

By Dr. Ara Deukmedjian, MD
Board-Certified Neurosurgeon, Deuk Spine Institute
Medically reviewed on January 20, 2026
Medical disclaimer: This content is for educational purposes only and does not constitute medical advice. Individual results may vary. Always consult with your healthcare provider about your specific condition and treatment options.

If you’ve been told you have a disc bulge at L3-L4, L4-L5, or L5-S1, you’re likely experiencing lower back pain, leg discomfort, or stiffness that’s affecting your daily life. Perhaps you’re worried about what this diagnosis means, whether you’ll need surgery, or if you’ll ever feel normal again.
Here’s something that might surprise you: Disc bulges are remarkably common, and not all of them cause pain. In fact, research shows that 30-84% of people (age dependent) without any back pain whatsoever have disc bulges visible on MRI scans.1 The presence of a bulge doesn’t automatically mean you’re destined for chronic pain or surgery.
What matters most is getting an accurate diagnosis that correlates your imaging findings with your actual symptoms, understanding all your treatment options, and making informed decisions about your care. This comprehensive guide will walk you through everything you need to know about L3-L4-L5 disc bulges, from what they are and why they happen, to conservative treatments and advanced surgical options.
Understanding L3-L4-L5 Disc Bulges: What’s Really Happening in Your Spine
Your lumbar spine consists of five vertebrae, labeled L1 through L5, with intervertebral discs sitting between each vertebra. These discs act as shock absorbers, allowing your spine to bend, twist, and move while protecting the vertebrae from grinding against each other.
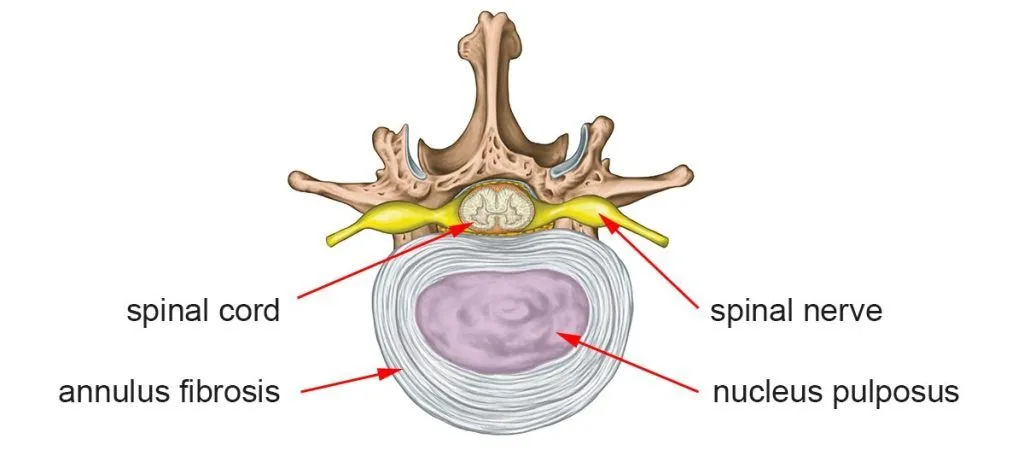
Each disc has two main components:
- The nucleus pulposus: A gel-like inner core that provides cushioning
- The annulus fibrosus: A tough outer ring of fibrous tissue that contains the nucleus
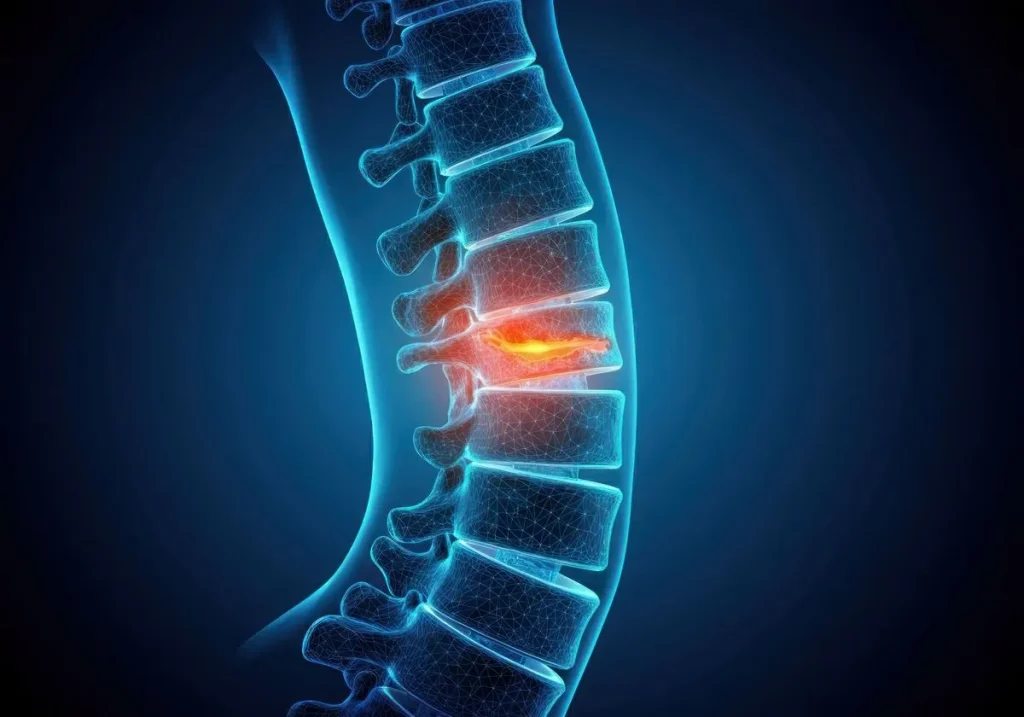
A disc bulge occurs when the disc extends beyond its normal boundaries without the outer layer rupturing completely. Think of it like a tire bulging outward but not yet flat. The disc material pushes outward in a broad, diffuse pattern, typically affecting 25% or more of the disc’s circumference.
