symptom severity and response to conservative measures; and, when surgery is indicated, choosing a procedure that addresses the underlying pathology while preserving spinal function.
At Deuk Spine Institute, we have developed advanced treatment protocols that reflect the latest understanding of disc pathophysiology. Our Deuk Laser Disc Repair® procedure represents a significant advancement over traditional spine surgery, providing definitive treatment for both bulging and herniated discs with minimal invasiveness, faster recovery, and excellent long-term outcomes.
If you are experiencing symptoms of disc-related pain that have not responded adequately to conservative treatment, I encourage you to schedule a consultation to discuss your specific situation. We offer complimentary MRI reviews to help determine whether you may be a candidate for our advanced treatment approaches.
Your spinal health significantly impacts your overall quality of life, functional capacity, and independence. You deserve an accurate diagnosis and access to the most advanced treatment options available. We are committed to helping patients achieve lasting relief and return to the activities they value.
Sources
1: https://pubmed.ncbi.nlm.nih.gov/17530454
2: https://deukspine.com/blog/best-treatment-for-herniated-disc
3: https://pubmed.ncbi.nlm.nih.gov/10707396/


