


By Dr. Ara Deukmedjian
Board-Certified Neurosurgeon
Medically reviewed on June 3, 2026
Medical Disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with a qualified spine specialist about your specific condition and treatment options.
Key Points
✓ The answer depends almost entirely on which surgery is being recommended. “Spine surgery” is not one operation. It is a spectrum ranging from procedures that eliminate motion permanently to procedures that preserve it entirely.
✓ Spinal fusion permanently eliminates motion at every fused segment. That loss is intentional, irreversible, and comes with documented downstream consequences: adjacent segment disease occurring in 5–18% of fusion patients at 4–14 years. ¹
✓ Decompression procedures: laminectomy, discectomy, foraminotomy do not inherently fuse the spine and do not eliminate segmental motion, though tissue removal can alter biomechanics in ways that affect functional range at higher rates of activity. ²
✓ Artificial disc replacement is marketed as motion-preserving. The evidence supports a modest advantage over fusion in measured range of motion at the operated level, but the benefit narrows over time and comes with its own reoperation and implant-related failure risks. ³ ⁴
✓ The most motion-preserving option currently supported by peer-reviewed data is full-endoscopic spine surgery. A procedure that does not remove the disc, place hardware, or alter the spine’s structural anatomy. There is nothing to lose motion from because nothing is removed or fused with the Deuk Laser Disc Repair®.
✓ The honest answer to “will spine surgery limit my range of motion permanently?” is: it depends on what they are planning to do to your spine, not what they call it. Ask the question about the specific procedure, not the marketing label.

What “Range of Motion” Actually Means in the Spine
Before answering whether surgery limits it, it is worth being precise about what range of motion means in the context of the spine; because the word is used loosely in both clinical and patient-facing settings.
The spine’s total range of motion is not produced by any one segment. It is the sum of many small movements distributed across dozens of motion segments, each consisting of a disc anteriorly and two facet joints posteriorly. Flexion, extension, lateral bending, and rotation all result from the cumulative contribution of multiple levels working in concert.

When surgeons talk about “preserving range of motion,” they often mean preserving motion at a single level. One disc, one segment. The loss of motion at one segment does not necessarily produce a clinically obvious loss of total spinal range of motion in the early years after surgery. This is why patients who have single-level fusions often report that they “feel fine” with their motion for several years afterward.
What this framing misses is the long-term cost. When a segment is fused and stops moving, the adjacent segments must compensate. They absorb greater mechanical stress, experience accelerated degeneration, and at measurable rates in the published literature. Develop symptomatic disease that requires additional surgery. ¹ The question is not just whether you can still bend forward a year after surgery. The question is what happens to your adjacent segments over the following decade.
The distinction between early perceived motion and long-term structural consequence. Is the most important thing a patient can understand about the range-of-motion question.
The Three Categories of Spine Surgery and What Each Does to Motion
Not all spine surgery answers this question the same. The procedures that patients are typically offered fall into three categories with meaningfully different effects for your range of motion.
1. Fusion Surgery: Motion Is the Intended Casualty
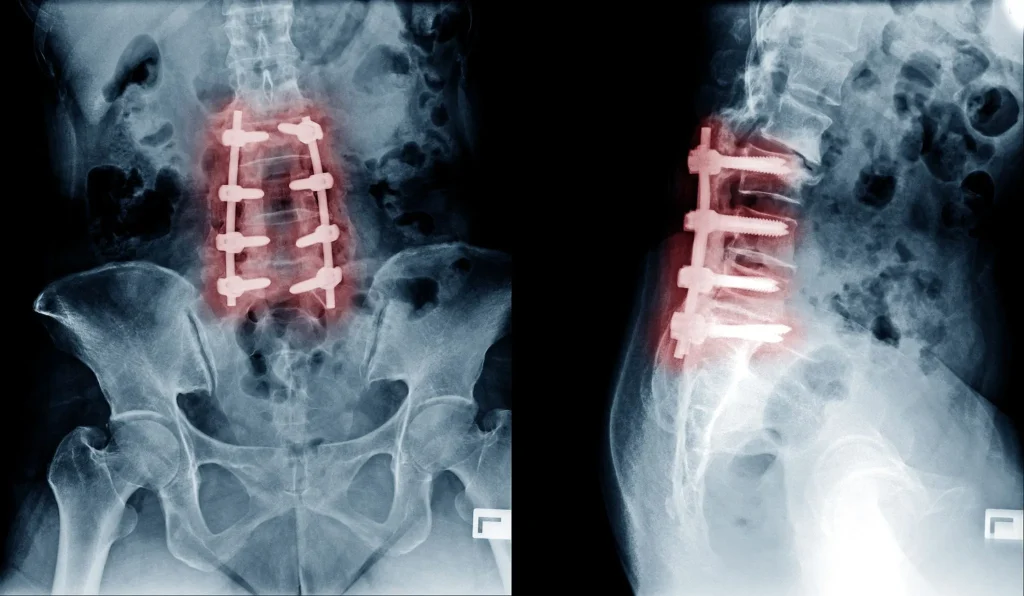
Spinal fusion is, by design, an operation that eliminates motion. The goal of the procedure is to cause two or more vertebrae to grow into a single rigid structure. This is achieved by removing the disc, placing bone graft or a cage implant in the disc space, and adding screws and rods to hold the segment still while the fusion solidifies.