How Common Are Disc Bulges?
Disc bulges are extraordinarily common, especially in the lower lumbar spine. The L3-L4, L4-L5, and L5-S1 levels bear the most mechanical stress during daily activities, making them the most frequent sites for disc problems.
A 2025 study examining the natural history of lumbar disc herniation found that disc abnormalities are present in a significant portion of asymptomatic individuals. By age 50, approximately 60% of people have disc bulges visible on imaging, yet many never experience symptoms. By age 60, that number increases to 80%.1
This is a crucial point that’s often misunderstood: The presence of a disc bulge on MRI does not mean you will have pain or need treatment. What matters is whether your specific bulge is causing symptoms, and if so, which symptoms it’s actually responsible for.
Disc Bulge vs. Herniated Disc: What’s the Difference?
The terms “disc bulge” and “herniated disc” are often used interchangeably, but they represent different stages of disc pathology:
Disc Bulge (Protrusion):
- The outer annulus remains intact but stretches outward
- The disc extends beyond its normal space in a broad, circumferential pattern
- Less likely to cause acute, severe symptoms
- May or may not compress nearby nerves
Herniated Disc (Extrusion):
- The outer annulus develops a tear or rupture
- The inner nucleus pulposus leaks out through the tear
- More likely to cause severe, acute symptoms
- The extruded material is highly inflammatory and can chemically irritate nearby nerves
Both conditions exist on a spectrum of disc degeneration. A bulge can progress to a herniation, though this doesn’t always happen. What’s important to understand is that both can cause similar symptoms, and both can be treated effectively when properly diagnosed.2
Why Disc Bulges Don’t Always Cause Pain: The Inflammation Connection
One of the most important concepts in understanding disc-related pain is this: Compression alone doesn’t cause most back pain; inflammation does.
For decades, the medical community believed that disc bulges caused pain primarily through mechanical compression of nerve roots. While nerve compression can certainly cause symptoms, recent research has fundamentally changed our understanding of disc pain.
At Deuk Spine Institute, our research and clinical experience with thousands of patients show that the pain from disc problems isn’t caused by simple mechanical pinching of the nerve. Instead, it’s the inflammation triggered by disc material that irritates nearby structures, causing persistent pain and neurological symptoms.3
The Chemical Inflammation Process
When a disc degenerates, develops an annular tear, or bulges significantly, inflammatory chemicals are released into the surrounding tissues. These chemical mediators include:
- Prostaglandins
- Cytokines (particularly TNF-alpha and IL-6)
- Proteolytic enzymes
- Substance P
These inflammatory substances sensitize nerve endings, causing pain even without significant mechanical compression. This explains why some people with large disc bulges have minimal symptoms, while others with relatively small bulges experience debilitating pain; the level of inflammation varies considerably between individuals.
A 2023 study on treatments for lumbar disc herniation confirmed that addressing inflammation, rather than just mechanical decompression, is crucial for successful outcomes.4
This understanding has profound implications for treatment: therapies that reduce inflammation (whether through medications, injections, or surgical removal of inflammatory tissue) often provide better relief than mechanical decompression alone.
Common Causes and Risk Factors for L3-L4-L5 Disc Bulges
While disc degeneration is a natural part of aging, several factors accelerate the process and increase your risk of developing symptomatic disc bulges:
Age-Related Degeneration
The most common cause of disc bulges is degenerative disc disease. As we age, several changes occur in our spinal discs:
- Water content decreases: Discs lose their hydration, becoming less flexible and more prone to injury
- Height loss: Dehydrated discs lose height, altering spinal mechanics
- Weakened annulus: The outer ring becomes less resilient and more susceptible to tears
- Reduced nutrient supply: Blood flow to discs decreases with age, impairing healing capacity
Recent research from 2025 examining spontaneous disc resorption mechanisms found that age-related changes affect not only disc structure but also the body’s ability to naturally heal and reabsorb herniated material.
Mechanical Stress and Trauma
Certain activities and events place excessive stress on lumbar discs:
- Heavy lifting: Improper lifting technique, especially with twisting motions, creates enormous pressure on L3-L4-L5 discs
- Repetitive bending: Occupations requiring frequent forward bending accelerate disc wear
- Prolonged sitting: Sitting increases intradiscal pressure by up to 40% compared to standing
- Acute trauma: Car accidents, falls, or sports injuries can cause sudden disc damage
- Vibration exposure: Long-distance truck drivers and heavy equipment operators face a higher risk
Lifestyle and Genetic Factors
Several modifiable and non-modifiable factors influence disc health:
- Obesity: Excess body weight increases the mechanical load on lumbar discs
- Smoking: Nicotine impairs blood flow to discs, accelerating degeneration
- Physical inactivity: Weak core muscles fail to support the spine adequately
- Genetics: Family history of disc problems increases individual susceptibility
- Poor posture: Chronic postural imbalances create uneven disc loading
- Occupation: Physically demanding jobs with heavy lifting increase risk
Understanding these risk factors helps inform both treatment and prevention strategies.

Recognizing Symptoms: When Should You Be Concerned?
Symptoms from L3-L4-L5 disc bulges vary dramatically depending on several factors: the size and location of the bulge, whether it compresses a nerve root, the degree of inflammation, and individual pain sensitivity.
Localized Back Pain
The most common symptom is lower back pain that may feel like:
- A dull, constant ache in the lumbar region
- Sharp pain with certain movements (bending, twisting, lifting)
- Stiffness, especially after periods of inactivity
- Pain that worsens with prolonged sitting or standing
This localized pain typically results from inflammation in the disc itself (discogenic pain) or irritation of nearby structures.
Radicular Pain (Sciatica)
When a disc bulge compresses or irritates a nerve root, pain can radiate into the leg, a condition called radiculopathy or sciatica. The specific pattern depends on which nerve root is affected:
L3-L4 disc bulge (affecting L4 nerve root):
- Pain radiating down the front of the thigh
- Numbness along the inner shin
- Weakness in straightening the knee
- Diminished knee-jerk reflex
L4-L5 disc bulge (affecting L5 nerve root):
- Pain traveling down the outer thigh and leg
- Numbness on top of the foot and between the first and second toes
- Weakness lifting the foot upward (foot drop)
- Difficulty walking on heels
L5-S1 disc bulge (affecting S1 nerve root):
- Pain down the back of the thigh and calf
- Numbness on the bottom of the foot and outer toes
- Weakness pushing up on tiptoes
- Diminished ankle-jerk reflex
According to research published in the British Medical Journal, the defining characteristic that separates sciatica from general low back pain is pain radiating below the knee and into the foot and toes.5 This specific distribution indicates more significant nerve involvement.