Once successfully fused, the operated segment does not move. That is not a side effect. It is the mechanism. The loss of motion at the treated level is permanent and is what the surgeon is trying to achieve.
This is appropriate for a narrow set of conditions. Genuine mechanical instability, high-grade spondylolisthesis, vertebral fracture; where eliminating motion is the correct biological treatment. For the large proportion of patients told they need fusion for degenerative disc disease, herniated discs, or back pain without documented instability, the loss of motion is not clinically justified by the problem being treated.
The published literature on adjacent segment disease is consistent and sobering. A systematic review of 27 studies found adjacent segment degeneration rates of 5–18% over 4–14 years following lumbar fusion. ¹ Higher fusion levels, more segments fused, and younger patient age at the time of surgery all predict higher adjacent segment disease rates. A patient who has two or three segments fused in their 40s is not preserving any range of motion at those levels and the segments above and below are being placed under a long-term mechanical stress they were not designed to carry.
The clinical implication: a two-level lumbar fusion does not just limit your range of motion at two segments. It reorganizes the biomechanical load of your entire lumbar spine for the rest of your life.
2. Decompression Surgery: Motion Is Not Eliminated, But Altered
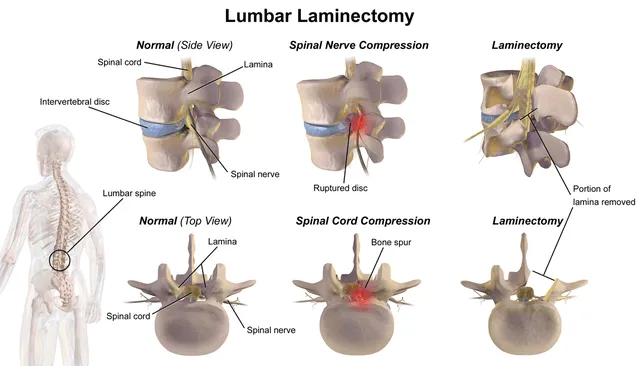
Decompression procedures: laminectomy, partial laminotomy, microdiscectomy, foraminotomy are different in kind from fusion. They do not involve implanting hardware or intentionally eliminating segmental motion. They remove bone, ligament, or disc material to relieve pressure on neural structures.
Decompression alone does not cause permanent fusion and does not, in a formal sense, eliminate range of motion. However, the tissue that is removed is not neutral to spinal biomechanics.
Laminectomy removes the posterior bony arch (the lamina) and often the interspinous ligament and facet joint cartilage. These are not passive structures; they constrain segmental motion, particularly extension and rotational movement, and provide posterior tension to stabilize the segment. Studies examining biomechanical outcomes after laminectomy have demonstrated increased segmental instability and altered motion at the operated level in a proportion of patients. ² In patients who develop post-laminectomy instability, surgeons frequently recommend a secondary fusion procedure. Which does eliminate motion.
The clinical scenario is not uncommon: a patient has a decompressive laminectomy, experiences relief for two to three years, develops progressive instability and recurrent symptoms, and is recommended a fusion at the same level. The motion that was preserved after the decompression is lost in the revision surgery.
Microdiscectomy carries a lower risk of secondary instability than full laminectomy, but carries a 7–15% recurrence rate for the disc herniation itself at 10 years, which creates its own pathway to additional surgery. ⁵
The takeaway: decompression surgery does not eliminate range of motion by design. But it alters the biomechanical substrate of the operated segment in ways that can lead to instability, recurrence, or progressive degeneration. And finally to a fusion recommendation and permanent loss of motion.
3. Disc Replacement: Motion Preservation in Theory and in Practice

Total disc replacement (TDR) was developed specifically to address the motion loss inherent to fusion. The logic is straightforward: replace the disc with an implant that allows the segment to continue moving, eliminate the long-term adjacent segment disease burden of fusion.