For more detailed information about sciatica patterns and their significance, see our comprehensive guide on sciatica causes and treatment.6
Neurological Symptoms
When nerve compression is significant, additional symptoms may develop:
- Tingling or “pins and needles” sensation in the leg or foot
- Numbness that persists or worsens over time
- Muscle weakness affecting specific movements
- Loss of reflexes in the knee or ankle
- In severe cases, bowel or bladder dysfunction (a medical emergency)
Pain Patterns and Triggers
Understanding what makes your pain better or worse provides diagnostic clues:
Pain typically worsens with:
- Prolonged sitting (increases intradiscal pressure)
- Forward bending
- Coughing, sneezing, or straining
- Transitioning from sitting to standing
- Long-distance walking or standing
Pain typically improves with:
- Lying down (reduces disc pressure)
- Walking short distances (promotes circulation)
- Changing positions frequently
- Gentle stretching
The Importance of Accurate Diagnosis: Why Correlation Matters
One of the most critical aspects of treating disc bulges successfully is ensuring that your diagnosis correlates with your imaging findings and your clinical symptoms. This correlation is absolutely essential, yet it’s frequently overlooked.
Why Imaging Alone Isn’t Enough
Here’s a scenario I encounter regularly in my practice: A patient presents with lower back pain. An MRI shows a disc bulge at L4-L5. The patient is told, “You have a bulging disc, that’s why you have pain.” Treatment is recommended based on the MRI findings.
The problem? This approach assumes the disc bulge seen on MRI is causing the patient’s symptoms. But as we discussed earlier, disc bulges are extremely common in people without pain. The bulge might be an incidental finding unrelated to the patient’s symptoms.
A 2025 systematic review on the management of lumbar disc herniation highlighted a significant lack of standardization in surgical decision-making. The study found that while imaging-confirmed nerve root compression and refractory pain are consistent surgical indications, there is high variability in how motor and sensory deficits are defined.7
The Three-Part Diagnostic Approach
Accurate diagnosis requires three components working together:
1. Clinical History:
- When did the pain start?
- What activities worsen or improve it?
- Is pain getting better, worse, or staying the same?
- Have you had similar episodes before?
- What treatments have you tried?
2. Physical Examination:
- Range of motion testing
- Neurological examination (strength, sensation, reflexes)
- Provocative tests (straight leg raise, femoral nerve stretch)
- Palpation for areas of tenderness
- Gait assessment
3. Imaging Studies:
- MRI showing the location, size, and type of disc abnormality
- Correlation between imaging findings and physical examination
- Assessment of other potential pain sources
Only when all three components align (i.e., your symptoms match the physical examination findings, which in turn match the imaging abnormalities) can we confidently identify the source of your pain.
The Value of a Second Opinion
Given the complexity of diagnosing disc-related pain and the significant variation in treatment recommendations among spine specialists, seeking a second opinion is often valuable. This is especially true if:
- You’ve been recommended for surgery, but have questions about whether it’s necessary
- Conservative treatments haven’t provided relief, but you’re unsure about next steps
- Your diagnosis seems unclear or doesn’t match your symptoms
- You want to explore all treatment options, including minimally invasive approaches
A second opinion can provide:
- Confirmation that your diagnosis is correct
- Alternative perspective on treatment options
- Identification of overlooked factors contributing to your pain
- Peace of mind that you’re making an informed decision
At Deuk Spine Institute, we offer free MRI reviews and virtual consultations to provide patients with expert second opinions. This service has helped countless patients avoid unnecessary procedures and find effective treatments they didn’t know existed.
Upload your latest MRI to schedule your time with Dr. Ara Deukmedjian now.
Diagnostic Testing: What to Expect
When you see a spine specialist for a suspected disc bulge, several tests may be used to confirm the diagnosis and assess the severity of your condition.