The evidence supports a partial version of this premise. A systematic review and meta-analysis of cervical disc replacement versus anterior cervical discectomy and fusion (ACDF) found that TDR produced a statistically higher range of motion at the operated level at 2 years, with lower rates of adjacent segment disease at 5 years. ³ Lumbar disc replacement shows a similar pattern in early-to-mid follow-up.
What the literature also shows is that the advantage narrows with time and comes with its own failure problems. Heterotopic ossification the spontaneous formation of bone around the implant. Occurs in a meaningful proportion of disc replacement patients and progressively reduces motion at the operated level, eventually producing a self-fusing segment without the surgical control of a formal fusion. ⁴ Implant wear, subsidence, and migration are additional failure modes that have no equivalent in fusion surgery.
A 2024 Cochrane review of lumbar disc replacement found moderate-quality evidence supporting TDR over fusion for short-term pain and disability, but noted high reoperation rates in several TDR series at 5–10 years, and significant heterogeneity across implant designs and patient populations. ⁶ The range-of-motion advantage of disc replacement over fusion is real but not as durable as early marketing suggested.
What “Motion Preservation” Actually Requires
If the goal is to treat spinal pain while preserving range of motion permanently. Not just in the first few postoperative years, but over the following decades. The requirements are specific.
The operation must not remove the disc. Fusion removes the disc and replaces it with a cage. Disc replacement removes the disc and replaces it with an implant. Both alter the motion segment permanently, one by eliminating motion, the other by substituting artificial motion for natural motion. Neither leaves the disc intact.
The operation must not place structural hardware. Screws, rods, cages, and artificial implants are permanent foreign objects that alter the biomechanics of the segments above and below, create infection risk, and have finite failure modes that often require reoperation.
The operation must not destroy the surrounding soft tissue. The paraspinal muscles, facet capsules, and interspinous ligaments that frame the motion segment are not decoration. They are active contributors to segmental stability and motion control. Operations that strip, cut, or permanently displace these structures alter motion biomechanics even when no fusion is performed.
By these criteria, a procedure that genuinely preserves range of motion in the long-term sense must leave the disc intact, place no hardware, and cause minimal disruption to the surrounding structural anatomy.
The Procedure That Most Precisely Meets This Standard

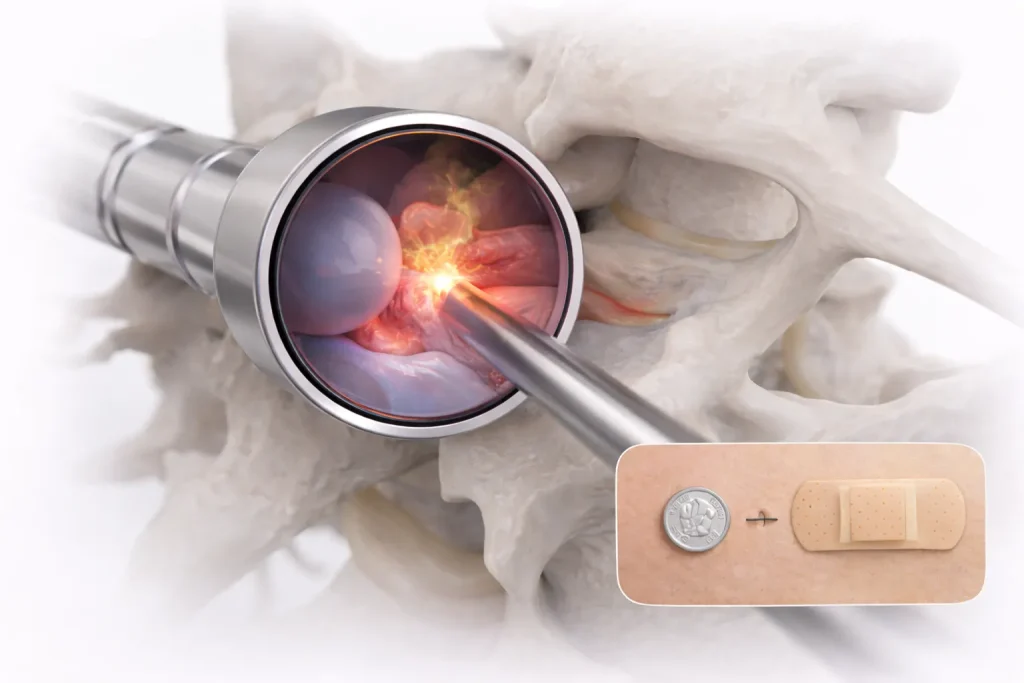
The Deuk Laser Disc Repair® (DLDR) was designed around exactly these principles. The procedure is performed through a 4 to 7 mm incision; roughly the diameter of a pencil eraser. Using a full-endoscopic approach. A precision laser is used to address the herniated nucleus material and the annular tear that is generating the pain. The disc is not removed. No fusion is performed. No implant is placed. No structural anatomy is altered.