Magnetic Resonance Imaging (MRI)
MRI is the gold standard for visualizing disc bulges and herniations. It provides detailed images of soft tissues, including:
- The discs themselves (showing bulges, herniations, or degeneration)
- Nerve roots (showing compression or inflammation)
- The spinal canal (showing stenosis if present)
- Surrounding ligaments and muscles
MRI allows physicians to see:
- The exact location and size of disc abnormalities
- Whether nerve roots are being compressed
- The degree of disc degeneration
- Other potential pain sources
X-Rays
While X-rays cannot visualize discs directly (they only show bones), they provide valuable information:
- Vertebral alignment
- Disc space height (indirect measure of disc degeneration)
- Bone spurs that might contribute to nerve compression
- Overall lumbar spine curvature
- Signs of instability with flexion-extension views
CT Scans
Computed tomography offers excellent bony detail and may be useful when:
- MRI is contraindicated (for patients with certain metal implants)
- Evaluating bone spurs or foraminal narrowing
- Surgical planning requires precise visualization of bony anatomy
Electrodiagnostic Studies (EMG/NCS)
These tests measure electrical activity in muscles and nerves:
- Confirm the presence and severity of nerve root compression
- Identify which specific nerve root is affected
- Distinguish lumbar radiculopathy from peripheral nerve problems
- Assess the chronicity and severity of nerve damage
EMG/NCS testing is particularly valuable when clinical symptoms don’t clearly match imaging findings.
Conservative Treatment Options: The First Line of Defense
For most patients with L3-L4-L5 disc bulges, an initial trial of conservative treatment is appropriate and often successful. Recent research indicates that patients with lumbar disc problems can improve with comprehensive conservative care.
The keyword here is “comprehensive.” Not all conservative treatments are equally effective, and the quality of implementation matters significantly.
Medications for Pain and Inflammation Management
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs):
Medications like ibuprofen, naproxen, or celecoxib help reduce inflammation and pain. They work best when used regularly during flare-ups rather than only when pain is severe. However, long-term use carries risks including gastrointestinal problems and cardiovascular concerns.
Acetaminophen:
This pain reliever can be helpful for mild to moderate pain, particularly when combined with other treatments. It doesn’t reduce inflammation but can improve pain tolerance.
Muscle Relaxants:
Medications such as cyclobenzaprine or methocarbamol can help reduce muscle spasms that often accompany disc problems, improving mobility and comfort.
Corticosteroids:
Oral steroids may be prescribed for short-term use during severe flare-ups to rapidly reduce inflammation.
Important note: While opioid medications may provide short-term relief for acute pain, they are not recommended for long-term management of chronic disc pain due to risks of dependence and limited long-term effectiveness.
Physical Therapy and Exercise
A well-designed physical therapy program is one of the most effective conservative treatments for disc bulges. A 2025 meta-analysis published in Frontiers in Medicine found that exercise therapy significantly improves pain, disability, range of motion, and quality of life in patients with lumbar disc herniation.
An evidence-based program might include:
Core Strengthening:
Building strength in abdominal and back muscles provides better support for the spine, reducing stress on discs. However, it’s crucial to perform exercises correctly as improper core work can worsen disc problems.
Flexibility Training:
Gentle stretching of tight muscles, particularly hip flexors, hamstrings, and lumbar paraspinals, can improve movement patterns and reduce strain on the lower back.
Nerve Gliding Exercises:
Specific movements that help nerves move more freely through surrounding tissues, potentially reducing radicular symptoms.
Postural Training:
Learning proper body mechanics for daily activities helps minimize disc stress. This includes proper lifting technique, sitting posture, and sleeping positions.
Manual Therapy:
Hands-on techniques by a physical therapist can help improve joint mobility and reduce muscle tension.
The effectiveness of physical therapy depends heavily on the quality of the program and patient compliance. Working with a therapist who specializes in spinal conditions and has experience treating disc problems is essential.
Activity Modification and Lifestyle Changes
Avoid aggravating activities:
Limit heavy lifting, repetitive bending, and prolonged sitting while your disc heals. This doesn’t mean complete rest—remaining moderately active is important.
Maintain a healthy weight:
For overweight individuals, losing even 5-10% of body weight can significantly reduce the mechanical load on lumbar discs and improve symptoms.