Because nothing is removed and nothing is fused, there is no mechanism by which DLDR produces motion loss. The segment continues to move after the procedure the same way it did before with the source of pain fixed but the spine intact.
The published outcomes support this model. A peer-reviewed study of cervical DLDR in 66 consecutive patients found a 94.6% average symptom resolution rate, with 50% of patients reporting complete (100%) resolution of preoperative symptoms. The recurrent herniation rate was 1.5%. No major complications were reported. ⁷ Across more than 2,700 procedures over 20 years, the institutional track record shows a 99.6% success rate with zero reported complications. ⁸
Adjacent segment disease is the primary long-term consequence of motion loss from fusion. It has no mechanism to occur after DLDR because no segment is fused or mechanically loaded by the presence of hardware.
What Each Surgery Actually Does to Motion
What These Numbers Don’t Tell You
The “Small Incision” Framing Does Not Change the Operation
A minimally invasive fusion produces the same motion loss as an open fusion. The incision is smaller. The resulting biomechanics of the spine after the procedure. The rigidity at the fused segment, the increased stress on adjacent segments, the long-term adjacent segment disease risk. Are the same because the underlying operation is the same. A fusion performed through a small incision is still a fusion.

Patients should ask what is being done to their spine, not how large the incision is. Incision size affects recovery from the surgery. It does not affect what the surgery does to the spine’s long-term range of motion.
Motion-Preservation Claims Are Procedure-Specific
Disc replacement genuinely preserves range of motion better than fusion in the early postoperative years. That advantage is real and supported by the literature. What the marketing of disc replacement does not always acknowledge is that heterotopic ossification, implant wear, and other long-term failure problems can progressively reduce that advantage over time and that the implant itself is a permanent structural change to the spine with its own failure rates.
“Motion preservation” as a marketing claim needs to be evaluated against a specific procedure’s 5- and 10-year data, not just its 1- or 2-year results.
The Procedure That Was Recommended Is Not Necessarily the Only Option
The range-of-motion question cannot be separated from the question of whether the procedure being recommended is the correct one for the underlying pathology. A patient with discogenic pain from a contained herniated disc and an annular tear. Who is recommended for fusion is being offered a procedure that eliminates motion at a segment that does not require motion elimination. And that does so permanently, with the long-term adjacent segment disease consequences that follow.
Before consenting to any spine procedure that permanently alters motion, an independent review of whether that procedure is actually indicated for the specific pathology is not a delay in care. It is care.
The Bottom Line
Spine surgery will limit your range of motion permanently if the procedure being performed involves fusion. That statement is not a criticism of fusion as a concept for the narrow set of patients with genuine mechanical instability, fusion is the correct operation. But fusion is frequently recommended for conditions it is not designed to treat: herniated discs, discogenic pain, degenerative disc disease without instability.
For patients in that large category, the question is not whether to accept permanent motion loss as the cost of pain relief. It is whether a motion-preserving alternative to fusion exists for their specific anatomy.
Decompression surgery preserves motion better than fusion but alters the biomechanical foundation of the operated segment in ways that carry real risk of secondary instability and revision surgery. Disc replacement preserves more motion than fusion but involves a permanent implant with its own long-term failure rates. A full-endoscopic minimally invasive operation, when correctly indicated, treats the pain generator while leaving the disc, the surrounding anatomy, and the range of motion intact.
If a fusion is minimally invasive or open has been recommended to you for back or neck pain from a herniated disc. Submit your MRI for an independent review before consenting. The motion you preserve now is not recoverable after the surgery. The decision is permanent. The review is not.

Frequently Asked Questions
Will I be able to bend normally after spine surgery?
It depends on the procedure. After spinal fusion, bending at the fused level is permanently eliminated. Your lumbar or cervical spine will compensate by redistributing movement to adjacent segments. Which can feel normal in the short term but increases long-term degeneration risk. After decompression surgery without fusion, most patients retain full range of motion, though altered tissue mechanics can affect motion quality. After a full-endoscopic procedure that leaves the disc and anatomy intact, no functional range of motion is lost.
Does losing range of motion at one level actually affect my daily life?
Often not immediately. Single-level fusion patients frequently report no noticeable stiffness in the first few years because the adjacent segments compensate. The concern is long-term: the compensating segments absorb increased mechanical load and degenerate at measurably higher rates. At 5–14 years, adjacent segment disease requiring additional surgery occurs in 5–18% of fusion patients. ¹ That downstream cost is the clinical significance of the motion loss and not just the immediate stiffness.