Smoking cessation:
Quitting smoking improves blood flow to discs, enhancing healing capacity and slowing degeneration.
Ergonomic modifications:
Adjust workstations, use lumbar support when sitting, and ensure proper mattress support for sleeping.
Stay active:
Low-impact activities like walking, swimming, or cycling help maintain disc nutrition and overall spinal health.
Tip: Addressing multiple factors, such as exercise, activity modification, and lifestyle changes, can produce better outcomes than single interventions alone.
Injection-Based Therapies
When oral medications and physical therapy provide insufficient relief, several injection options may be considered:
Epidural Steroid Injections (ESIs):
These involve injecting corticosteroid medication and local anesthetic into the epidural space around inflamed nerve roots. ESIs can reduce inflammation and provide pain relief lasting weeks to months in some patients.
However, limitations exist:
- Relief is often temporary (3-6 months on average)
- Repeated injections may weaken bone and soft tissues
- They don’t address the underlying disc problem
- Not all patients respond favorably
Selective Nerve Root Blocks:
These more targeted injections deliver medication directly around specific nerve roots, both for diagnosis and treatment.
Platelet-Rich Plasma (PRP) Injections:
PRP injections are currently being explored as a viable regenerative treatment for disc problems.
When Conservative Treatment Isn’t Working
You may need to consider more advanced interventions if:
- Pain persists after 6-12 weeks of appropriate conservative care
- Symptoms are progressively worsening
- You develop new neurological symptoms (weakness, numbness)
- Quality of life is severely impacted despite conservative treatment
- Bowel or bladder dysfunction develops (requires immediate evaluation)
Patient Story: A Day-and-Night Transformation
A mother of three from Pennsylvania had been bedridden since December, sidelined by a herniated disc at L5-S1 that was pinching the nerve down her leg. She had tried everything: physical therapy, chiropractic care, pain medication, even at-home McKenzie exercises. “Nothing would alleviate my pain,” she recalls.
Traditional surgery scared her. She had watched her father struggle through months of recovery after a spinal fusion, and as a busy mom, she couldn’t afford that. “There’s no way. I have three kids,” she remembers thinking.
Her answer came from an unexpected place. While searching YouTube, she found a Deuk Spine testimonial, then started watching Dr. Deukmedjian’s live surgeries and asking questions in real time. Convinced, she submitted her MRI and traveled from Pennsylvania to Florida for Deuk Laser Disc Repair®.
Just twelve hours after her procedure at L5-S1, the change was undeniable. “It’s literally a day-and-night transformation,” she says. The morning after surgery she was up walking, doing her hair, and smiling. The day before, she had been in tears. “I’m so grateful. I feel like my prayers have been answered.”
Asked if she’d do it again, her answer was instant: “One thousand percent.”
Watch Her Full Testimonial
Surgical Treatment Options: When Is Surgery Necessary?
Surgery for L5-S1 disc bulges is considered when:
- Conservative treatments have been exhausted (typically 6-12 weeks of appropriate care)
- Progressive neurological deficits develop
- Severe, unrelenting pain significantly impacts quality of life
- Cauda equina syndrome develops (a surgical emergency)
Traditional Surgical Approaches
Microdiscectomy:
This procedure involves removing the portion of disc material that’s compressing a nerve root. It’s performed through a small incision using microscopic visualization. While generally effective for appropriate candidates, traditional microdiscectomy often requires cutting through muscle and sometimes removing bone to access the disc, which can weaken spinal structures.
Laminectomy:
This surgery removes a portion of the vertebral bone (lamina) to create more space for compressed nerves. It’s often performed when disc bulges contribute to spinal stenosis. However, removing bone can compromise spinal stability.
Spinal Fusion:
When disc degeneration is severe or instability exists, fusion surgery may be recommended. This involves permanently joining two or more vertebrae together using bone grafts and hardware (screws and rods).
However, fusion comes with significant drawbacks:
- Eliminates motion at the fused segment
- Places increased stress on adjacent levels, potentially accelerating their degeneration (adjacent segment disease)
- Requires longer recovery time
- Higher complication rates
- Permanent alteration of spinal mechanics
Advanced Minimally Invasive Option: Deuk Laser Disc Repair®
At Deuk Spine Institute, we’ve developed an advanced alternative that addresses disc problems while preserving your spine’s natural structure and function.
Deuk Laser Disc Repair® (DLDR) is a minimally invasive endoscopic procedure that removes only the inflamed, damaged portion of the disc while leaving healthy disc tissue intact. Unlike fusion, DLDR® requires no screws, rods, or metal implants.
How the procedure works:
- A tiny incision (less than ¼ inch) is made
- A tubular retractor gently spreads muscle to create a surgical corridor
- An endoscopic camera provides visualization
- A medical laser precisely removes only the inflammatory disc tissue through the annular tear
- The healthy disc structure remains intact, preserving natural spinal motion
Key advantages of DLDR®:
- Outpatient procedure: Patients go home the same day
- Rapid recovery: Most patients return to light activities within days, not months
- No fusion: Natural spinal motion is preserved
- No bone removal: Spinal stability remains intact
- Minimal scarring: Less than ¼ inch incision
- High success rate: 95% success rate in over 1,300 procedures with zero complications
Recovery timeline:
- Walking within an hour of the procedure
- Light activities within 1-2 weeks
- Return to work within 2-3 weeks for desk jobs
- Full recovery typically within 4-6 weeks
To learn more about whether you’re a candidate for Deuk Laser Disc Repair®, visit our treatment page.
Prevention Strategies: Protecting Your Spine Long-Term
Whether you’ve already experienced disc problems or want to prevent them, these strategies can help protect your lumbar spine:
Core Strengthening
Strong core muscles offload pressure from your discs. Effective exercises include:
- Planks (when appropriate for your condition)
- Bird-dogs
- Dead bugs
- Bridge variations
- McGill Big 3 exercises
Work with a physical therapist to ensure proper form. Remember, incorrect technique can worsen disc problems.
Proper Body Mechanics
Lifting technique:
- Bend at the knees, not the waist
- Keep the object close to your body
- Avoid twisting while lifting
- Use your legs to generate power
Sitting posture:
- Use lumbar support
- Keep feet flat on the floor
- Take frequent breaks to stand and move
- Adjust the desk and monitor height appropriately
Sleeping positions:
- Side sleeping with a pillow between the knees
- Back sleeping with a pillow under the knees
- Avoid stomach sleeping
Nutrition and Hydration
Discs rely on fluid exchange for nutrition. Adequate hydration supports disc health. Anti-inflammatory foods (leafy greens, fatty fish, nuts, berries) may help reduce systemic inflammation.

Regular Exercise
Low-impact activities like walking, swimming, or cycling help maintain disc nutrition, core strength, and overall spinal health. Aim for 150 minutes of moderate activity weekly.

Frequently Asked Questions
-
How long does it take for a disc bulge to heal naturally?
The natural history of disc bulges varies considerably. Many improve within 6-12 weeks with appropriate conservative treatment. However, “healing” doesn’t mean the bulge completely disappears; rather, inflammation resolves and symptoms improve. Recent research on spontaneous disc resorption found that some disc material can naturally reabsorb over 3-6 months, particularly with larger herniations and extrusions.8 Smaller bulges may persist on imaging even after symptoms resolve. The key is symptom improvement, not necessarily complete resolution of the bulge on MRI.
-
Can I exercise with a disc bulge, or will it make things worse?
The right exercises, properly performed, will not make a disc bulge worse and can actually accelerate recovery. However, certain movements should be avoided, especially during acute pain:
- Avoid: Heavy lifting, deep forward bending, high-impact activities, exercises that cause pain
- Beneficial: Walking, swimming, gentle stretching, proper core stabilization exercises, nerve gliding exercises
The key is working with a physical therapist who understands disc pathology to develop an appropriate, progressive exercise program. A 2025 meta-analysis confirmed that exercise therapy is safe and effective for patients with lumbar disc herniation when properly prescribed and supervised.9
-
How do I know if my disc bulge requires surgery?