Is disc replacement really better than fusion for preserving motion?
In the short term, yes. Peer-reviewed comparisons consistently show disc replacement produces greater range of motion at the operated level at 1–2 years and lower adjacent segment disease rates at 5 years compared to fusion. ³ However , heterotopic ossification can progressively reduce motion at the implant over time, and the implant itself creates long-term failure rates. From wear-and-tear, subsidence, migration, and potential revision. Disc replacement is a genuine improvement over fusion for appropriately selected patients; it is not a complete solution to the motion-preservation question.
Can I get my range of motion back after a fusion?
No. Fusion is irreversible. Once the segment has fused and the hardware is in place, the motion at that level is permanently eliminated. Subsequent surgeries can address adjacent segment disease or hardware complications but cannot restore motion to a successfully fused segment. This is the most important thing to understand before consenting to fusion: the decision is permanent.
Does a laminectomy permanently restrict my movement?
Not in the way a fusion does. Laminectomy removes posterior bone and soft tissue to relieve nerve compression, but does not inherently fuse the spine. However, the removal of the lamina and associated ligaments alters the segment’s biomechanical stability. In a proportion of patients, this contributes to post-laminectomy instability that eventually requires a fusion at the same level. Converting a motion-preserving decompression into a motion-eliminating stabilization procedure. The risk is greatest in patients with pre-existing instability or significant facet joint removal during the decompression.
What questions should I ask my surgeon about range of motion?
Ask four questions. First: does this procedure involve fusing any segment of my spine? Second: if fusion is recommended, what specifically in my anatomy makes instability the source of my pain rather than disc pathology alone? Third: if I have a herniated disc or annular tear, is there a disc-preserving alternative to fusion that has published peer-reviewed outcomes? Fourth: what is your personal reoperation rate and adjacent segment disease rate for this procedure at 5 and 10 years? If the answers are vague or the alternative-procedure question is dismissed, seek an independent review of your imaging before consenting.
What makes Deuk Laser Disc Repair® different from other motion-preserving surgeries?
Most “motion-preserving” spine procedures still remove the disc and replace it with something either a cage for a fusion or an artificial implant. Both alter the segment permanently. The Deuk Laser Disc Repair® is different because it does not remove the disc. It addresses the herniated nucleus and the annular tear through a 4–7 mm endoscopic incision, leaves the disc in place, places no hardware, and alters no structural anatomy. The operated segment retains its native motion because its native structure is retained. This is what motion preservation in the genuine sense of the term actually requires.
Sources
- Hashimoto K, et al. Adjacent segment degeneration after fusion spinal surgery: a systematic review. Int Orthop. 2019. https://pmc.ncbi.nlm.nih.gov/articles/PMC11605282/
- Hamasaki T, et al. Biomechanical assessment after partial facetectomy and laminectomy. Spine. 2009;34(2):E65–73. https://pubmed.ncbi.nlm.nih.gov/19112338/
- Yao QY, et al. Cervical TDR vs. ACDF: a meta-analysis of RCTs. Medicine. 2017;96(35):e7822. https://pubmed.ncbi.nlm.nih.gov/28858117/
- Hui N, et al. Cervical total disc replacement and heterotopic ossification: a review of literature outcomes and biomechanics. Asian Spine J. 2021;15(1):127–137. https://pubmed.ncbi.nlm.nih.gov/32050310/
- Weinstein JN, et al. Surgical vs. nonoperative treatment for lumbar disc herniation: SPORT trial. JAMA. 2006;296(20):2441–50. https://pubmed.ncbi.nlm.nih.gov/17119141/
- Jacobs WC, et al. Total disc replacement vs. fusion for cervical disc disease: a systematic review. Cochrane Database Syst Rev. 2024. https://www.cochranelibrary.com/
- Deukmedjian AJ, et al. Deuk Laser Disc Repair® for symptomatic cervical disc disease. Surg Neurol Int. 2013;4:68. https://pubmed.ncbi.nlm.nih.gov/23776754/
- Deuk Spine Institute. Deuk Laser Disc Repair® clinical outcomes data. https://deukspine.com/treatment-options/deuk-laser-disc-repair/
- Esposito F, et al. Open vs. minimally invasive surgery for thoracolumbar fractures: a systematic review. J Clin Med. 2024;13:5558. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11433229/
- Radcliff K, et al. Costs of cervical disc replacement vs. ACDF: Blue Health Intelligence analysis. Spine. 2015;40(8):521–29. https://pubmed.ncbi.nlm.nih.gov/25901961/