Surgery is typically considered when:
- You’ve exhausted 6-12 weeks of appropriate conservative treatment without adequate improvement
- You have progressive weakness (like foot drop) that’s getting worse
- You develop bowel or bladder dysfunction (a surgical emergency)
- Your pain is so severe that it prevents you from performing essential daily activities and work
- Imaging clearly shows significant nerve compression that correlates with your symptoms
However, even when these criteria are met, minimally invasive options like Deuk Laser Disc Repair® often provide excellent outcomes without the risks and prolonged recovery of traditional fusion surgery. Getting a second opinion from a specialist experienced in both conservative and minimally invasive approaches ensures you understand all your options.
-
Will my disc bulge show up on an X-ray?
No, disc bulges cannot be seen directly on X-rays because X-rays only visualize bones, not soft tissues like discs. However, X-rays can provide indirect evidence of disc problems:
- Reduced disc space height (suggesting disc degeneration)
- Bone spurs that may have developed due to chronic disc problems
- Vertebral alignment abnormalities
- Signs of instability
An MRI is the gold standard for visualizing disc bulges, herniations, and their effect on surrounding nerves. If your doctor orders only X-rays when you have symptoms suggesting a disc problem, you may want to request an MRI for a more accurate diagnosis.
Key Takeaways: What You Need to Remember
If you’re dealing with a disc bulge at L3-L4, L4-L5, or L5-S1, here are the most important points to remember:
- Disc bulges are extremely common: Up to 80% of people over 60 have disc bulges visible on MRI, yet many experience no pain. The presence of a bulge doesn’t automatically mean you need treatment.
- Accurate diagnosis requires correlation: Imaging findings must match your symptoms and physical examination. Don’t accept treatment recommendations based on MRI alone without thorough clinical evaluation.
- Inflammation drives pain, not just compression: Understanding that chemical inflammation is often more important than mechanical pressure helps explain why anti-inflammatory treatments (whether conservative or surgical) are often most effective.
- Most cases improve with conservative care: Many patients with disc problems improve with comprehensive conservative treatment, including physical therapy, medications, activity modification, and time.
- Not all disc bulges are the same: A bulge that causes no symptoms requires no treatment. A bulge causing mild pain may respond to conservative care. A bulge causing progressive neurological symptoms may require intervention.
- Modern treatment options preserve your spine: If surgery becomes necessary, minimally invasive procedures like Deuk Laser Disc Repair can address the problem while preserving natural spinal motion and stability, avoiding the risks and limitations of fusion.
- Second opinions matter: Given the significant variation in treatment recommendations and the life-changing impact of spine surgery, seeking expert second opinions helps ensure you’re making the best decision for your specific situation.
- Recovery is possible: Whether through conservative treatment or advanced minimally invasive surgery, the vast majority of patients with L3-L4-L5 disc bulges can achieve significant pain relief and return to active, fulfilling lives.
If you’re experiencing symptoms from a disc bulge, don’t wait for the problem to worsen. Early, appropriate treatment provides the best chance for rapid recovery and prevents the development of chronic pain patterns. At the same time, don’t rush into surgery without exploring all your options and ensuring your diagnosis is accurate.
At Deuk Spine Institute, we’re committed to providing honest, evidence-based assessments and offering the full spectrum of treatment options, from conservative care to the most advanced minimally invasive procedures available. We offer free MRI reviews and virtual consultations to help you understand your diagnosis and explore all available treatment paths.
Upload your MRI for a free review and personal consultation with Dr. Ara Deukmedjian, founder of Deuk Spine Institute and creator of the Deuk Laser Disc Repair® procedure. Take the first step toward lasting relief and a return to the activities you love.
Sources
1: https://pmc.ncbi.nlm.nih.gov/articles/PMC4464797
2: https://deukspine.com/blog/herniated-disc-mri
3: https://deukspine.com/blog/what-is-causing-my-sciatica
4: https://pmc.ncbi.nlm.nih.gov/articles/PMC10888666
5: https://pmc.ncbi.nlm.nih.gov/articles/PMC1895638/
6: https://deukspine.com/blog/sciatica-surgery-overview
7: https://www.sciencedirect.com/science/article/pii/S2772529425014389
8: https://www.frontiersin.org/journals/medicine/articles/10.3389/fmed.2025.1633762/full


